Medizinische Universität Innsbruck - Prhoinsa
186
Medizinische Universität Innsbruck Universitätsklinik für Kinder- und Jugendheilkunde Abteilung für Neonatologie ELECTRICAL IMPEDANCE SEGMENTOGRAPHY : REGIONAL LUNG VENTILATION IN INFANTS DISSERTATION Zur Erlangung des akademischen Grades Doktor der gesamten Heilkunde an der medizinischen Universität Innsbruck Betreuer: Univ.-Prof. Dr. Georg Simbruner Vorgelegt von Judith C. Weinknecht Innsbruck, Juni 2009
Transcript of Medizinische Universität Innsbruck - Prhoinsa
Medizinische Universität Innsbruck
Universitätsklinik für Kinder- und Jugendheilkunde Abteilung für Neonatologie
ELECTRICAL IMPEDANCE SEGMENTOGRAPHY:
REGIONAL LUNG VENTILATION IN INFANTS
DISSERTATION
Zur Erlangung des akademischen Grades
Doktor der gesamten Heilkunde
an der medizinischen Universität Innsbruck Betreuer: Univ.-Prof. Dr. Georg Simbruner
Vorgelegt von
Judith C. Weinknecht
Innsbruck, Juni 2009

2
Eidesstattliche Erklärung Ich erkläre hiermit an Eides Statt, dass ich die vorliegende Arbeit selbständig sowie ohne
unzulässige Hilfe Dritter und ohne Benutzung anderer als der angegebenen Hilfsmittel
angefertigt habe. Die aus anderen Quellen direkt oder indirekt übernommenen Daten und
Konzepte sind unter Angabe der Quelle gekennzeichnet.
Die Arbeit wurde bisher weder im In- noch im Ausland in gleicher oder ähnlicher Form einer
anderen Prüfungsbehörde vorgelegt.
Innsbruck, am 01. Juli 2009
3
Dedicated to Andreas

4
Quand tu veux construire un bateau, ne commence pas par rassembler du bois, couper des planches et distribuer du
travail, mais réveille au sein des hommes le désir de la mer grande et large.
Antoine de Saint- Exupéry
5
Acknowledgements
It has been a three and a half years endeavour from the very beginning of this work until its
completion. I have achieved my aim and hence I would like to deeply thank various people
who - during the years and months in which this endeavour lasted - provided me with useful
and helpful assistance. Without their care and consideration, this doctoral thesis would not
have matured.
Most importantly I am indebted to my “Doktorvater” Univ.-Prof. Dr. Georg Simbruner,
who has been much more than a supervisor of this work. In him I have found encouragement,
enthusiasm and numerous ideas in scientific questions. His dedication and interest in this
work is ever-lasting. Furthermore his charismatic personality and his inspiration shaped me in
a way I will never forget and will influence my career in neonatology. Dit het baie vir my
beteken om jou te ontmoet.
I am deeply grateful to Dr. Salvador Navarro-Psihas who supported me during my clinical
examinations without reserve. His never-ending patience in answering my medical questions
and his personal support as well as his severe interest in the care of newborns showed me a
role model of a good doctor.
Of crucial importance for the success of this work was the support of the Neonatal Intensive
Care Unit Staff and Intermediate Care Unit Staff, mainly the nurses who warmly
welcomed me on their team, introduced me into their daily routine and implied me and my
clinical trial into their daily work. Furthermore I am truly thankful for the cooperation of the
attendings in the NICU, namely Univ.-Prof. Dr. Rudolf Trawöger, Univ.-Prof. Dr. Ursula
Kiechl-Kohlendorfer, Univ.-Prof. Dr. Elisabeth Steichen-Gersdorf, Dr. Gernot Reiter,
Dr. Erika Pastner, and Dr. Uwe Klingkowski for their long-lasting support during my
examinations on their wards.
Special thanks to Dr. Wolfgang Wetsch for introducing me to the depths of anaesthesiology
and mechanical ventilation as well as his severe interest in my investigations. His ideas in
electrical impedance measurements and knowledge of mechanical ventilation have always
been - literally - “inspirations” to this work.
I am very grateful to Dr. Andreas Mühlig-Hoffmann for ever introducing me into the field
of neonatology and to share his fascination for infants with me.

6
I would like to thank Univ.-Prof. Dr. Johannes Pöschl for giving me the chance to work
independently with newborns during my rotation in Heidelberg. I’ve truly learned how to
handle infants and to be responsible for my work, a skill which I could use during my
examinations in our NICU.
My sincere thanks to Elvira Parravicini, M.D. who showed me during my stay in New York
that caring of newborns is much more than providing medicine, doing everything we can do,
but make decisions based on the infants’ needs and she truly cared about the well-being of
both infants and their parents.
I am very grateful to Dr. Audrey Bekker for teaching me so intensely the secrets of neonatal
care during my medical elective in South Africa, at the same time introducing me into a
completely different world of neonatal care and showing me many ways of excellent newborn
treatment, experiences which clearly inspired this work and will affect my further neonatal
education.
I am very thankful to Mag. Heike Dusik who helped me through all the bureaucratic work to
get the medical devices by the responsible authorities approved, as well as her personal
support through the entire time of this work.
He was the most reliable man in this project, Dipl.-Ing. Herbert Bauer, who introduced me
to the fascinating world of electrical impedance measurements, guided me through the
technical tasks during my examinations, realized plenty of our ideas, and always did his work
with great joy. I have learned to appreciate his effort and I have always enjoyed his fabulous
humour.
My sincere thanks to Alfred Ortner, EMS Biomedical Handels.gesmbH, Korneuburg who
sponsored the electrical impedance device I have employed during my measurements.
I am very thankful to Ing. Hans Redl on behalf of Chemomedica, Medizintechnik und
Arzneimittel Vertriebsges.m.b.H, Vienna for sponsoring the self-adhesive electrodes we have
applied during our measurements.
In the beginning of this study Univ.-Prof. Dr. Mario Rüdiger and Dr. Wolfram Burkhardt
introduced me to real-life measurements with our electrical impedance device while they were
working on their animal experiments. They both clearly and well demonstrated the fascination
of this new method.
My deepest thanks go to Andreas Lebesmühlbacher who truly had the best explanations for
every single medical phenomenon I have ever experienced. He did not only visualize each and
every thought I’ve had, he did it with plenty of joy and in a loveable way and mostly on a
daily basis.
7
During the last months of my endeavours Daniel Asnes, M.D. gave me wonderful and never-
ending support through the final hoops I had to jump through. His unique character is
fascinating and his personality inspiring in both the medical field and personally.
I am grateful to my sisters Mag. Kora Weinknecht and Hannah Weinknecht who both
helped me with their great skills, Kora mostly showed me the depths of correctly done
scientific work and statistics, Hannah introduced me patiently to the depths of the English
language, and both guided me through numerous technical and computer related topics.
Personal thanks for their support and understanding go to all of my friends and family, who
followed me through this work and did it with great care, namely Dr. Martina Zechmann,
Dr. Silke Dormeier, Dr. Alexander Varga, Dr. Marion Domby, Dr. Marion Welzel,
Dr. in spe Juliana Oberdanner, Dr. Thomas Hager, Mag. Ingrid Mantl, Theresia
Wenisch, Paul Sauer PhD and my dearest little Felicia Stadler.
Traditionally at the end but not less important is the constant support of my parents Dipl.-Ing.
Paul Weinknecht and Mag. Christa Weinknecht during the entire time I have spent on this
work.
8
EIDESSTATTLICHE ERKLÄRUNG ................................................................................... 2
ACKNOWLEDGEMENTS ..................................................................................................... 5
I. INTRODUCTION .............................................................................................................. 10 1.1 MEDICAL BACKGROUND - NEONATAL RESPIRATORY AND CARDIAC DISEASES .......................................... 12
1.1.1 Clinical Features in Infants with Respiratory Diseases Admitted to the NICU .................................. 12 1.1.2 Observation of Respiratory and Cardiac Diseases ............................................................................. 12 1.1.3 Treatment and Complications of Neonatal Respiratory and Cardiac Diseases .................................. 13 1.1.4 Tidal Volume and Functional Residual Capacity ................................................................................ 13
1.2 HYPOTHESIS ................................................................................................................................................. 14
II. MATERIALS AND METHODS ..................................................................................... 15 2.1 ELECTRICAL IMPEDANCE TOMOGRAPHY (EIT): ........................................................................................... 15 A HISTORICAL BACKGROUND – FROM 1983 UNTIL TODAY ............................................................................... 15 2.2 ELECTRICAL IMPEDANCE SEGMENTOGRAPHY (EIS): INTRODUCTION OF A NEW METHOD .......................... 17
2.2.1 Which Information Can Be Derived by EIS? ....................................................................................... 17 2.2.2 Indications for the Use of EIS in Newborns and Infants ..................................................................... 18 2.2.3 Further Potential Use of EIS ............................................................................................................... 19
2.3 EIS MEASURING DEVICES ............................................................................................................................ 20 2.3.1 Basic Information ................................................................................................................................ 20 2.3.2 Signal Transmission ............................................................................................................................ 21 2.3.3 Instrumentation Amplifier ................................................................................................................... 23 2.3.4 Constant Current Source ..................................................................................................................... 25 2.3.5 User Software ...................................................................................................................................... 25 2.3.6 “Angelie” – A New Monitoring Tool .................................................................................................. 26 2.3.7 Handling of Medical Devices .............................................................................................................. 28 2.3.8 International Standards ....................................................................................................................... 28 2.3.9 Risk Analysis ....................................................................................................................................... 28
2.4 THE INVESTIGATION PLAN ........................................................................................................................... 29 2.4.1 Study Design ........................................................................................................................................ 29 2.4.2 Patient Selection .................................................................................................................................. 29 2.4.3 Inclusion Criteria and Exclusion Criteria for the Infants in our Study Group .................................... 33 2.4.4 Parental Consent ................................................................................................................................. 34 2.4.5 Positioning of Electrodes .................................................................................................................... 34 2.4.6 Electrode Vest ..................................................................................................................................... 40 2.4.7 “Electrode- Onesie” – A Future Concept? ......................................................................................... 40 2.4.8 Examination Course ............................................................................................................................ 43
2.5 ANALYZING DATA – PROCEDURE INSTRUCTION .......................................................................................... 46 2.5.1 How to Detect Tidal Impedance Changes? ......................................................................................... 46 2.5.2 From Record to Results: Spontaneously Breathing Infants ................................................................. 47 2.5.3 From Record to Results: Infants with Assisted Ventilation ................................................................. 50 2.5.4 Breathing Pattern ................................................................................................................................ 54 2.5.5 Data Export from EIS to MS Excel ...................................................................................................... 57 2.5.6 Filtered Data versus Unfiltered Data .................................................................................................. 62 2.5.7 Self- Adhesive Electrodes .................................................................................................................... 62 2.5.8 Mirrored Impedance Signals ............................................................................................................... 63 2.5.9 Difficulty with Analyzing Data ............................................................................................................ 64
III. RESULTS ......................................................................................................................... 66 3.1 SPONTANEOUSLY BREATHING INFANTS ....................................................................................................... 66
3.1.1 Group I: Infants Weighing 1.5- 2.0kg.................................................................................................. 66 3.1.2 Group II: Infants Weighing 2.0- 2.5kg ................................................................................................ 72 3.1.3 Group III: Infants Weighing more than 3kg ........................................................................................ 77 3.1.4 Relationship between Tidal Volume and Functional Residual Capacity ............................................. 82 3.1.5 Summary of Spontaneously Breathing Infants ..................................................................................... 85
3.2 INFANTS WITH ASSISTED VENTILATION ....................................................................................................... 91 3.2.1 Infants with SIMV ................................................................................................................................ 91 3.2.2 The Infant with CPAP ........................................................................................................................ 109

9
3.2.3 Summary of Infants with Assisted Ventilation ................................................................................... 119 3.2.4 Spontaneously Breathing Infants versus Infants with Assisted Ventilation ....................................... 119 3.2.5 Tidal Impedance and Residual Impedance Before and After Extubation/ Weaning of CPAP ........... 120
3.3 MISCELLANEOUS........................................................................................................................................ 121 3.3.1 Distribution of Tidal Impedance Based on Body Weight .................................................................. 121 3.3.2 Distribution of Residual Impedance Based on Body Weight ............................................................. 122 3.3.3 Effect of Incorrectly Placed Electrodes on the Results ...................................................................... 123 3.3.4 Total Tidal Impedance Based on Body Weight.................................................................................. 126 3.3.5 Total Residual Impedance Based on Body Weight ............................................................................ 127 3.3.6 Residual Impedance in the Lower Left Segment of the Thorax Based on Body Weight .................... 128 3.3.7 Different Breathing Pattern in Infants ............................................................................................... 129 3.3.8 The Impact of Feeding on Tidal Impedance and Residual Impedance .............................................. 137 3.3.10 The Effect of Hiccups on Tidal Impedance and Residual Impedance .............................................. 144
IV. DISCUSSION ................................................................................................................. 145 4.1 ELECTRICAL IMPEDANCE SEGMENTOGRAPHY: A NEW GENERATION IN BEDSIDE LUNG CONTROL OF NEWBORNS? .................................................................................................................................................... 145
4.1.1 Spontaneously Breathing Infants ....................................................................................................... 145 4.1.2 Infants with Assisted Ventilation ....................................................................................................... 156 4.1.3 Tidal Impedance as Surrogate for Tidal Volume? ............................................................................ 163 4.1.4 Residual Impedance as Surrogate for Functional Residual Capacity? ............................................. 164 4.1.5 Practicability of a New Method in Neonatal Intensive Care ............................................................. 167
4.2 THE ROLE OF LUNG ANATOMY AND LUNG PHYSIOLOGY IN EIS MEASUREMENTS .................................... 168 4.2.1 Is EIS a New Method to Study Lung Function? ................................................................................. 168 4.2.2 Control of Lung Physiology of every Infant Admitted to the NICU or Simply Control of Lung Pathophysiology under Mechanical Ventilation? ...................................................................................... 168 4.2.3 What is Homogeneous Ventilation? .................................................................................................. 169
4.3 ADVANTAGES AND LIMITATIONS OF EIS ................................................................................................... 170 4.4 CONCLUSION .............................................................................................................................................. 171
SUMMARY ........................................................................................................................... 172
ZUSAMMENFASSUNG ..................................................................................................... 174
ABBREVIATIONS .............................................................................................................. 176
INDEX OF FIGURES .......................................................................................................... 178
REFERENCES ..................................................................................................................... 182 BOOKS ............................................................................................................................................................. 186 INTERNET ......................................................................................................................................................... 186

10
I. Introduction Electrical Impedance Segmentography (EIS) is a painless, low cost, non invasive and
radiation-free method to continuously record distribution of air and/or fluids in parts of the
human body, thus to monitor tissue composition and its alteration (e.g. within the thorax).
Inhomogeneous distribution of air and ventilation between right and left lung as well as
within each lung remains a major problem in neonatal intensive care. It constitutes a
therapeutic dilemma, since increasing ventilatory support also increases the inhomogeneity
and gas exchange disturbances. Alveolar collapse or overdistension of the lungs is associated
with ventilation/perfusion mismatch. Regional changes of lung ventilation, such as alveolar
collapse and atelectasis, pneumothorax, thoracic effusions, misplacement of tracheal tubes or
surfactant can be diagnosed by x-ray, but cannot be monitored continuously in clinical routine
at bedside in NICUs at present. Therefore methods to monitor regional ventilation of
spontaneously breathing infants and especially of mechanically ventilated infants at bedside
are required.
According to an innovative proposal by G.Simbruner and innovative development of software
by EMS Biomedical Handelsges.mbH, Korneuburg, Austria, this electrical impedance method
is used to detect changes in regional lung volume and regional tidal ventilation in four
segments of the thorax. It has been termed Electrical Impedance Segmentography (abbr. EIS).
In a series of animal experiments 1, 2, 3 conducted in six newborn piglets, EIS was shown to
reliably reflect regional tidal ventilation since the sum of all regional tidal impedance changes
closely correlated with the pneumotachographically measured tidal volume. 3
The clinical use of EIS would allow to detect and monitor pathologies such as 1) unilateral
lung diseases (e.g. pneumothorax, pleural effusions, misplaced tracheal tubes and surfactant;
overdistensions due to congenital or acquired emphysema, others), 2) effect of alveolar
recruitment maneuvers (according to open lung concepts & strategies; Lachmann B)4 as well
as 3) serve as trigger signal of a respirator.
The aim of a monitoring tool - such as EIS - is to observe newborns continuously that require
mechanical ventilation, continuous positive airway pressure (CPAP) or newborns at risk of
developing any kind of respiratory disease.

11
Finally EIS could be used to assess cardiovascular changes (e.g. fall in cardiac output,
increased lung perfusion due to a left-to-right shunting via a patent ductus arteriosus,
hemodynamics of congenital heart diseases, others) represented by electrical impedance
changes within the thorax along the heart axis (predominantly heart, little lung tissue, thus
functional residual capacity (FRC) changes would have a minor effect.)
In this pilot investigation of human newborns we studied 1) the feasibility and practicality of
the method, 2) the impact of body movements, feeding and body position on EIS recordings,
3) the effect of alteration of positive end expiratory pressure (PEEP) on regional FRC and
regional tidal volumes reflected by residual impedance and tidal impedance changes and 4)
whether cardiovascular changes due to “autotransfusion” by elevating both legs to vertical can
be reliably detected by EIS.

12
1.1 Medical Background - Neonatal Respiratory and Cardiac
Diseases
1.1.1 Clinical Features in Infants with Respiratory Diseases Admitted to
the NICU
Electrical impedance segmentography is designed to monitor lungs of premature and mature
sick infants in Neonatal Intensive Care Units. Infants with any kind of lung disease admitted
to the NICU most commonly present with respiratory distress (RDS). Respiratory distress
syndrome is a condition which can be clinically diagnosed by X-ray, treated with surfactant,
continuous positive airway pressure, conventional mandatory ventilation or when needed high
frequency ventilation.55 Indeed a continuous monitoring of regional processes ongoing within
the lungs (i.e overdistension of the lungs, atelectasis, edema, pneumothorax and others) is still
missing until today.
Mostly prematurely born infants present with respiratory distress syndrome after birth (within
up to the first 72 hours after birth) and a reduction in functional residual capacity (FRC) of the
lungs occurs. Transient tachypnea of the newborn may be another cause of FRC reduction in
near-term infants, further a persistent ductus arteriosus, meconium aspiration syndrome, and
pulmonary edema may affect FRC and tidal breathing of the infant.56
Infants clinically present with cyanosis, grunting, tachypnea, intercostal retractions and
sometimes even nasal flaring during their postnatal period.55 Electrical impedance
segmentography should be applied in these infants in a daily routine.
1.1.2 Observation of Respiratory and Cardiac Diseases
Continuous observation of infants with respiratory distress syndrome is not routinely available
until today. X-ray is used for diagnosis of RDS in infants. Knowledge about regional tidal
volume and regional functional residual capacity would help to better and less harmful
ventilate premature infants and disclose the development of pulmonary disease.21

13
1.1.3 Treatment and Complications of Neonatal Respiratory and Cardiac
Diseases
Infants with severe RDS may need mechanical ventilation and therefore endotracheal
intubation has to be performed, which is a procedure with well known complications such as
hypoxia, esophageal perforation, vocal cord injury, subglottic edema, nasal septum damage,
tracheomalacia, tracheostenosis, malposition, dislodge or obstruction of endotracheal tube,
and increased airway resistance. If successful intubation has been performed the infant is put
at risks arising from positive pressure ventilation, which include cardiovascular effects (i.e.
decrease of venous return and cardiac output, “tamponade” of the heart, and interference with
pulmonary blood flow), acute lung injuries (i.e. barotrauma, volutrauma, biotrauma, and
atelectasis), airleaks, uneven ventilations, V/Q mismatch, acid-base imbalance, chronic lung
disease, pulmonary hypertension, cor pulmonary and even intraventricular hemorrhage and
periventricular hemorrhage.56 Mechanical ventilation should be closely monitored to reduce
the risk of developing any disease.
1.1.4 Tidal Volume and Functional Residual Capacity
Tidal volume (VT) is defined as the volume of gas in and out of the lungs during a single
breath. Other lung volumes include functional residual capacity (FRC) and inspiratory
capacity (IC), the latter is determined by tidal volume (VT) and inspiratory reserve volume
(IRV). Functional residual capacity is the volume of gas in the lungs that is in direct
communication with the airways at the end of expiration. It serves as an oxygen storage
compartment in the body as well as a buffer; therefore large changes in alveolar gas tension
are reduced. Observation of newborns’ lungs including tidal volume, functional residual
capacity and respiratory rate are invaluable. Spontaneously breathing infants can only achieve
successful gas exchange within a limited range of respiratory rates. Low rates result in
reduced alveolar minute ventilation and high rates (and likely low tidal volumes) lead to a
larger volume of minute ventilation which is wasted in ventilating dead space.24

14
1.2 Hypothesis
Electrical impedance segmentography is employed to regionally monitor tidal impedance
changes and residual impedance changes of the lungs to gain information about tidal
impedance distribution and residual impedance distribution in spontaneously breathing infants
and in infants with assisted ventilation. Heterogeneity within lung air distribution is known to
occur physiologically in healthy infants determined by several factors such a body position14,
gravity57, ventilation/ perfusion mismatch50, and surfactant production20.
Three hypothesises have been tested in this trial:
1. Regional tidal impedance shows the highest tidal impedance changes within the lower
right segment of the lungs
2. Regional residual impedance shows the highest residual impedance changes within the
upper right segment of the lungs.
3. Total residual impedance shows the highest tidal impedance changes in prone position of
the infant.
15
II. Materials and Methods
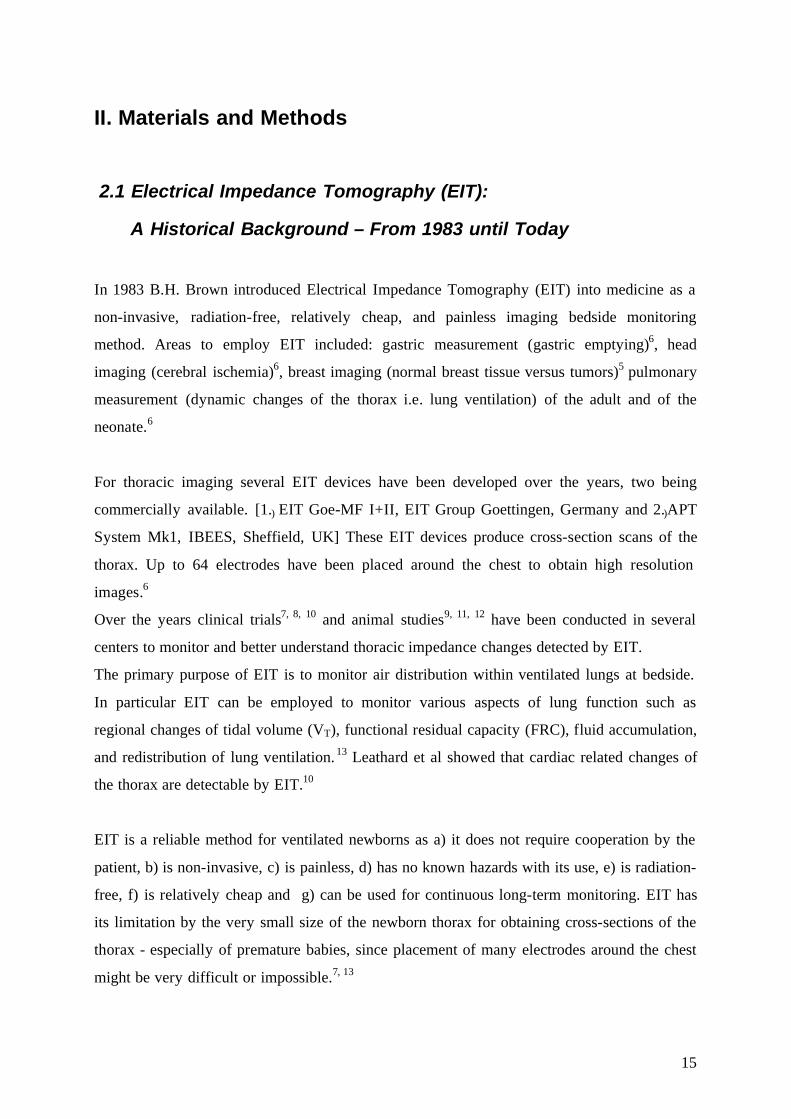
2.1 Electrical Impedance Tomography (EIT):
A Historical Background – From 1983 until Today In 1983 B.H. Brown introduced Electrical Impedance Tomography (EIT) into medicine as a
non-invasive, radiation-free, relatively cheap, and painless imaging bedside monitoring
method. Areas to employ EIT included: gastric measurement (gastric emptying)6, head
imaging (cerebral ischemia)6, breast imaging (normal breast tissue versus tumors)5 pulmonary
measurement (dynamic changes of the thorax i.e. lung ventilation) of the adult and of the
neonate.6
For thoracic imaging several EIT devices have been developed over the years, two being
commercially available. [1.) EIT Goe-MF I+II, EIT Group Goettingen, Germany and 2.)APT
System Mk1, IBEES, Sheffield, UK] These EIT devices produce cross-section scans of the
thorax. Up to 64 electrodes have been placed around the chest to obtain high resolution
images.6
Over the years clinical trials7, 8, 10 and animal studies9, 11, 12 have been conducted in several
centers to monitor and better understand thoracic impedance changes detected by EIT.
The primary purpose of EIT is to monitor air distribution within ventilated lungs at bedside.
In particular EIT can be employed to monitor various aspects of lung function such as
regional changes of tidal volume (VT), functional residual capacity (FRC), fluid accumulation,
and redistribution of lung ventilation. 13 Leathard et al showed that cardiac related changes of
the thorax are detectable by EIT.10
EIT is a reliable method for ventilated newborns as a) it does not require cooperation by the
patient, b) is non-invasive, c) is painless, d) has no known hazards with its use, e) is radiation-
free, f) is relatively cheap and g) can be used for continuous long-term monitoring. EIT has
its limitation by the very small size of the newborn thorax for obtaining cross-sections of the
thorax - especially of premature babies, since placement of many electrodes around the chest
might be very difficult or impossible.7, 13

16
Dunlop et al7 conducted a clinical trial applying EIT in prematurely born infants (mean
weight 1126gm, mean 29 weeks of postconceptional age) to monitor the lungs of
mechanically ventilated infants. According to difficulties of placing neighboring electrodes
and unacceptable signal-to-noise ratio unfiltered EIT images recorded were very noisy.7
Indeed prematurely born infants (<2kg) are in dire need of a bedside monitoring method of
their lungs which does not exist until today. Chest x-ray (as well as CT) allows obtaining
instantaneous imaging of lungs, but is limited due to radiation exposure. MRI without
radiation hazard of newborn infants is possible, but not always available and expensive. MRI
requires cooperation by the patient thus most infants have to be sedated by narcotic drugs
which are a hazard to the developing central nervous system of the newborn.58
Clinical trials performed in mature infants clearly show that EIT is a feasible method to
monitor ventilated neonates. Heinrich et al 8 published a clinical trial on EIT use in mature
infants [current weight (±SD) 3478g (± 782), postnatal age 58 (±36) days]. The influence of
head and body position on the distribution of ventilation in mechanically ventilated infants
has been studied by chest cross-section scans obtained by EIT. Tidal volumes in the right and
left lung regions were significantly higher during mechanical ventilation than during
spontaneous breathing but were not affected by body or head position. Tidal volumes during
spontaneous breathing were not affected by body or head position, whilst during mechanical
ventilation; their magnitude was influenced by head or body position. Dunlop et al observed a
shift of ventilation from right-to-left during controlled mechanical ventilation. (In detail: a
reduced tidal volume in the left lung by rotation of the head to the left side and an increased
ventilation of the right lung, a shift which was more pronounced in prone position than in
supine position). According to these findings of ventilation dependent on body and head
position and the occurrence of pathologies described above, a reliable and meaningful
monitoring of newborn infants on mechanical ventilation is warranted in infants particularly
in those receiving long-term mechanical ventilation.

17
2.2 Electrical Impedance Segmentography (EIS): Introduction of a New Method Electrical Impedance Segmentography (EIS) is developed and provided by EMS Biomedical,
EMS Handelsges.mbH, Korneuburg, Austria. EIS is composed of a computer unit, an
amplifier, and a constant current source. The current software “EIS Version 2.8” is developed,
programmed, supervised and evaluated by EMS Biomedical, EMS Handelges.m.b.H. Sensing
electrodes (Blue Sensor, BRS-50-k) are produced by Ambu®, Denmark, distributed by
Chemomedica Vertriebsgesellschaft.m.b.H, Vienna, Austria. The primary purpose of EIS is to
detect regional impedance changes simultaneously in upper and lower parts, right and left side
of the thorax. The thorax thus is virtually divided into four regions of interest and impedance
signals are recorded in all four regions of interest (upper left, upper right, lower left, lower
right thorax) continuously over time. EIS is an electrical impedance measurement to assess
impedance changes in four segments of the lungs.
2.2.1 Which Information Can Be Derived by EIS?
A) Regional lung function in terms of regional tidal volume (VT) which is reflected by total
tidal impedance changes (abbreviated: tidal impedance tidI).3
B) Functional residual capacity (FRC) of the four thoracic segments is reflected by the total
residual impedance (abbreviated: residual impedance resI) which depends on the composition
of air and fluid of the lung tissue of the segment under consideration as well as intrathoracic
changes. (See “4.1.4 Residual Impedance as Surrogate for Functional Residual Capacity?”)
In contrast to previous attempts to use EIT for imaging and detection of lung
inhomogeneties12 we abandoned the goal of producing electrical impedance images of cross-
sections of the chest. To produce cross-section scans and to gain high resolution images of the
human thorax a high number of electrodes, up to 16 electrodes, would be necessary. The EIS
method proposed by G. Simbruner focuses on detecting and monitoring the clinical treatable
inhomogeneities as they occur in the upper and lower, left and right segments of the chest.
(See"2.2.2 Indications for using EIS in Newborns and Infants")

18
EIS was initially based on using only eight detecting electrodes and two injecting electrodes
in the mode of bipolar recording. The number of electrodes was further reduced to five
detecting and two injecting electrodes for the unipolar recording. The aim of our study is to
investigate whether tidal volume changes and FRC changes during various settings of MAP
(as PEEP) and tidal volume are detected with sufficient accuracy to be of clinical use, the
influence of body and head position, and to test the practicability and feasibility of this
innovative method before EIS is introduced for monitoring and diagnostic procedures in
neonatal intensive care.
2.2.2 Indications for the Use of EIS in Newborns and Infants
Indications to monitor the lungs of premature and mature infants include:
1) To closely study lung physiology of infants and herewith achieve less harmful ventilation:
To monitor patterns, amount and distribution of ventilation in spontaneously breathing
neonates as reported by Frerichs et al.14 Neonatal spontaneously breathing was shown to
consist of episodes of fast, slow, small, and big breaths and to vary in newborns when lying
in three different postures.14 (prone position, right lateral position, and supine position)
2) To monitor periods of apnea, a very common respiratory disorder in premature infants -
notably Apnea of Prematurity - requires therapy and is associated with risk of abnormal
neurological outcome. 15
3) To detect abnormal positioning and dislocation of the endotracheal tube. The correct
positioning and monitoring is the maintenance of or dislocation from this position.
4) To detect abnormal placement of administered surfactant often resulting in inhomogeneous
air distribution and ensuing pneumothoraces .
INSURE (Intubation – Surfactant – Extubation) provides surfactant application followed by a
short period of ventilation and reduces extubation time. Drugs to provide good analgesia
during INSURE but early extubation have been recently studied.59 Monitoring of this process
would be a great benefit for this procedure.

19
5) Instantaneous detection and localization of a pneumothorax which is associated with an
increased risk of cerebral injury. 16
6) To avoid damage of the lung tissue due to overdistension of the lungs by inadequate PEEP
levels and ensuing pneumothorax, or due to atelectasis by continuous assessing trends of
distribution of ventilation in the four segments of the thorax, and employing high frequency
oscillatory ventilation (HFOV) which was shown to result in a more homogenous
ventilation.17
2.2.3 Further Potential Use of EIS 7) EIS may be employed as a monitoring tool to monitor lung recruitment when employing
PEEP and setting it to various levels in mechanically ventilated infants since avoiding
atelectasis and achieving full, homogeneous lung recruitment is known as protective
ventilation. 12
8) EIS may provide an appropriate signal for triggering inspiration and terminating expiration
of mechanical breath provided by a respirator.
9) EIS may indicate abnormal haemodynamics.
20
2.3 EIS Measuring Devices
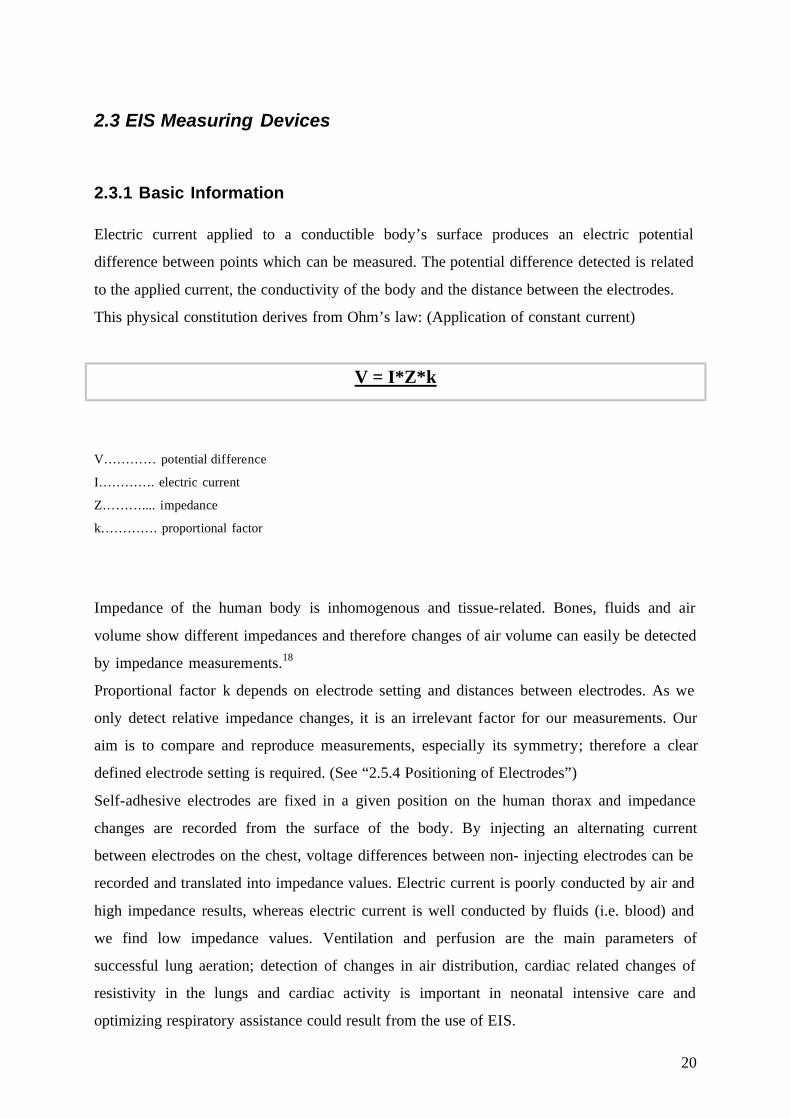
2.3.1 Basic Information Electric current applied to a conductible body’s surface produces an electric potential
difference between points which can be measured. The potential difference detected is related
to the applied current, the conductivity of the body and the distance between the electrodes.
This physical constitution derives from Ohm’s law: (Application of constant current)
V = I*Z*k
V………… potential difference
I…………. electric current
Z……….... impedance
k…………. proportional factor
Impedance of the human body is inhomogenous and tissue-related. Bones, fluids and air
volume show different impedances and therefore changes of air volume can easily be detected
by impedance measurements.18
Proportional factor k depends on electrode setting and distances between electrodes. As we
only detect relative impedance changes, it is an irrelevant factor for our measurements. Our
aim is to compare and reproduce measurements, especially its symmetry; therefore a clear
defined electrode setting is required. (See “2.5.4 Positioning of Electrodes”)
Self-adhesive electrodes are fixed in a given position on the human thorax and impedance
changes are recorded from the surface of the body. By injecting an alternating current
between electrodes on the chest, voltage differences between non- injecting electrodes can be
recorded and translated into impedance values. Electric current is poorly conducted by air and
high impedance results, whereas electric current is well conducted by fluids (i.e. blood) and
we find low impedance values. Ventilation and perfusion are the main parameters of
successful lung aeration; detection of changes in air distribution, cardiac related changes of
resistivity in the lungs and cardiac activity is important in neonatal intensive care and
optimizing respiratory assistance could result from the use of EIS.
21
Figure 1 Scheme of electrical impedance segmentography [Bauer H, 2005]
.
2.3.2 Signal Transmission Impedance changes recorded by EIS are relative impedance changes (rel. ∆ |Z|) measured
over time. Signals and impedance changes described in each chapter of this work are always
rel ∆ |Z|.
Electrical impedance segmentography requires 2 injection electrodes and 8 measuring
electrodes in the bipolar mode, 2 injection electrodes and 5 measuring electrodes in the
unipolar mode. (See “2.4.5 Positioning of Electrodes”)
In this study all infants have been examined by applying electrodes in the bipolar mode onto
the infants’ thoraces. A constant sinus wave alternating current is running in between the two
injection electrodes. Based on Ohm’s Law (V= Z*I)a the electric current remains unchanged
during measurements independently from the height of the impedance signal. As a
consequence potential difference is changing. Alternating current is injected into the thorax by
the frontal or dorsal injection electrode in turns, alternating 5000 times per second. (5kHz) a V= Z*I, V= potential difference, Z= impedance, and I= electric current
22
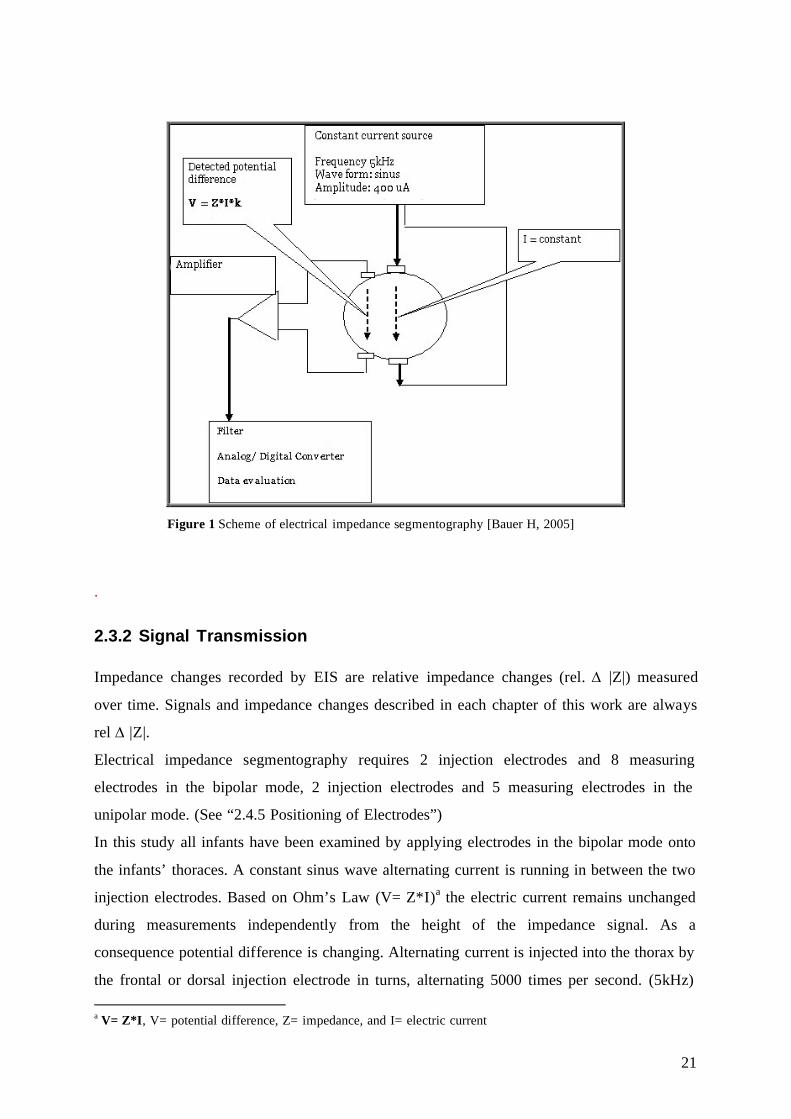
The alternating current generates an electrical field showing field lines and potential lines.
Potential lines end at the body’s surface, therefore potential differences within two measuring
points can be detected. The instrumentation amplifier is able to measure the differences in
potentials. Inhomogenities, i.e. changes in air distribution, fluids within the thorax change the
signal of the potential lines and electrodes are able to detect these potential alternations which
are measured by the instrumentation amplifier. The signals measured are potential differences.
Fig 2 illustrates the characteristics of potential lines and field lines within the thorax.
Figure 2 Cross-section of the thorax Illustration of field lines and potential lines within an object. [Bauer H, 2009]
Fig 3 demonstrates the characteristics of potential lines and field lines within the thorax by
showing an example organ and the deviation of their characteristics which can be measured
by EIS.

23
Figure 3 Cross-section of the thorax displaying one organ to illustrate potential lines and field lines within the thorax.[Bauer H, 2009]
2.3.3 Instrumentation Amplifier
EMS has recently developed a new CE approved amplifier SURPASS EMG/EP/NSC. This
amplifier is compatible for electrical impedance segmentography measuring devices.
Figure 4 Surpass system [Bauer H, 2005]
24
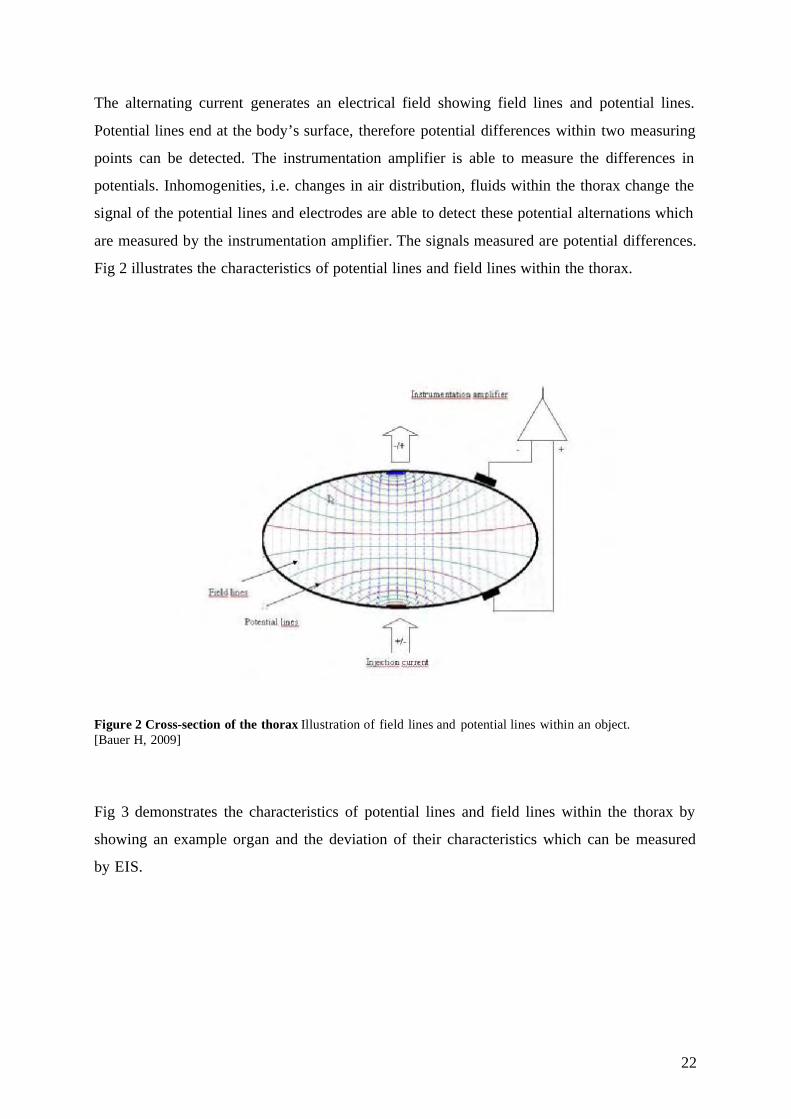
Electrode signals arrive through an analogue cross switch to the instrumentation amplifier,
which is characterized by a high input resistance and a common mode rejection voltage of at
least 110dB.
Accordingly the signals are processed by a switchable second order high pass filter and by a
switchable amplifier level. A fixed frequency second order low pass filter serves as anti-
aliasing filter for a 200K sample 4 fold ADC with a 16bit resolution.
The low pass filter cannot be switched directly, but only through the analysing software.
The consecutive logic processes information from up to 24 channels. Patient safety is of high
priority. Therefore the digital signals are disconnected by a 5kV isolation barrier and buffered
by a FIFO. The FIFO is connected to the PC via a USB 2.0 interface; information is
transferred and evaluated by the software. Additionally the stimulation unit HELIOS is
connected to the PC.
The sampling rate of the amplifier is regulated by the number of active channels. During our
measurements we apply 4 channels. Therefore the sampling rate achieves a maximum of 50K
samples per second.
Instrumentation Amplifier
For technical data of the instrumentation amplifier, see Tab 1.
Amplifier 800 fold
Second order high pass filter 1Hz
ADC sampling frequency 40kHz/per channel, 16bit resolution
Measuring frequency 5kHz sinus-signal
Measurement current 400 µA
Sampling rate 2ms/ 4 channels
Tab 1. Instrumentation amplifier information [Bauer H, 2009]

25
2.3.4 Constant Current Source A constant current source is required to produce a measurement current. A digital frequency
generator triggers a sinus wave output voltage. Frequency is adjusted to 5 kHz. Measurement
current achieves 400 µΑ.
2.3.5 User Software
Controlling software is derived from SURPASS EMG/EP/NSC. PC software is newly
developed by EMS Biomedical, Biomedical Handelsges.mbH, Korneuburg, Austria. PC
software “EIS 2.8” shows two main functions:
• Record/ Review data
• Data evaluation
SURPASS Amplifier – connected to an USB Interface – is transmitting raw data to the PC for
subsequent processing. According to advanced technology impedance is recorded
independently from signal-noises. Raw data is collected for evaluation purposes. To easily
review the collected data in time, a related text marker can be used during the recording
process.
We use a maximum of 8 measuring (non- injection) and 2 current (injection) electrodes to
assess changes of regional tidal volume (VT), changes of fractional residual capacity (FRC)
and cardiovascular changes. The human thorax is divided into 4 segments; each segment is
represented by 2 measuring electrodes, one placed in front of the body and one on the
backside. (See “2.5.4 Positioning of the Electrodes”)
Fig. 5 displays the front mask of the EIS software “Angelie”. EIS is able to monitor tidal
volumes (tidal impedance) changes, dynamic changes of the thorax (mostly affected by
increase/ decrease of FRC), EKG, and SaO2. Connected to a ventilator EIS is able to gain
flow and pressure data from the ventilator through a connection wire, compliance may be
observed by EIS in infants.

26
Figure 5 EIS software - front mask
Data Evaluation
For further information see “2.5 Analyzing Data”
2.3.6 “Angelie” – A New Monitoring Tool
The first newborn - at a body weight of nearly 2kg - has been examined in December 2006 to
introduce EIS into neonatal care. Fig 6 illustrates impedance signals of the first EIS
measurements in neonates ever. According to this promising examination EIS showed to be a
reliable tool to detect impedance changes in newborns after a series of successful studies in
newborn piglets.1,2, 3 Ever since written consent from the local Ethics Committee of the
Medical University of Innsbruck, Austria (written consent: February 5, 2008) and the
Austrian Agency for Health and Food Safety (written consent: AGES, May 20, 2008) have
been achieved to conduct our trial in newborn babies and to employ EIS for further
monitoring of newborns’ lungs in Austria.
After a time consuming approval to get EIS approved by the responsible authorities, primarily
by the local Ethics Committee and secondly by the Agency for Health and Food Safety EIS
could be employed for its first clinical trial in neonatology. During that time EIS software
underwent plenty of updates to end up with the – until today – best possible recording and
analyzing software so far.

27
Back in 2005 EIS has been invented by G. Simbruner to primarily monitor the lungs of
ventilated neonates. Based on that idea EIS had been modified several times:
First parameters of interest included tidal volume and functional residual capacity in 4
segments of the lungs. Electrode setting has not been changed but has been extended (unipolar
mode or bipolar mode, See “2.5.4 Positioning of Electrodes”) during that time. SaO 2
monitoring and ECG function have been added to the software features. Furthermore the idea
to connect EIS devices with the ventilator of the observed infant to assess pressure and flow
curves has been suggested by M. Rüdiger and is now included in the EIS software. EIS
recorded data can now be seen in the review mode as an “overview” data or in the data panel
as “real time” data, to easily detect tidal impedance and exclude artifacts which may have
irritated our measurement signal. EIS data can be transferred to MS Excel 2003 and following
MS Excel versions for analyzing purposes, either each recorded data point is transferred, an
average of each 50th recorded data point or – according to newly development by H. Bauer –
only tidal impedance changes, such as the highest tidal amplitude are detected by EIS Version
2.8 and directly transferred to MS Excel 2003. Furthermore EIS 2.8 is able to record
impedance changes of both ventilated infants and spontaneously breathing infants.
Figure 6 First EIS measurements in a 2kg infant in 4 Figure 7 First EIS measurements segments of the lungs
28
2.3.7 Handling of Medical Devices To correctly set up the medical devices of EIS follow the instructions:
1) Connect EIS to the USB 2.0 port of the PC on which the EIS software is installed.
2) Power up the PC – no extra power supply for the amplifier is required; the amplifier is
energized via the USB 2.0 interface.
3) Start “EIS” program on the PC.
4) If disconnected, connect the electrode box with the amplifier.
5) Turn current potentiometer to zero.
6) Attach the electrodes carefully to the patient’s thorax.
7) Start “check amplifier” function of the program to test the connection with the electrodes.
8) Start “Record” mode to observe electrical impedance signals and record data.
2.3.8 International Standards
Surpass EMG/EP/NSC meets the essential requirements of the medical device directive
93/42/EWG, class IIa, directive 10 and is manufactured to the following standards:
• EG-Richtlinie: 93/42/ EWG
• IEC 60601-1:1996; IEC 60601-1-2: 2001; IEC 60601-2-26:2002
2.3.9 Risk Analysis Electrical Impedance Segmentography has been tested by the Austrian Technical Inspection
Authority (TÜV), positive written confirmation was provided by the Austrian Technical
Inspection Authority (TÜV) on March 13, 2008.

29
2.4 The Investigation Plan
Written consent from the local Ethics Committee of the Medical University of Innsbruck,
Austria to conduct this trial at our local Neonatal Intensive Care Unit has been successfully
achieved on February 5, 2008 and positive written consent from the Austrian Agency of
Health and Food Safety to employ our electrical impedance device developed by EMS
Biomedical Handels.ges.mbH was received on May 20, 2008.
2.4.1 Study Design
The aim of our study was to detect changes in VT and FRC in neonates by EIS. The infants
have been organized in two groups: 1) Spontaneously breathing infants and 2) infants
requiring assisted ventilation. In the spontaneously breathing infants group examination of the
body position (supine position, left lateral position, and prone position) and its effect on V T
(reflected by tidal impedance tidI) and FRC (reflected by residual impedance resI) has been
investigated.
In the assisted ventilation infants group a total alternation of PEEP of 2 cm H2O has been
performed and its effects on tidI and resI have been observed.
2.4.2 Patient Selection
We performed a controlled trial of 15 newborn infants admitted to either the NICU or the
Intermediate Care Unit. Infants must have met the inclusion criteria and have no exclusion
criteria. (See “2.4.3 Inclusion Criteria and Exclusion Criteria of the Infants”) First the 15
neonates were divided into two groups: Spontaneously breathing infants (11) and
mechanically ventilated infants (4). Further on the spontaneously breathing infants were
subdivided into 3 groups according to the infants’ current weight at the day of examination.
One newborn was eliminated from the spontaneously breathing infants group due to an
alteration of electrode positions. (See “3.3.3 Effect of Incorrectly Placed Electrodes on the
Results”)
Fig. 8 gives an overview of the patient groups and fig.9 and 10 describe the patient groups in
detail:

30
Figure 8 Main patient groups
15
Infants
4
Infants with Assisted
Ventilation
11
Spontaneously Breathing
Infants

31
Spontaneously Breathing Infants The patient group of the spontaneously breathing infants was divided into 3 subgroups which
were defined by the patients’ current body weight. The first group GI included 3 newborns
with a body weight between 1500g and 2000g. The second group GII is composed of 3 infants
with a body weight of 2000g to 2500g. The third group GIII consists of bigger infants whose
bodies weigh more than 3000g and this group includes 4 infants. One additional infant with a
body weight over 3000g has been excluded from the study as the electrode position on the
thorax of that baby was altered. Figure 9 describes the patients groups GI, GII, and GIII in
detail:
Figure 9 Details of spontaneously breathing infants
11
Spontaneously Breathing
Infants
3 Infants
1.5-2.0kg
3 Infants
2.0-2.5kg
4 Infants > 3kg
1 Drop Out

32
Infants with Assisted Ventilation The group IV of the mechanically ventilated infants included 3 neonates receiving SIMV and
a PEEP level of 4.5cm H2O and one newborn receiving CPAP therapy. The infants’ weight
ranged from 1500g to 3210g. Fig10 shows the group of the mechanically ventilated infants in
detail:
Figure 10 Infants with assisted ventilation
4 Infants with
Assisted Ventilation
3 Infants SIMV+ PEEP
1 Infant CPAP

33
2.4.3 Inclusion Criteria and Exclusion Criteria for the Infants in our Study Group
Inclusion Criteria Spontaneously Breathing Newborns
Eligible patients must have met all of the following inclusion criteria:
• Current weight: >1500g
• Postconceptional age: >30 weeks, < 42 weeks
• Signed informed parental consent
Newborns Requiring Respiratory Assistance
Eligible patients must have met all of the following inclusion criteria:
• Current weight: >1500g
• Postconceptional age: >30 weeks, < 42 weeks
• Signed informed parental consent
PLUS
• Continued need for respiratory assistance (CPAP or ventilation of one of the
following):
1.) Continuous positive airway pressure (CPAP)
2.) Controlled or intermitted mandatory ventilation (CMV/ IMV) with positive end-
expiratory pressure (PEEP)
3.) High frequency oscillatory ventilation (HFOV)
• Admitted to the neonatal intensive care unit (NICU)
Exclusion Criteria Spontaneously Breathing Newborns
Eligible patients must have met none of the following exclusion criteria:
• Any lung disease or critical illness
• Any skin disease
• Any acute resuscitation or unstable condition
• Patients participating in any other trial of the respiratory tract

34
Newborns Requiring Respiratory Assistance
Eligible patients must have met none of the following exclusion criteria:
• Any skin disease
• Any acute resuscitation or unstable condition
• Patients participating in any other trial of the respiratory tract
2.4.4 Parental Consent Parental consent was given at least from one of the parents before the onset of the
examination of their child(ren). Consent was obtained in a written form, signed by the
newborn’s parents and verified and signed by the responsible investigator of this study.
2.4.5 Positioning of Electrodes There are two optional modes to measure the electrical impedance changes and therefore there
a two different settings:
Positioning of Electrodes – Bipolar Mode
We define the positions of 2 current electrodes and the positions of 8 measuring electrodes for
15 infants in our study. 5 electrodes (1 current electrode and 4 measuring electrodes) will be
placed on the anterior thorax and 5 electrodes (1 current electrode and 4 measuring
electrodes) will be fixed on the posterior thorax. On each side of the thorax 4 measuring
electrodes represent one segment of the lungs to detect regional changes of lung air volume.
In the anterior of the thorax 2 measuring electrodes will be placed in an upper plain at the 2 nd
intercostal space, one on the left side (UL = upper left electrode) of the thorax and one on the
right side (UR = upper right electrode) at the point that crosses with the medioclavicular line
of each side. Two measuring electrodes will be put on the anterior thorax in a lower plain at
the 5th intercostal space, one on the left side (LL = lower left electrode) of the thorax and one
on the right (LR = lower right electrode) at the point that crosses with the anterior axillary line
of each side.

35
In the upper plain electrodes are fixated in the medioclavicular line, while the lower
electrodes are placed in the axillary line. In the plain of the 5th intercostal space at the point
that crosses the medioclavicular line heart beat may interact with our electrical impedance
measurements. Therefore lower electrodes in the plain of the 5 th intercostal space are placed
in the axillary line. Electrodes have to be arranged symmetrically; therefore the lower left and
right electrodes are placed in the axillary line.
The current electrode of the anterior thorax is placed at the sternum in the plain of the 4 th
intercostal space.
In the posterior of the thorax 2 measuring electrodes are defined in the upper plain of the 3 rd
intercostal space and fixed on the thorax on the left side (UL = upper left electrode) of the
thorax and on the right side (UR = upper right electrode) at the point that the plain crosses
with the scapular line of each side. Two measuring electrodes will be placed in the lower plain
at the 7th intercostal space at the point that crosses with the scapular line one the left side
(LL = lower left electrode) of the thorax and on the right side (LR = lower right electrode).
The current electrode of the posterior thorax is placed at the spine in the plain of the 6 th
thoracic vertebra.
Two electrodes - one from the anterior of the thorax and one from the posterior - represent
one segment, displayed as a variable “channel (ch)” on the screen of the program used, “EIS
2.8”.
Measuring channels:
1.) Anterior UL + posterior UL = representing EI (Electrical Impedance) of upper left
segment by pair of electrodes, ch1+ (ant)b, ch1- (post)c
2.) Anterior UR + posterior UR = representing EI of upper right segment by pair of
electrodes, ch2+ (ant), ch2- (post)
3.) Anterior LL + posterior LL = representing EI of lower left segment by pair of
electrodes, ch3+ (ant), ch3- (post)
4.) Anterior LR + posterior LR = representing EI of lower right segment by pair of
electrodes, ch4+ (ant), ch4- (post)
b (ant) = anterior side of the thorax c (post) = posterior side of the thorax

36
Fig 11 and Fig 12 illustrate the cross section of the thorax, Fig 11 shows the cross section at
the 2nd intercostal space and the electrode positions in this plain. Fig 12 demonstrates the
cross section at the 5th intercostal space and the electrode setting in this plain.
Electrode Setting:
Cross Section at the 2nd Intercostal space Cross Section at the 5th Intercostal Space Fig 11 Fig 12
Figure 11 Cross section of the thorax at the 2nd intercostal space and Figure 12 Cross section of the thorax at the 5th intercostal space. [UR= upper right electrodes, UL= upper left electrodes, LL= lower left electrodes, and LR= lower right electrodes]
Fig 13 shows a newborn and the electrode positions on this infant’s thorax. Upper right
electrodes (anterior and posterior electrodes presenting one channel) are red, the yellow color
has been chosen for the upper left electrodes. The lower left electrodes are illustrated in green
and blue is the color of choice for the lower right electrodes.
Lungs Aorta
Lungs Heart
Thorax Thorax
Left Side Left Side
UR
LR
LL UL
Trachea

37
Figure 13 Electrode setting in a newborn
Picture 14 shows the electrode setting in the anterior view. The 6 th additional, differently
looking electrode was an EKG measuring electrode of the newborn and does not belong to our
electrode setting.
Figure 14 Electrode setting in a newborn anterior view
Front Side of Thorax = Anterior Electrodes … Upper right electrode … Upper left electrode … Lower right electrode … Lower left electrode Back Side of Thorax = Posterior Electrodes … Upper right electrode … Upper left electrode … Lower right electrode … Lower left electrode Injection Electrodes: … one in front of the throax … one at the back of the thorax

38
Fig 15& 16 illustrate the electrode position in the anterior view and in the posterior view.
Figure 15 Scheme of electrode setting in a newborn – Figure 16 Scheme of electrode anterior view setting in a newborn posterior view
Positioning of Electrodes – Unipolar Mode The unipolar mode differs from the bipolar mode in the posterior electrodes´ position. The
anterior positions do not differ from the bipolar mode. In the unipolar mode we define a
posterior common reference, presented only by two posterior electrodes positioned in the
plains of the 5th and 7th thoracic vertebrae. (Fig 17 & Fig18)
The definition of the 4 measuring channels is the following:
1.) Anterior LL + common reference = representing EI of lower left segment by pair of
electrodes, ch3+(ant), common reference
2.) Anterior LR + common reference = representing EI of lower right segment by pair of
electrodes, ch4+(ant), common reference
3.) Anterior UL + common reference = representing EI of upper left segment by pair of
electrodes, ch1+(ant), common reference
4.) Anterior UR + common reference = representing EI of upper right segment by pair of
electrodes , ch2+(ant), common reference

39
Cross Section at the 5th Intercostal Space
Figure 17 Unipolar mode – posterior view Figure 18 Cross section of the thorax at the 5th intercostal space The advantage of the unipolar mode would be the limited number of seven electrodes in total.
In this study we placed the electrodes in the bipolar mode only; therefore further
investigations to test the practicability of the unipolar mode have to be carried out in the
future.
Lungs Heart
ThoraxFront Side
Left Side
Lower Left and Lower Right Electrodes
Common Reference
40
2.4.6 Electrode Vest
As suggested by Dott. Ing. E. Avitabile from Bioingegneria e Elettronica Medica, Napoli,
Italy in a meeting on June 4, 2009 the development of an electrode vest may improve the
electrode setting on the thorax. We still have the problem that self-adhesive electrodes’
impedance signals aren’t as optimal as impedance signals of gold disc electrodes when it
comes to signal transmission. Furthermore self- adhesive electrodes (Ambu® Denmark, Blue
Sensor, BRS-50-k) which have been used in this study, are not produced for long-term
monitoring, but this would be an important purpose of the EIS.
This electrode vest in different sizes (according to the average circumference of the thorax)
could be easily applied around the thorax, made of cotton, and it would increase both
practicability of electrode setting and electrical impedance signal. After disinfection according
to medical standards, this vest could be re-used in infants.
2.4.7 “Electrode- Onesie” – A Future Concept?
In this study all infants’ electrodes have been applied to the infants’ thoraces as described
above. (See “2.4.5 Positioning of Electrodes”)
Electrode placing remains time consuming and requires concentration to properly adjust the
electrodes. Admissions to Neonatal Intensive Care Units are mostly emergencies and time is
limited. Therefore a concept has to be developed to apply electrodes quickly but properly and
to exclude as many sources of error as possible. As described above an electrode vest could
simplify the process of electrode positioning. Herewith the idea of the electrode vest is
specified and the development of an electrodes-included onesie is suggested. Other than the
electrode vest an electrode onesie could be applied closely to the infant’s thorax which is a
dire need as optimal electrode contact with the infant’s skin is required for good impedance
signals. The idea is the development of an electrode onesie made of a combination of cotton
(95%) and spandex (5%), the spandex content gives the fabric elasticity and keeps the shape
of the garment. Cotton/spandex garments move with the body for comfort and stretch, which
would make this fabric ideal for our electrode-onesie. (See “Fig 19 Electrode- Onesie”)
This onesie would be made of three parts (upper, middle and lower part) to provide optimal
signal detection and comfort clothing for the infant.

41
The upper part contains the five frontal and the five backside electrodes and is made of two
layers, each made of 95% cotton and 5% spandex. Every electrode in its unique position has
been assigned a special colour to correctly insert the electrodes in their plugs of the EIS
device.
The middle part is made of two layers, each made of 95% cotton and 5% spandex, in between
which an elastic tape is running. The purpose of this elastic tape is to provide the optimal
shape of the upper part even during manipulation of the infant, i.e. nursing of the infant,
changing diapers.
The lower part consists of cotton (100%) and simply covers the infant’s diapers.
Figure 19 “Electrode- Onesie”: The concept
Upper part: Includes the five frontal side electrodes [upper left, upper right, lower left, lower right and the frontal injection electrode] This part is made of two layers, each made of a fabric consisting of 95% cotton and 5% spandex covering the infant’s chest.
Middle part: Made of two layers, each consisting of 95% cotton and 5% spandex, in between those two layers is an elastic tape, which is never in direct contact with the skin.
Lower part: Simply made of 100% cotton and covers the diaper of the infant.
Color-coded electrode leads with a cotton closure.

42
The two layer-concept of the fabric would contain the electrodes in the upper part of the
onesie. (See “Fig 21 Electrodes within the fabric”)
Figure 20 Syringe with a stump needle Figure 21 Electrodes within the fabric To produce optimal impedance signals with gold disc electrodes, a gel for signal transmission
has to be applied by a syringe with a stump needle into the cylinder of the electrode which has
a hole for exactly that purpose.
Little slots within the fabric of the onesie could be made on the sides of the onesie to lead
drains and other wires of monitoring devices to the outside of the onesie.
Fabric of the onesie
Cylinder of Gold disc electrode
Electrode Lead

43
2.4.8 Examination Course Two courses of examination have been performed during our investigation depending on the
group (spontaneously breathing infants versus infants requiring assisted ventilation) the
examined infant has been assigned to:
Spontaneously Breathing Infants
Before the examination was conducted in this group, signed informed parental consent was
given for all infants. At the beginning electrodes have been carefully placed on the infants’
thoraces to continuously monitor impedance changes of the thorax over a total of 50 to 60
minutes.
The aim of this investigation was to observe the influence of body position on tidI and resI.
FRC has not been investigated in healthy premature and mature infants so far. To develop a
new beside monitoring tool and to gain FRC values of healthy newborns and to use those as
reference data, we investigated lung (patho)physiology of newborns not requiring any kind of
assisted ventilation or CPAP, therefore we observed the lungs of spontaneously breathing
infants. There is a dire need to combine the FRC measurements with the mechanical
respiratory support21, to define the “least” harmful degree of lung recruitment during CPAP
and mechanical ventilation. In this pilot investigation we studied the lungs of 11
spontaneously breathing infants to determine their intra- and intersubject variability.
We started our examination in supine position of the infant and recorded impedance changes
for the next 15 minutes. Further on we lifted the newborn’s legs to the vertical to detect
impedance changes due to cardiovascular changes for a 5 minutes period. After a control
period of another 5 minutes we turned the infant to its left lateral side and recorded
impedances changes for another 15 minutes in this position. Our last procedure was to collect
data of the effect of prone position on tidI and resI, therefore we placed the infant in prone
position for another 15 minutes..
As most of the newborns assigned to the spontaneously breathing infants group have been
admitted to the Intermediate Care Unit, only EKG and/or SaO2 has been observed routinely in
these babies and recorded by the investigator for analyzing purposes.

44
Figure 22 Examination course in spontaneously breathing infants, *CP= control period
Supine Position
15’
Auto- trans-fusion
5’
*CP
5’
Left Lateral Side
15’
Prone Position
15’
45
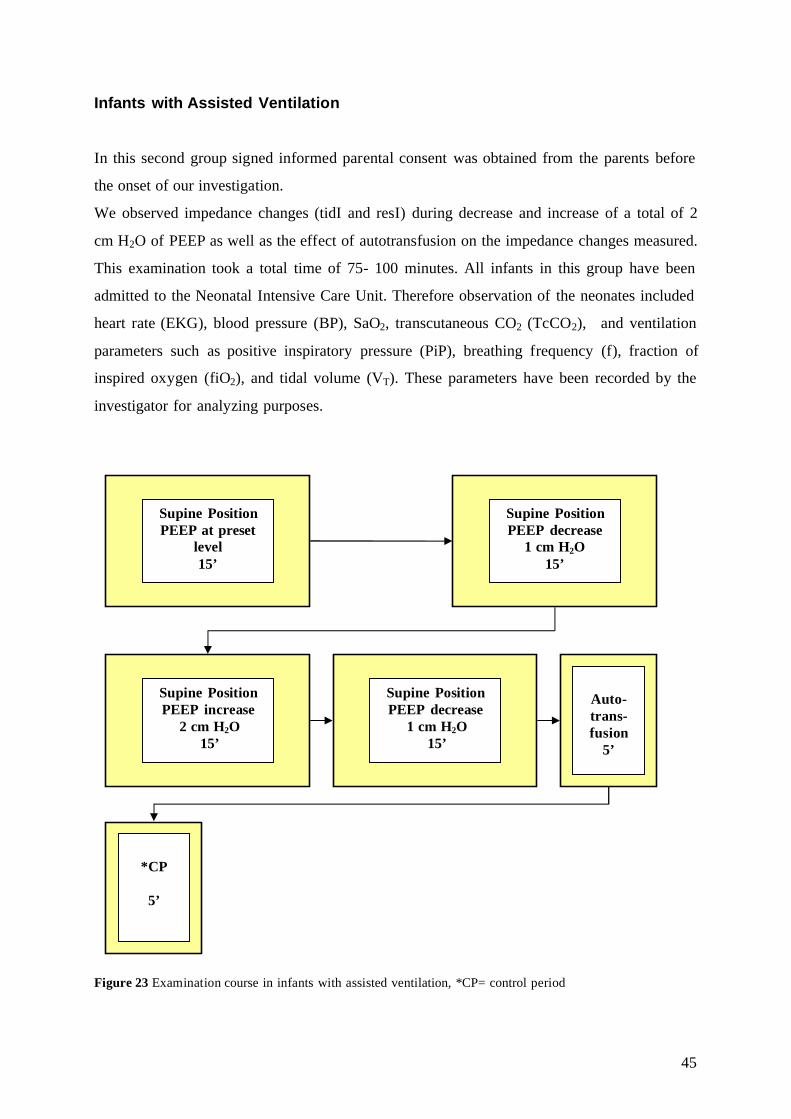
Infants with Assisted Ventilation
In this second group signed informed parental consent was obtained from the parents before
the onset of our investigation.
We observed impedance changes (tidI and resI) during decrease and increase of a total of 2
cm H2O of PEEP as well as the effect of autotransfusion on the impedance changes measured.
This examination took a total time of 75- 100 minutes. All infants in this group have been
admitted to the Neonatal Intensive Care Unit. Therefore observation of the neonates included
heart rate (EKG), blood pressure (BP), SaO2, transcutaneous CO2 (TcCO2), and ventilation
parameters such as positive inspiratory pressure (PiP), breathing frequency (f), fraction of
inspired oxygen (fiO2), and tidal volume (VT). These parameters have been recorded by the
investigator for analyzing purposes.
Figure 23 Examination course in infants with assisted ventilation, *CP= control period
Auto-trans-fusion
5’
*CP
5’
Supine Position PEEP decrease
1 cm H2O 15’
Supine Position PEEP increase
2 cm H2O 15’
Supine Position PEEP decrease
1 cm H2O 15’
Supine Position PEEP at preset
level 15’

46
2.5 Analyzing Data – Procedure Instruction
2.5.1 How to Detect Tidal Impedance Changes?
A special algorithm has been designed by EMS Biomedical to detect the height of tidal
impedance amplitudes. Distinction between small tidal impedance changes and cardiovascular
changes may be sometimes hard, cardiovascular changes need to be further studied to define a
limit value for cardiovascular changes which are overall the smaller impedance changes.
Fig 24- Fig 26 display different shapes of tidal impedance changes observed during our
investigations.
Figure 24 Scheme of normal breathing pattern in a newborn. The high amplitudes reflect the gas exchange resulting as tidal volume, the small amplitudes show curves resulting from cardiovascular changes. TidI = tidal impedance, cvaI= impedance of cardiovascular changes, resI= residual impedance Thoracic changes are dynamic changes and in some infants tidal impedance changes and
cardiovascular changes may simply overlap as shown in Fig 25 and Fig 26. Even this is a
physiologic phenomenon; it is probably one of the challenges for EIS devices to become an
adequate monitoring tool.
Figure 25 Breathing pattern in a spontaneously breathing infant. Tidal impedance changes and cardiovascular impedance changes may overlap as thoracic impedance changes are dynamic impedance changes.
tidI
cvaI
resI

47
Figure 26 Tidal impedance changes may primarily be regular and than become overlapping with cardiovascular changes.
2.5.2 From Record to Results: Spontaneously Breathing Infants
All measured data has been recorded by EIS Version 2.1 and was analysed by EIS Version
2.8. (For analyzing data EIS software had to be modified by EMS Biomedical to easily detect
the amplitudes of tidal volume.)
We evaluated data of 11 spontaneously breathing infants in this group. The infants have been
divided into three subgroups. (See “2.4.2 Patient Selection”) We examined the influence of
body position (supine position, left lateral position and prone position) on tidal volume and
functional residual capacity in all infants as well as the effect of autotransfusion on VT and
FRC. Bhat et al23 conducted a trial in which they studied the effect of body position on FRC
and lung mechanics such as compliance and resistance. They describe an increase of FRC in
oxygen-dependent premature infants depending on body position of the infant, but no
significant increase of FRC in non-oxygen dependent infants. None of our investigated infants
has been oxygen dependent.
We observed tidI and resI changes during our steps 1) supine postion, 2) left lateral position,
3) prone position, 4) autotransfusion, and 5) control period. (See “Fig 22, 2.4.8 Course of
Examination in Spontaneously Breathing Infants.”) We analyzed the 15th measured minute of
steps 1-3 and the 5th measured minute of step 4 and 5. According to movements of the infants
leading to artifacts in our impedance signal we had to adjust, and therefore we analyzed the
last minute clear of artifacts before the 15th minute/ 5th minute of each step. (See “2.5.8
Difficulty with Analyzing Data”)
IRREGULAR

48
Tidal Impedance
Tidal volume (VT) is reflected by tidal impedance (tidI) during our measurements.3 It has
been observed in all 4 quadrants of the lungs and the last minute of each step has been used
for analyzing purposes. To detect tidal impedance changes a special algorithm has been
developed for the software. The height of the amplitude which reflects tidal impedance varies
enormously within newborns of different sizes. During evaluation processes it can be adjusted
manually. Spontaneous breathing is not a totally regular breathing pattern neither in a healthy
newborn nor a grown up. Deeper or flatter breaths occur for several periods in infants which
do differ in frequency as well. In a newborn a breathing frequency of 35- 60 is considered
“normal” meaning average.41
Fig 27 shows tidal impedance changes of the lower right segment of the lungs in a
spontaneously breathing 1.5kg infant over a 10 second period. Single tidal volumes within the
spontaneously breathing patient differs more in height and frequency than in infants receiving
assisted ventilation. In infants with CMV breathing frequency would be given by the
ventilator and therefore totally regular.
Figure 27 Tidal impedance changes of the lower right segment of the lungs in a spontaneously breathing 1.5kg infant.
Residual Impedance
Functional residual capacity is a main factor to reflect residual impedance (resI) during our
measurements. Regional FRC has not been studied yet in healthy newborns and reference data
of healthy newborns to compare those with data of infants suffering from any kind of
respiratory disease are still lacking until today. According to that less optimal situation, “least
harmful” ventilation cannot be applied in newborns until today. 21
Information about FRC in healthy term babies compared to sick term babies, FRC in healthy
(without any lung disease) premature babies compared to sick premature babies as well as
tidI tidI
49
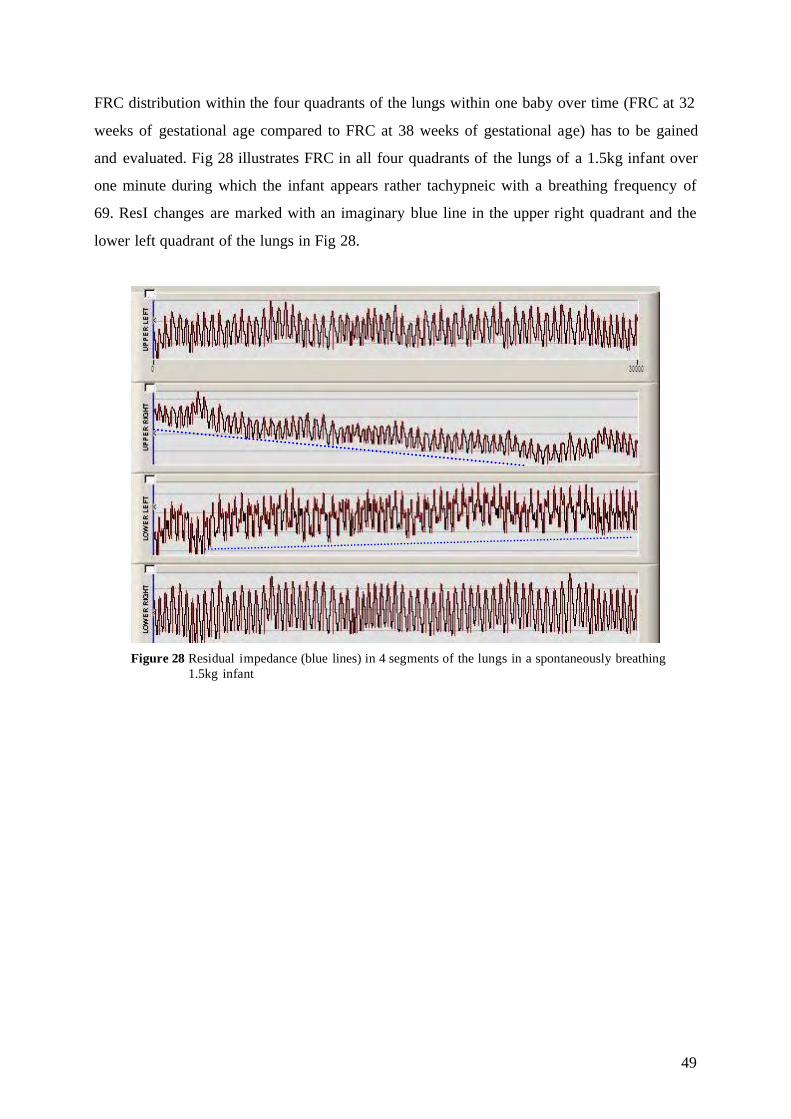
FRC distribution within the four quadrants of the lungs within one baby over time (FRC at 32
weeks of gestational age compared to FRC at 38 weeks of gestational age) has to be gained
and evaluated. Fig 28 illustrates FRC in all four quadrants of the lungs of a 1.5kg infant over
one minute during which the infant appears rather tachypneic with a breathing frequency of
69. ResI changes are marked with an imaginary blue line in the upper right quadrant and the
lower left quadrant of the lungs in Fig 28.
Figure 28 Residual impedance (blue lines) in 4 segments of the lungs in a spontaneously breathing 1.5kg infant
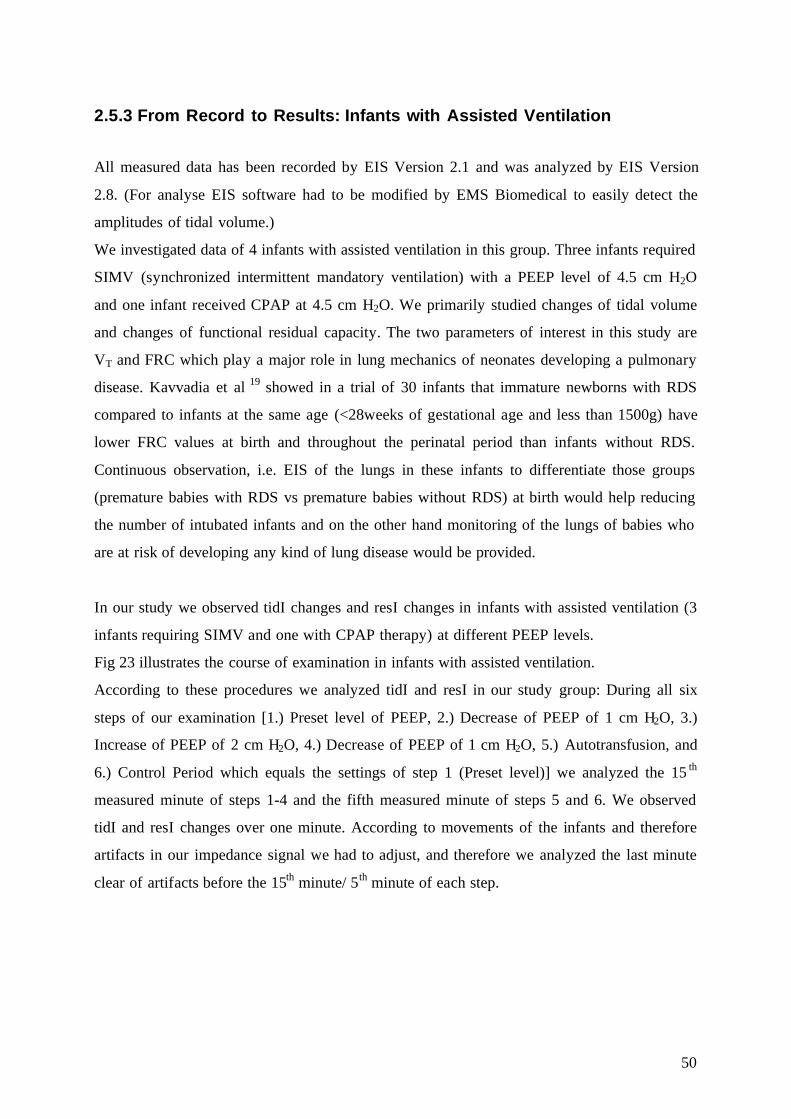
50
2.5.3 From Record to Results: Infants with Assisted Ventilation
All measured data has been recorded by EIS Version 2.1 and was analyzed by EIS Version
2.8. (For analyse EIS software had to be modified by EMS Biomedical to easily detect the
amplitudes of tidal volume.)
We investigated data of 4 infants with assisted ventilation in this group. Three infants required
SIMV (synchronized intermittent mandatory ventilation) with a PEEP level of 4.5 cm H2O
and one infant received CPAP at 4.5 cm H2O. We primarily studied changes of tidal volume
and changes of functional residual capacity. The two parameters of interest in this study are
VT and FRC which play a major role in lung mechanics of neonates developing a pulmonary
disease. Kavvadia et al 19 showed in a trial of 30 infants that immature newborns with RDS
compared to infants at the same age (<28weeks of gestational age and less than 1500g) have
lower FRC values at birth and throughout the perinatal period than infants without RDS.
Continuous observation, i.e. EIS of the lungs in these infants to differentiate those groups
(premature babies with RDS vs premature babies without RDS) at birth would help reducing
the number of intubated infants and on the other hand monitoring of the lungs of babies who
are at risk of developing any kind of lung disease would be provided.
In our study we observed tidI changes and resI changes in infants with assisted ventilation (3
infants requiring SIMV and one with CPAP therapy) at different PEEP levels.
Fig 23 illustrates the course of examination in infants with assisted ventilation.
According to these procedures we analyzed tidI and resI in our study group: During all six
steps of our examination [1.) Preset level of PEEP, 2.) Decrease of PEEP of 1 cm H2O, 3.)
Increase of PEEP of 2 cm H2O, 4.) Decrease of PEEP of 1 cm H2O, 5.) Autotransfusion, and
6.) Control Period which equals the settings of step 1 (Preset level)] we analyzed the 15 th
measured minute of steps 1-4 and the fifth measured minute of steps 5 and 6. We observed
tidI and resI changes over one minute. According to movements of the infants and therefore
artifacts in our impedance signal we had to adjust, and therefore we analyzed the last minute
clear of artifacts before the 15th minute/ 5th minute of each step.
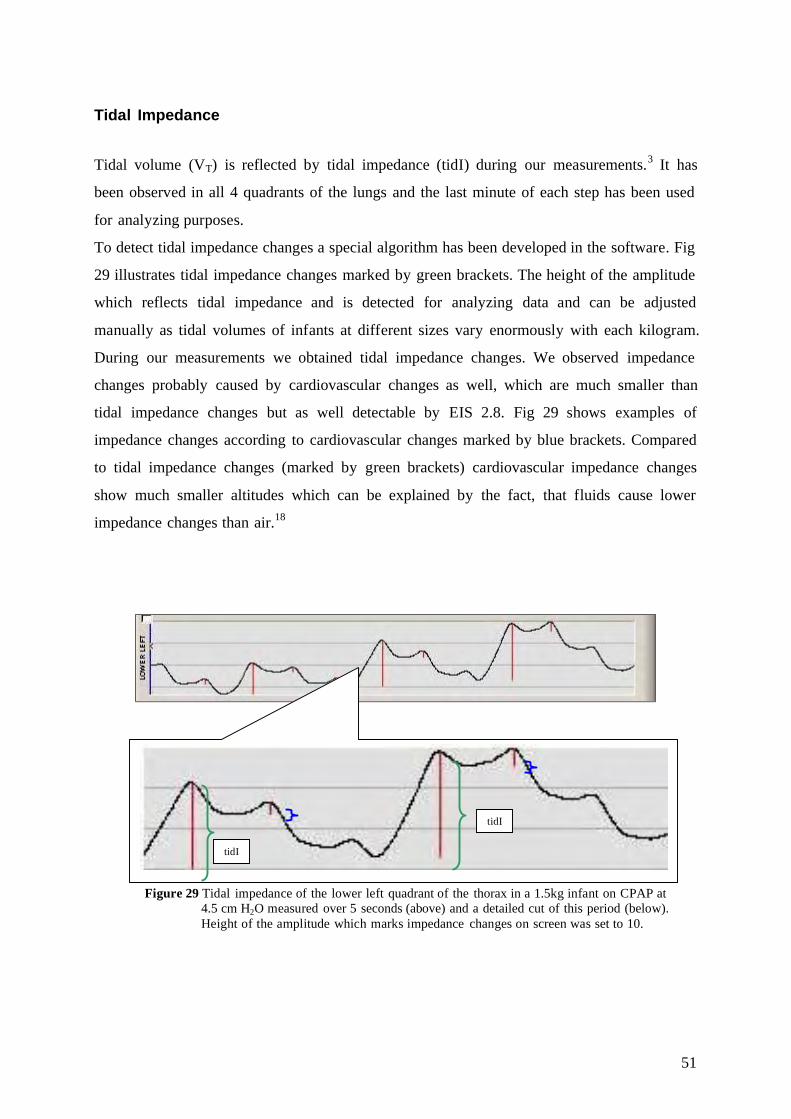
51
Tidal Impedance
Tidal volume (VT) is reflected by tidal impedance (tidI) during our measurements.3 It has
been observed in all 4 quadrants of the lungs and the last minute of each step has been used
for analyzing purposes.
To detect tidal impedance changes a special algorithm has been developed in the software. Fig
29 illustrates tidal impedance changes marked by green brackets. The height of the amplitude
which reflects tidal impedance and is detected for analyzing data and can be adjusted
manually as tidal volumes of infants at different sizes vary enormously with each kilogram.
During our measurements we obtained tidal impedance changes. We observed impedance
changes probably caused by cardiovascular changes as well, which are much smaller than
tidal impedance changes but as well detectable by EIS 2.8. Fig 29 shows examples of
impedance changes according to cardiovascular changes marked by blue brackets. Compared
to tidal impedance changes (marked by green brackets) cardiovascular impedance changes
show much smaller altitudes which can be explained by the fact, that fluids cause lower
impedance changes than air.18
Figure 29 Tidal impedance of the lower left quadrant of the thorax in a 1.5kg infant on CPAP at 4.5 cm H2O measured over 5 seconds (above) and a detailed cut of this period (below). Height of the amplitude which marks impedance changes on screen was set to 10.
tidI
tidI

52
Residual Impedance
Functional residual capacity (FRC) may be reflected by residual impedance (resI) marked by
the green arrows in Fig 30. Residual impedance is the minimal impedance measured.
Minimal impedance is mostly caused by changes of lung air volume, as air has the highest
impedance18, even tough changes in fluids (i.e. feeding of the baby) may have an impact on
minimal impedance and have to be further investigated. Information about FRC is mainly
important to adequately ventilate infants and to properly adjust PEEP levels to the infant’s
needs.21
Figure 30 Displays an imaginary line to demonstrate the change of residual impedance in the lower left segment of the lungs in a 1.5kg infant over 5 seconds
Fig 31 represents resI of all four quadrants of the lungs at the same time over 5 seconds in the
same baby as above with CPAP. ResI changes are tagged with an imaginary line (blue line) to
easier detect minimal impedance changes. In this picture minimal impedance of the upper left,
the lower left, and the lower right quadrant are increasing while resI in the upper right
quadrant first was increasing followed by a decrease of resI.

53
Figure 31 Impedance changes in 4 segments of the lungs in a 1.5kg infant on CPAP Fig 32 illustrates tidal impedance changes and constant residual impedance over one minute
in the upper left quadrant of the lungs. In this picture tidal impedance changes can be easily
detected and a frequency of 17 breaths per minute correlated with the observed ventilator
setting (SIMV) of a frequency of 17 in this 3.2kg asphyxiated newborn. 42 cardiovascular
changes can be detected during that one minute period, there are for sure again about the same
amount of unseen cardiovascular impedance changes which are overlaid by tidal impedance
changes. Still, an observed total of 88 heart beats per minute in that infant may correlate with
the recorded number of cardiovascular changes.
Upper left quadrant
Upper right quadrant
Lower left quadrant
Lower right quadrant
EKG
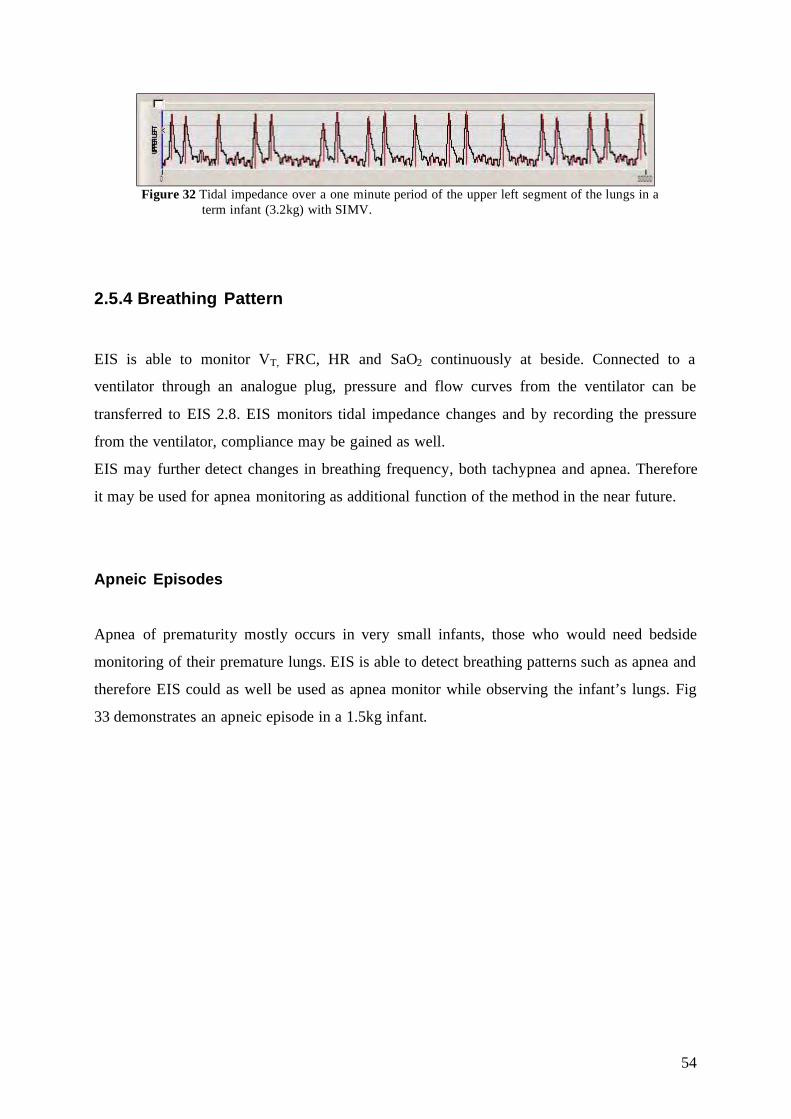
54
Figure 32 Tidal impedance over a one minute period of the upper left segment of the lungs in a
term infant (3.2kg) with SIMV.
2.5.4 Breathing Pattern
EIS is able to monitor VT, FRC, HR and SaO2 continuously at beside. Connected to a
ventilator through an analogue plug, pressure and flow curves from the ventilator can be
transferred to EIS 2.8. EIS monitors tidal impedance changes and by recording the pressure
from the ventilator, compliance may be gained as well.
EIS may further detect changes in breathing frequency, both tachypnea and apnea. Therefore
it may be used for apnea monitoring as additional function of the method in the near future.
Apneic Episodes
Apnea of prematurity mostly occurs in very small infants, those who would need bedside
monitoring of their premature lungs. EIS is able to detect breathing patterns such as apnea and
therefore EIS could as well be used as apnea monitor while observing the infant’s lungs. Fig
33 demonstrates an apneic episode in a 1.5kg infant.
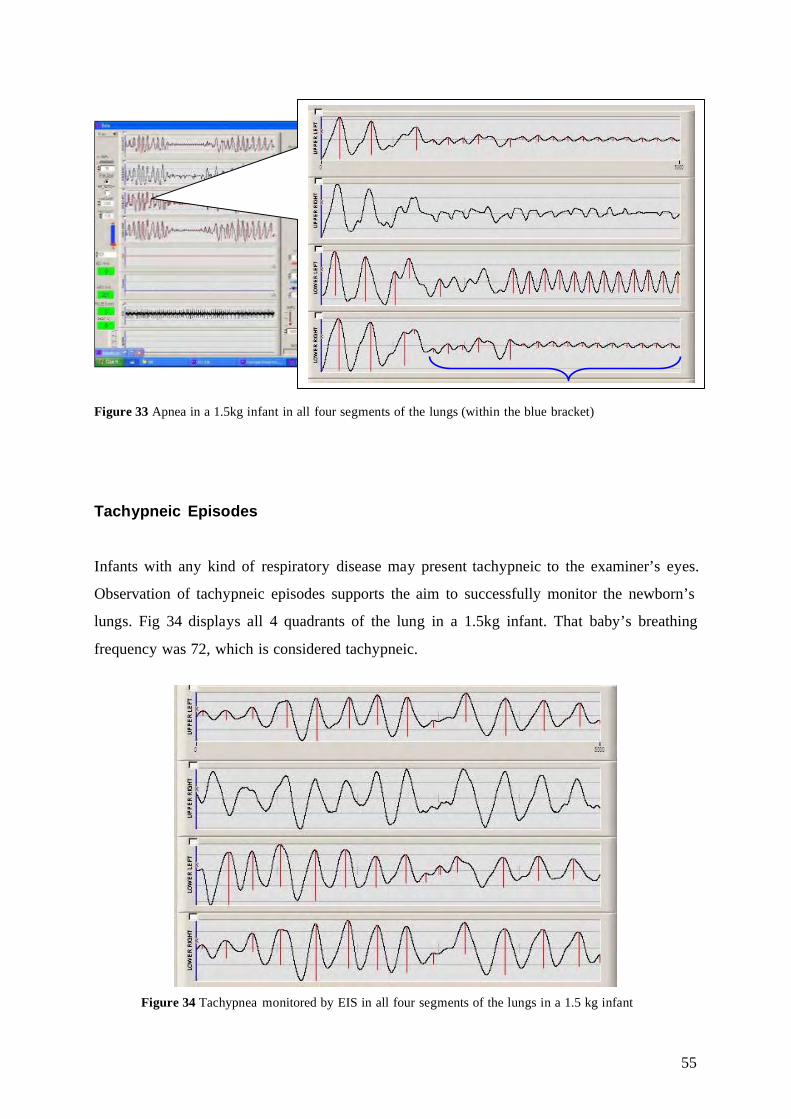
55
Figure 33 Apnea in a 1.5kg infant in all four segments of the lungs (within the blue bracket)
Tachypneic Episodes
Infants with any kind of respiratory disease may present tachypneic to the examiner’s eyes.
Observation of tachypneic episodes supports the aim to successfully monitor the newborn’s
lungs. Fig 34 displays all 4 quadrants of the lung in a 1.5kg infant. That baby’s breathing
frequency was 72, which is considered tachypneic.
Figure 34 Tachypnea monitored by EIS in all four segments of the lungs in a 1.5 kg infant

56
Cardiovascular Impedance Changes
Dynamic changes of the thorax such as cardiovascular changes of the lungs may be detected
by EIS. Even tough fluids cause lower impedance changes than air18 we clearly observed
cardiovascular changes in our measurements, best seen during apneic episodes of the infants.
Fig 35 demonstrates cardiovascular changes in a 3.2kg infant requiring SIMV: Each curve of
our EIS measurement equals one heart beat of the EKG, correlation between these
observations is suggested.
Pulse pressure is determined by subtracting the diastolic pressure from the systolic pressure. A
wide pulse pressure usually occurs in patients with aortiovenous malformations, aortic
insufficiency, and arteriopulmonary connections such as patent ductus arteriosus (PDA).
Aortic stenosis and congestive heart failure (CHF) may cause a narrow pulse pressure.22
Further investigations have to be performed to study cardiovascular impedance changes and
its significance and its correlation with pulse pressure.
Figure 35 Cardiovascular impedance changes mostly in the upper left and lower right segment of the lungs in a 3.2kg newborn with SIMV
Upper left quadrant
Upper right quadrant
Lower left quadrant
Lower right quadrant
EKG
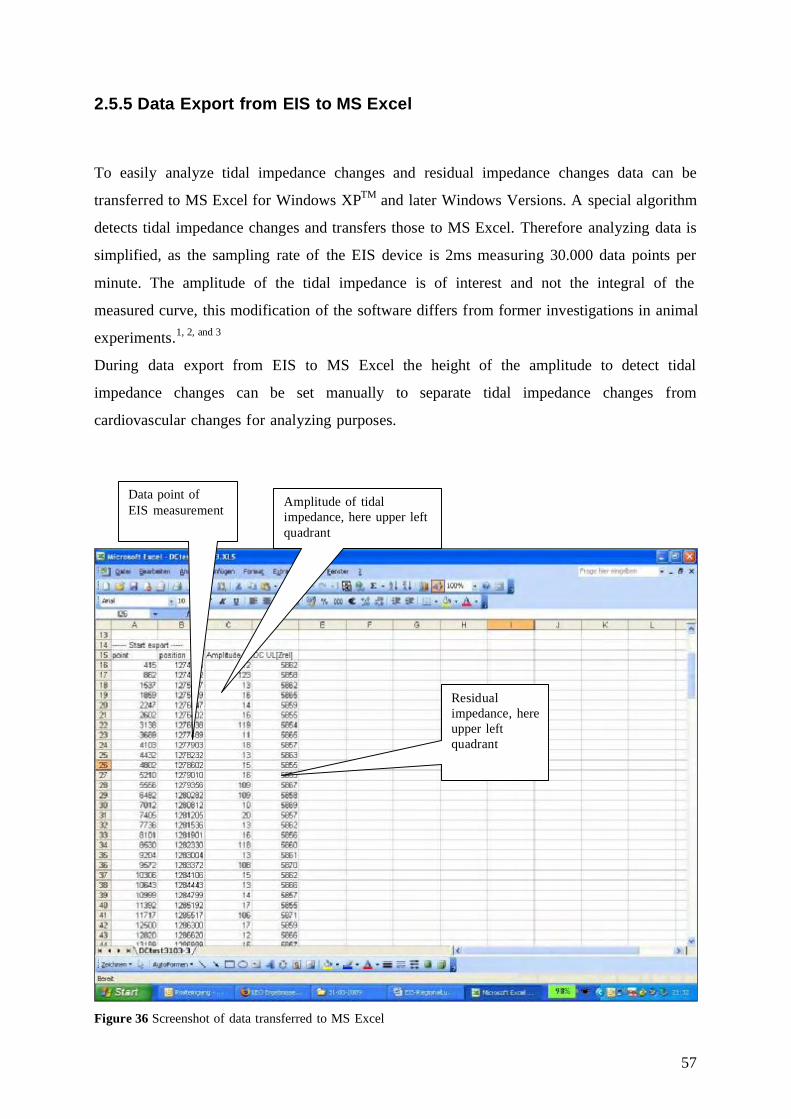
57
2.5.5 Data Export from EIS to MS Excel
To easily analyze tidal impedance changes and residual impedance changes data can be
transferred to MS Excel for Windows XPTM and later Windows Versions. A special algorithm
detects tidal impedance changes and transfers those to MS Excel. Therefore analyzing data is
simplified, as the sampling rate of the EIS device is 2ms measuring 30.000 data points per
minute. The amplitude of the tidal impedance is of interest and not the integral of the
measured curve, this modification of the software differs from former investigations in animal
experiments.1, 2, and 3
During data export from EIS to MS Excel the height of the amplitude to detect tidal
impedance changes can be set manually to separate tidal impedance changes from
cardiovascular changes for analyzing purposes.
Figure 36 Screenshot of data transferred to MS Excel
Amplitude of tidal impedance, here upper left quadrant
Residual impedance, here upper left quadrant
Data point of EIS measurement
58
Data transferred to MS Excel has been analyzed as mentioned above (See “2.5.2 From Record
to Results: Infants with Assisted Ventilation) and evaluated according to the group the infant
has been assigned to. (See “III. Results”)
Patient information such as body weight, current weight, gestational age, diseases and
treatment may be included in the MS Excel export file.
Data was transferred from EIS to MS Excel 2003 and has been analyzed in MS Excel 2003,
mean values and standard deviations have been calculated for examination periods in every
infant in this study. For statistical analysis SPSS 13.0 for Windows has been applied.
Statistical methods to analyze data included a two-tailed paired student’s t-test and Pearson
Correlation. A p value <0.05 has been considered as statistical significant, a p value <0.001 as
highly significant. According to the small number of patients in this study, especially in the
subgroups of the spontaneously breathing infants, validity of statistical analysis of these data
remains limited. To determine correlation between impedance changes and body weight
Peasron Correlation has been used, r= 0.5-0.7 has been considered as weak correlation, while
for a strong correlation r= 0.7-1.0 has been required.
Fig 37 to Fig 50 show an example of tidal impedance changes throughout a whole
examination period. In these pictures every 50th data point is printed out, leading to 600
datapoints printed per minute, this 3.2kg infant with assisted ventilation (SIMV) has been
measured over ninety minutes. The figures demonstrate the amount of data gained by EIS. In
this infant, tidal impedance of the upper left segment and lower right segment were higher
than tidal impedance changes in the upper right segment and lower left segment of the lungs.
[Yellow line= upper left segment, red line= upper right segment, blue line= lower left
segment and green line= lower right segment of the thorax]

59
Figure 37 Figure 38
Figure 39 Figure 40
Figure 41 Figure 42

60
Figure 43 Figure 44
Figure 45 Figure 46
Figure 47 Figure 48

61
Figure 49 Figure 50

62
2.5.6 Filtered Data versus Unfiltered Data
Different filters have been developed by EMS Biomedical for the EIS software. These filters
include:
1) Running Filter:
Band pass filter and high pass filter: High pass filter is applied to allow more precise
measurements of the amplitudes, while band pass filter suppresses artifacts resulting
from cardiovascular changes. These filters can be adjusted during measurements and
during reviewing data without having any impact on raw data.
2) Acquisition Filter:
Acquisition filter influence raw data and affect respiratory frequency.
3) Flow Filter:
Determine recorded flow data from the respirator.
4) Pressure Filter:
Determine recorded pressure data from the respirator.
5) ECG Filter:
Determine recorded ECG data.
In our pilot study we abandoned from adjusting any filter to our measurements to clearly
detect, observe, and evaluate raw data. To enable meaningful comparisons between
techniques and different research groups of reference data in the field of neonatal pulmonary
research, published results should be presented as raw data.21 This is especially true by
introducing a new monitoring tool i.e. EIS into neonatal care, filters may not only detect
formerly unseen data (e.g. suppress cardiovascular changes to precisely show tidal impedance
changes), but blur formerly seen raw data. All filters have been used in their factory setting.
2.5.7 Self- Adhesive Electrodes
In former animal experiments1, 2 and 3 needle electrodes have been chosen for electrical
impedance measurements. For infants needle electrodes cannot be used as they are pierced
into the skin. Besides the fact that they are applied invasively, they would be a source of
infection and especially in premature infants infection has to be kept low. Therefore we chose
63
self-adhesive electrodes Blue Sensor, BRS-50-k by Ambu®, Denmark. The advantage of self-
adhesive electrodes is that they are not attached invasively to the thorax. Surface constitution
i.e. skin of the thorax plays a major role in freezing of the electrodes. Lotions and any
substance which produces a fatty skin have to be avoided before applying the electrodes to the
infant’s thorax. Disadvantage of the self-adhesive electrodes is that their impedance signal
will never be as good as with needle electrodes. Blue Sensor, BRS-50-k self adhesive
electrodes are an option for EIS but not necessarily the best option, but surely a good option
and other self-adhesive electrodes may to be tested. We chose Blue Sensor, BRS-50-k by
Ambu® Denmark because of their translucency on x-ray and their small size. (1.6x 1.9cm)
Gold disc electrodes would be another option for EIS measurements. They could be sewed in
an electrode vest or electrode onesie to be quickly and properly applied. (See “2.4.6 Electrode
Vest” and “2.4.7 Electrode Onesie”)
2.5.8 Mirrored Impedance Signals
During our measurements we observed impedance signals which we named “mirrored
impedance signals” according to their appearance on screen. We disclosed this kind of
impedance signals in EIS measurements in several children but not all of the infants and not
during the whole examination course. First it was suggested that mirrored signals occur
according to misplaced electrodes. As we detected these signals only over periods during our
measurements and not constantly during the whole examination (which must be seen in the
case of a misplacement), it may be caused by the self-adhesive electrodes as the one or other
may become “bad” during measurements. Electrolyte concentrations of the skin may vary
within the patients on the surface of their skin, so different potentials are detected by the
electrodes which may lead to “mirrored” (=negative) signals if the signal itself is very small.
The software EIS 2.8 has been adapted by EMS Biomedical to invert mirrored impedance
signals. Further investigations have to be made to identify the origin of this phenomenon.
Fig. 51 is a good example of a period of mirrored impedance signals in the upper right and
lower left quadrant of the lungs.

64
Figure 51 Mirrored impedance signals in the upper right and lower left segment of the lungs in a 3.2 kg infant with SIMV.
2.5.9 Difficulty with Analyzing Data
Motion Artifacts
Spontaneously breathing newborn infants as well as ventilated, non sedated infants move their
heads, and mostly limbs on a regularly basis. These movements caused artifacts during our
measurements. Motion artifacts can be easily detected as a deviation of the impedance signal
occurs. Movements and hiccups of the baby are source of irritation of the impedance signal.
For analyzing purposes in this study we had to exclude these periods from our evaluation.

65
Breathing Frequency
Breathing frequency differs within humans not just newborns and is influenced by many
factors such as pain, fever, and sleep. Furthermore breathing frequency is not regular within
the mentioned states of neither newborns or grown ups. Our aim is to develop a method to
observe newborns’ lungs at beside as a monitoring tool from the delivering room to discharge
or at least until dissolving of respiratory diseases during hospital stay. Therefore there is a
need for a monitoring tool which not only observes lungs of ventilated infants which would
only have regular breaths. It is easier to develop a method to detect regular breaths than
irregular and this feature needs accurate attention. Only infants on ventilators have regular
breaths determined by the machine. As the number of infants on ventilators is further
decreasing according to the success of CPAP therapy in infants with respiratory diseases, a
tool to monitor the lungs from the beginning is of major interest. Respiratory distress does not
primarily occur at birth but within the first 72 hours of life. Prematurely born infants and
infants with assisted ventilation are always at risk of developing pneumothorax, a life
threatening condition which cannot monitored until today. 55

66
III. Results
3.1 Spontaneously Breathing Infants
In our study we examined 11 spontaneously breathing infants with a mean body weight of
2659g (± 903) on the day of examination. According to the range of body weight, we assigned
11 newborns to 3 subgroups. (See “2.4.2 Patient Selection”) In each group infants have been
examined in supine position, left lateral position, and prone position as well as during
autotransfusion followed by a control period. (See “2.4.6 Examination Course”)
As we were interested in the distribution of both tidal impedance and residual impedance
within the thorax, total tidal impedance and total residual impedance observed during each
examination period have been set to 100% and regional tidal impedance and regional residual
impedance have been calculated according to this. Unless otherwise noted all graphs display
distribution given in percent (%) of either total tidal impedance or total residual impedance
within the thorax.
3.1.1 Group I: Infants Weighing 1.5- 2.0kg
In this study group we investigated three premature infants at 31,3 (±0,57) weeks of
gestational age and a body weight of 1690g (±186) on the day of examination. According to
our examination course all infants have been examined in supine position, left lateral position,
and prone position and during autotransfusion followed by a control period. Investigated
parameters of interest are tidal impedance changes and residual impedance changes.
Tidal Impedance
We studied the distribution of tidal impedance in the four segments of premature infants and
observed the following findings:
Tidal impedance distribution of the lower right segment showed a mean (±SD) of 49,66%
(±10,01), followed by the upper left segment with a tidal impedance distribution of 34,33%

67
(±6,65). In the lower left segment we observed a tidal impedance of 10,33 (±2,08) and the
upper right segment had the lowest tidal impedance with 5,10% (±4,18).
According to our hypothesis we expect the lower right segment to display the highest tidal
impedance changes, therefore significance of all three other segments compared to the lower
right segment have been tested. Lower right segment showed higher mean tidal impedance
than the upper left segment; although by statistical analysis a p-value of 0,251 was detected
not significant. Unlike upper left segment, upper right segment (p= 0,031) and lower left
segment (p=0,019) had significantly lower tidal impedance changes than the lower right
segment. Fig 52 demonstrates tidal impedance distribution of all 4 segments in supine
position.
Lower RightLower LeftUpper RightUpper Left
70
60
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f TTI
Figure 52 Tidal impedance changes in spontaneously breathing infants with a mean body weight of 1690g. (n=3) Table 2 demonstrates the mean (±SD) of tidal impedance distribution within the thorax of
three spontaneously breathing infants during all examination periods.
Tidal Impedance Distribution within the Thorax (Mean ±SD)
Upper left segment
Upper right segment
Lower left segment
Lower right segment
Supine Position 34,3 % (±6,65) 5,10 % (±4,18) 10,33 % (±2,08) 49,66 % (±10,01) Autotransfusion 33,33 % (±3,05) 5,8 % (±4,69) 8,67 % (±3,21) 52 % (±10,44) Control Period 36 % (±5,29) 6,77 % (±5,58) 8,33 % (±3,78) 48,66 % (±14,22) Left Side Position
38,33 % (±17,92) 10,26 % (±10,78) 10,33 % (±5,5) 23,25 % (±13,42)
Prone Position 39 % (±7) 6,8 % (±5,54) 8,33 % (±4,5) 45,66 % (10,21) Table 2 Tidal impedance changes within the thorax in spontaneously breathing infants with a mean body weight of 1690g.
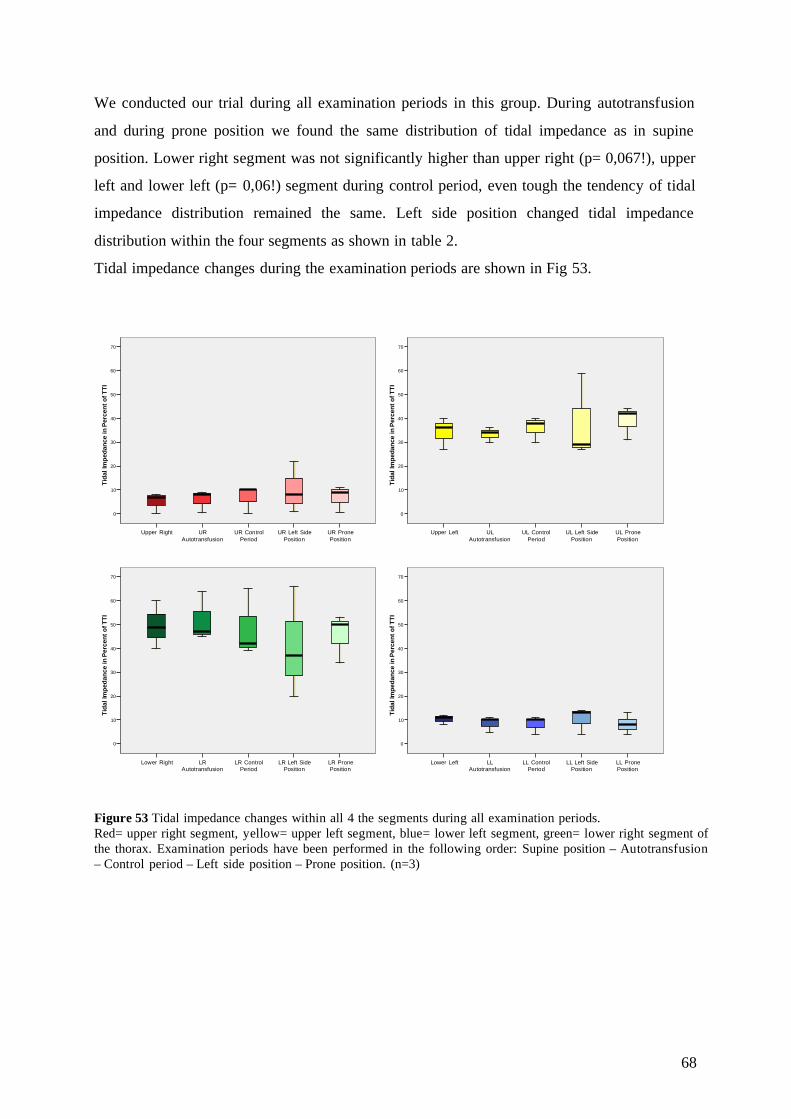
68
We conducted our trial during all examination periods in this group. During autotransfusion
and during prone position we found the same distribution of tidal impedance as in supine
position. Lower right segment was not significantly higher than upper right (p= 0,067!), upper
left and lower left (p= 0,06!) segment during control period, even tough the tendency of tidal
impedance distribution remained the same. Left side position changed tidal impedance
distribution within the four segments as shown in table 2.
Tidal impedance changes during the examination periods are shown in Fig 53.
UR PronePosition
UR Left SidePosition
UR ControlPeriod
URAutotransfusion
Upper Right
70
60
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f TTI
UL PronePosition
UL Left SidePosition
UL ControlPeriod
ULAutotransfusion
Upper Left
70
60
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f TTI
LR PronePosition
LR Left SidePosition
LR ControlPeriod
LRAutotransfusion
Lower Right
70
60
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f TTI
LL PronePosition
LL Left SidePosition
LL ControlPeriod
LLAutotransfusion
Lower Left
70
60
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f TTI
Figure 53 Tidal impedance changes within all 4 the segments during all examination periods. Red= upper right segment, yellow= upper left segment, blue= lower left segment, green= lower right segment of the thorax. Examination periods have been performed in the following order: Supine position – Autotransfusion – Control period – Left side position – Prone position. (n=3)

69
Residual Impedance
Residual impedance has been investigated during all examination periods and in all infants of
this group. We found the following distribution of residual impedance within the thorax in
supine position: The upper right segment showed the highest residual impedance changes
with a mean (±SD) of 28,33% (±3,78). Lower right and upper left segment tidal impedance
distribution were close with 27% (±2) in the lower right segment, and 24,66% (±5,68) in the
upper left segment. In the lower left segment we observed a residual impedance of 20%
(±3,6).
In supine position only residual impedance in the lower left segment (20%) was significantly
lower than in the upper right (28,33%) segment with p=0,011.
Fig 54 illustrates residual impedance distribution within the thorax of all four segments in
supine position of the infant.
Lower RightLower LeftUpper RightUpper Left
60
50
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f Tot
al R
esI
Figure 54 Residual impedance distribution within all segments of the thorax in spontaneously breathing infants with a mean body weight of 1690g. (n=3)
Mean values (±SD) of residual impedance have been calculated for all four segments during
all examination periods and are displayed in Table 3.

70
Residual Impedance Distribution within the Thorax (Mean ±SD)
Upper left segment
Upper right segment
Lower left segment
Lower right segment
Supine Position 24,66 % (±5,68) 28,33 % (±3,78) 20 % (±3,6) 27 % (±2) Autotransfusion 22,33 % (±3,21) 29,33 % (±1,15) 23,66 % (±0,57) 24,66 % (±1,52) Control Period 22,66 % (±4,72) 30,33 % (±1,52) 21,33 % (±2,88) 25,66 % (±2,08) Left Side Position
33,66 % (±18,47) 25 % (±8,18) 20 % (±7,54) 21,33 % (±6,02)
Prone Position 24,33 % (±6,65) 27,66 % (±4,93) 20,66 % (±5,85) 27 % (±3,6) Table 3 Residual impedance changes within the thorax in spontaneously breathing infants with a mean body weight of 1690g. During our examination periods we noticed the following residual impedance distribution: In
supine position upper right segment was significantly higher than lower left segment (also
see “3.1.3 Group III: Infants weighing more than 3kg”) with p=0,011. During
autotransfusion upper right segment (29,33%) was significantly higher than lower left
segment (23,66%) with p=0,003 and lower right segment (24,66%) with p=0,006. On contrary
control period showed residual impedance distribution as already monitored in supine
position, upper right segment (30,33%) was only significantly higher than upper left segment
(22,66%) with p=0,016. We did not detect any significance of residual impedance distribution
in left side position and prone position, with one exemption: In prone position residual
impedance showed a significantly higher tidal impedance distribution of the upper right
segment (27,66%) once again than lower left segment (20,66%) with p=0,02.
Fig 55 displays residual impedance distribution within the thorax during all examination
periods.

71
UR PronePosition
UR Left SidePosition
UR ControlPeriod
URAutotransfusion
Upper Right
60
50
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f To
tal R
esI
UR PronePosition
UL Left SidePosition
UL ControlPeriod
ULAutotransfusion
Upper Left
60
50
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f To
tal R
esI
LR PronePosition
LR Left SidePosition
LR ControlPeriod
LRAutotransfusion
Lower Right
60
50
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f To
tal R
esI
LL PronePosition
LL Left SidePosition
LL ControlPeriod
LLAutotransfusion
Lower Left
60
50
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f To
tal R
esI
Figure 55 Residual impedance changes within all 4 the segments during all examination periods. Red= upper right segment, yellow= upper left segment, blue= lower left segment, green= lower right segment of the thorax. Examination periods have been performed in the following order: Supine position – Autotransfusion – Control period – Left side position – Prone position. (n=3)

72
3.1.2 Group II: Infants Weighing 2.0- 2.5kg
We studied three infants in this group at 31,66 (±0,57) weeks of gestational age and a mean
body weight of 2200g (±187) on the day of examination. Parameters of interest were tidal
impedance and residual impedance during our examination periods supine position, left lateral
position, and prone position as well as autotransfusion followed by a control period.
Tidal Impedance Tidal impedance distribution has been tested and we detected the following results:
In supine position lower right segment showed the highest tidal impedance distribution with
a mean (±SD) of 40% (±6,08), upper left segment displayed 34,66% (±5,68), lower left
segment had a tidal impedance distribution of 14% (±2) and upper right segment was lowest
with a tidal impedance distribution of 11,66% (±3,51).
Fig 56 illustrates tidal impedance distribution of all 4 segments in supine position.
Lower RightLower LeftUpper RightUpper Left
70
60
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f TT
I
Figure 56 Tidal impedance distribution of all 4 segments of the thorax in spontaneously breathing infants with a mean body weight of 2200g (n=3) Tidal impedance distribution of the lower right segment was not significantly higher than tidal
impedance distribution of the upper left segment (p=0,513). Upper right segment was
significantly lower than lower right segment, with p=0,020. Nearly the same tidal impedance
distribution was observed in lower left segment, which was significantly lower than tidal
impedance distribution with p=0,021.

73
Table 4 states tidal impedance distribution within the thorax during all examination periods.
Tidal Impedance Distribution within the Thorax (Mean ±SD)
Upper left segment
Upper right segment
Lower left segment
Lower right segment
Supine Position 34,66 % (±5,68) 11,66 % (±3,51) 14 % (±2) 40 % (±6,08) Autotransfusion 39 % (±9,53) 11 % (±3,6) 16,33 % (±6,8) 34,33 % (±8,96) Control Period 37,66 % (±4,5) 11,66% (±3,51) 17,33 % (±8,73) 33,66 % (±6,02) Left Side Position
30 % (±14,1) 10 % (±6) 16 % (±2,64) 43,33 % (±15,27)
Prone Position 28,66 % (±16,5) 10,33 % (±8,62) 13,66 %(±2,51) 47,66 % (±17,03) Table 4 Tidal impedance changes within the thorax in spontaneously breathing infants with a mean (±SD) body weight of 2200g.
During our examination periods autotransfusion, control period, left side position and
prone position we could not find further significance in tidal impedance distribution even our
results show a clear tendency. Lower right segment and upper left segment tidal impedance
are higher throughout all examination periods than upper right segment and lower left
segment. In this study group standard deviation appeared to be relatively high.
One exemption has been detected during control period where lower right segment was
significantly higher than upper right segment with p=0,041.
Fig 57 visualizes tidal impedance distribution of all four segments during our examination
periods.
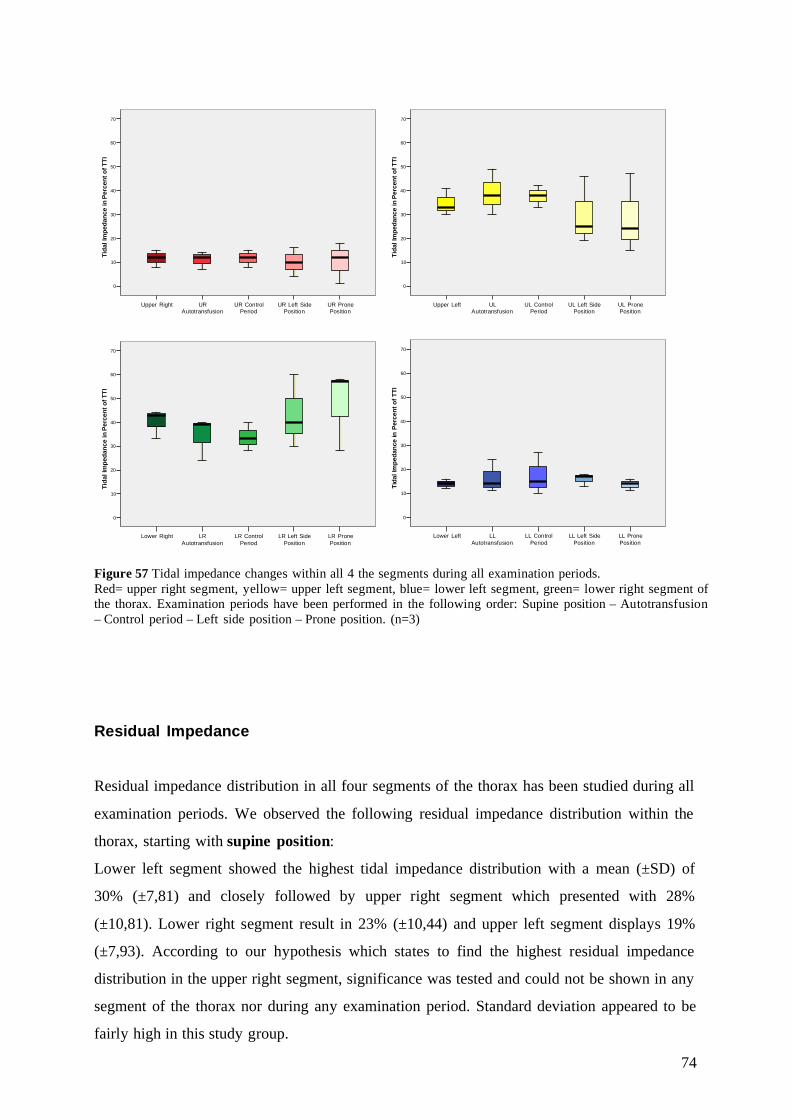
74
UR PronePosition
UR Left SidePosition
UR ControlPeriod
URAutotransfusion
Upper Right
70
60
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f TTI
UL PronePosition
UL Left SidePosition
UL ControlPeriod
ULAutotransfusion
Upper Left
70
60
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f TTI
LR PronePosition
LR Left SidePosition
LR ControlPeriod
LRAutotransfusion
Lower Right
70
60
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f TTI
LL PronePosition
LL Left SidePosition
LL ControlPeriod
LLAutotransfusion
Lower Left
70
60
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f TTI
Figure 57 Tidal impedance changes within all 4 the segments during all examination periods. Red= upper right segment, yellow= upper left segment, blue= lower left segment, green= lower right segment of the thorax. Examination periods have been performed in the following order: Supine position – Autotransfusion – Control period – Left side position – Prone position. (n=3)
Residual Impedance
Residual impedance distribution in all four segments of the thorax has been studied during all
examination periods. We observed the following residual impedance distribution within the
thorax, starting with supine position:
Lower left segment showed the highest tidal impedance distribution with a mean (±SD) of
30% (±7,81) and closely followed by upper right segment which presented with 28%
(±10,81). Lower right segment result in 23% (±10,44) and upper left segment displays 19%
(±7,93). According to our hypothesis which states to find the highest residual impedance
distribution in the upper right segment, significance was tested and could not be shown in any
segment of the thorax nor during any examination period. Standard deviation appeared to be
fairly high in this study group.
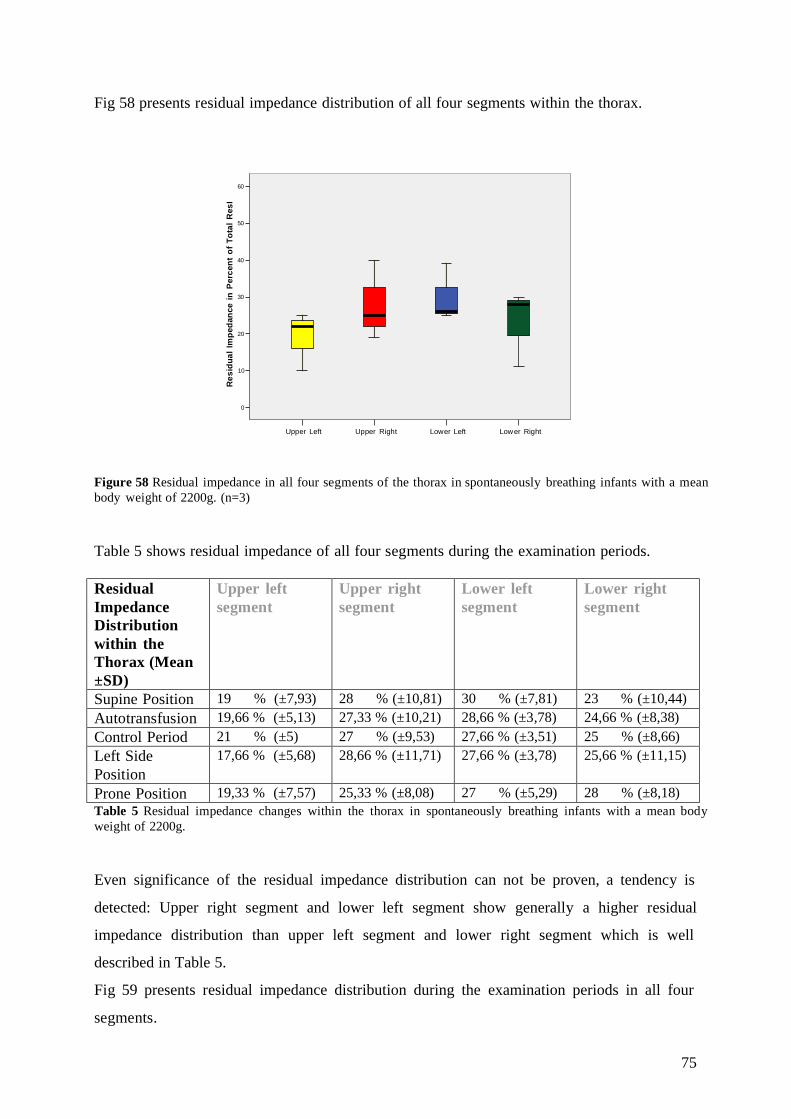
75
Fig 58 presents residual impedance distribution of all four segments within the thorax.
Lower RightLower LeftUpper RightUpper Left
60
50
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f Tot
al R
esI
Figure 58 Residual impedance in all four segments of the thorax in spontaneously breathing infants with a mean body weight of 2200g. (n=3)
Table 5 shows residual impedance of all four segments during the examination periods.
Residual Impedance Distribution within the Thorax (Mean ±SD)
Upper left segment
Upper right segment
Lower left segment
Lower right segment
Supine Position 19 % (±7,93) 28 % (±10,81) 30 % (±7,81) 23 % (±10,44) Autotransfusion 19,66 % (±5,13) 27,33 % (±10,21) 28,66 % (±3,78) 24,66 % (±8,38) Control Period 21 % (±5) 27 % (±9,53) 27,66 % (±3,51) 25 % (±8,66) Left Side Position
17,66 % (±5,68) 28,66 % (±11,71) 27,66 % (±3,78) 25,66 % (±11,15)
Prone Position 19,33 % (±7,57) 25,33 % (±8,08) 27 % (±5,29) 28 % (±8,18) Table 5 Residual impedance changes within the thorax in spontaneously breathing infants with a mean body weight of 2200g. Even significance of the residual impedance distribution can not be proven, a tendency is
detected: Upper right segment and lower left segment show generally a higher residual
impedance distribution than upper left segment and lower right segment which is well
described in Table 5.
Fig 59 presents residual impedance distribution during the examination periods in all four
segments.

76
UR PronePosition
UR Left SidePosition
UR ControlPeriod
URAutotransfusion
Upper Right
60
50
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f To
tal R
esI
UL PronePosition
UL Left SidePosition
UL ControlPeriod
ULAutotransfusion
Upper Left
60
50
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f To
tal R
esI
LR PronePosition
LR Left SidePosition
LR ControlPeriod
LRAutotransfusion
Lower Right
60
50
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f To
tal R
esI
LL PronePosition
LL Left SidePosition
LL ControlPeriod
LLAutotransfusion
Lower Left
60
50
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f To
tal R
esI
Figure 59 Residual impedance changes within all 4 the segments during all examination periods. Red= upper right segment, yellow= upper left segment, blue= lower left segment, green= lower right segment of the thorax. Examination periods have been performed in the following order: Supine position – Autotransfusion – Control period – Left side position – Prone position. (n=3)

77
3.1.3 Group III: Infants Weighing more than 3kg
We investigated five infants in this group, who were born at 38, 4 (±2,7) weeks of gestational
age and presented with a mean body weight of 3516g (±472) on the day of examination. In
this group we have monitored the same examination periods in four segments of the thorax.
Parameters of interest we investigated are tidal impedance distribution within the thorax and
residual impedance distribution.
Tidal Impedance
Tidal impedance distribution has been observed in five infants in supine position and during
all other examination periods four infants have been investigated. One infant has been
excluded from the study after supine position as the placing of electrodes has been switched
and therefore results gained from this infant differ from the other examined infants in this
group.
The following tidal impedance distribution has been detected in supine position: Highest
tidal impedance has been monitored in the lower right segment as all study groups with a
mean (±SD) of 44,15% (±11,3) closely followed by tidal impedance of the lower left segment
with 39,5% (±14,38). According to our hypothesis significance should be found between
those two segments, which did show no significance in tidal impedance distribution.
(p=0,647). On the contrary upper right segment showed a tidal impedance of 7,09% (±7,95),
which is significantly lower than tidal impedance of lower right segment with p=0,004. Lower
left segment in relation to lower right segment resulted with p=0,018, a significant lower tidal
impedance distribution. Fig 60 demonstrates these findings in supine position.

78
Lower RightLower LeftUpper RightUpper Left
70
60
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f TT
I
4
1
4
Figure 60 Tidal impedance in 4 segments of the thorax in spontaneously breathing infants with a mean body weight of 3516g (n=5) We examined the effect of body positions (left lateral position and prone position) as well
as the influence of autotransfusion followed by a control period on tidal impedance
distribution.
Table 6 illustrates tidal impedance distribution within the thorax during examination periods.
Tidal Impedance Distribution within the Thorax (Mean ±SD)
Upper left segment
Upper right segment
Lower left segment
Lower right segment
Supine Position 39,5 % (±14,38) 7,09 % (±7,95) 9,23 % (±10,58) 44,15 % (±11,30) Autotransfusion 29,01% (±9,08) 10,85 % (±2,02) 16,11%(±6,98) 43,75 % (±11) Control Period 34,68% (±11,17) 8,31 % (±3,64) 9,1 %(±3,85) 47,87 % (±12,63) Left Side Position
35,8 % (±3,36) 15,73 % (±9,93) 12,72%(±6,91) 35,4 % (±10,03)
Prone Position 30,61% (±16,06) 7,3 % (±3,18) 16,74%(±11,34) 45,33 % (±7,45) Table 6 Tidal impedance changes within the thorax in spontaneously breathing infants with a mean body weight of 3516g.
The significance in tidal impedance distribution remained during our examination periods,
tidal impedance of upper right segment and lower left segment were significantly lower than
tidal impedance of lower right segment (p <0,05). An exception occurred during left side

79
position in which no significance in tidal impedance distribution could be detected as p> 0,05
was observed. (UL-LRd: p=0,913; UR-LRe: p=0,135 and LL-LRf: p=0,061!)
Fig 61 visualizes tidal impedance distribution in all segments during examination periods.
UR PronePosition
UR Left SidePosition
UR ControlPeriod
URAutotransfusion
Upper Right
70
60
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f TT
I
UL PronePosition
UL Left SidePosition
UL ControlPeriod
ULAutotransfusion
Upper Left
70
60
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f TTI
LR PronePosition
LR Left SidePosition
LR ControlPeriod
LRAutotransfusion
Lower Right
70
60
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f TT
I
LL PronePosition
LL Left SidePosition
LL ControlPeriod
LLAutotransfusion
Lower Left
70
60
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f TT
I
Figure 61 Tidal impedance changes within all 4 the segments during all examination periods. Red= upper right segment, yellow= upper left segment, blue= lower left segment, green= lower right segment of the thorax. Examination periods have been performed in the following order: Supine position – Autotransfusion – Control period – Left side position – Prone position. (n=5 in supine position, n=4 in all other examination periods)
d UL-LR: upper left segment – lower right segment e UR-LR: upper right segment – lower right segment f LL-LR: lower left segment – lower right segment

80
Residual Impedance
Residual impedance was studied in this group during our examination periods and in four
segments of the thorax. Results showed the following in supine position:
Residual impedance was highest in the upper right segment with a mean (±SD) of 38,4%
(±5,02). Lower left segment displayed a tidal impedance of 33,8 % (±4,08). No significance
of residual impedance distribution could be described between these two segments with
p=0,249.
Upper left segment [13,6 % (±5,22)] was significantly lower than upper right segment with
p=0,004. Same observation has been made in lower right segment [14,2% (±1,78)],
significance was given with p=0,001.
Fig 62 presents these findings of residual impedance distribution in supine position of all four
segments.
Lower RightLower LeftUpper RightUpper Left
60
50
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f To
tal R
esI
2
Figure 62 Residual impedance in 4 segments of the thorax in spontaneously breathing infants with a mean body weight of 3516g (n=5) These distributions of residual impedance and therefore detection of significance (p< 0,05 in
upper left and lower right segment compared with upper right segment; p> 0,05 in lower left
segment compared with upper right segment) were true for all examination periods in this
study group of spontaneously breathing infants with a body weight higher than 3kg.
Table 7 presents residual impedance distribution during all examination periods and Fig 63
visualizes these findings.

81
Residual Impedance Distribution within the Thorax (Mean ±SD)
Upper left segment
Upper right segment
Lower left segment
Lower right segment
Supine Position 13,6 % (±5,22) 38,4 % (±5,02) 33,8 % (±4,08) 14,2 % (±1,78) Autotransfusion 11,5 % (±5,68) 37 % (±5,09) 35,25% (±6,18) 16 % (±5,71) Control Period 11 % (±4) 36,5 % (±3,1) 34,5 % (±6,02) 18,5 % (±5,91) Left Side Position
11,5 % (±6,4) 32,75% (±7,41) 33,75% (±4,85) 18,5 % (±1,73)
Prone Position 10,2 % (±3,68) 38 % (±4,96) 36,75% (±4,85) 15 % (±4,96) Table 7 Residual impedance changes within the thorax in spontaneously breathing infants with a mean body weight of 3516g.
UR PronePosition
UR Left SidePosition
UR ControlPeriod
URAutotransfusion
Upper Right
60
50
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f To
tal R
esI
UL PronePosition
UL Left SidePosition
UL ControlPeriod
ULAutotransfusion
Upper Left
60
50
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f Tot
al R
esI
LR PronePosition
LR Left SidePosition
LR ControlPeriod
LRAutotransfusion
Lower Right
60
50
40
30
20
10
0
Res
idua
l Im
pdan
ce in
Per
cent
of
Tota
l Res
I
LL PronePosition
LL Left SidePosition
LL ControlPeriod
LLAutotransfusion
Lower Left
60
50
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f To
tal R
esi
Figure 63 Residual impedance changes within all 4 the segments during all examination periods. Red= upper right segment, yellow= upper left segment, blue= lower left segment, green= lower right segment of the thorax. Examination periods have been performed in the following order: Supine position – Autotransfusion – Control period – Left side position – Prone position. (supine position n=5, all other examination periods n=4)
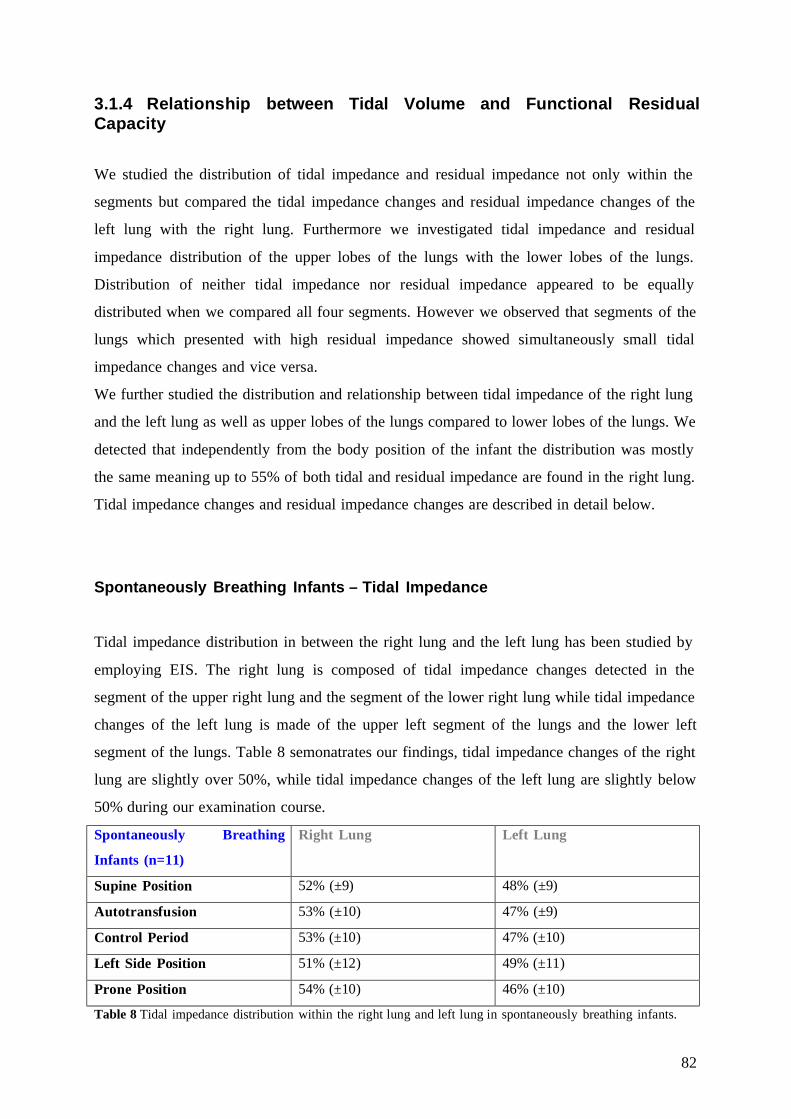
82
3.1.4 Relationship between Tidal Volume and Functional Residual Capacity
We studied the distribution of tidal impedance and residual impedance not only within the
segments but compared the tidal impedance changes and residual impedance changes of the
left lung with the right lung. Furthermore we investigated tidal impedance and residual
impedance distribution of the upper lobes of the lungs with the lower lobes of the lungs.
Distribution of neither tidal impedance nor residual impedance appeared to be equally
distributed when we compared all four segments. However we observed that segments of the
lungs which presented with high residual impedance showed simultaneously small tidal
impedance changes and vice versa.
We further studied the distribution and relationship between tidal impedance of the right lung
and the left lung as well as upper lobes of the lungs compared to lower lobes of the lungs. We
detected that independently from the body position of the infant the distribution was mostly
the same meaning up to 55% of both tidal and residual impedance are found in the right lung.
Tidal impedance changes and residual impedance changes are described in detail below.
Spontaneously Breathing Infants – Tidal Impedance
Tidal impedance distribution in between the right lung and the left lung has been studied by
employing EIS. The right lung is composed of tidal impedance changes detected in the
segment of the upper right lung and the segment of the lower right lung while tidal impedance
changes of the left lung is made of the upper left segment of the lungs and the lower left
segment of the lungs. Table 8 semonatrates our findings, tidal impedance changes of the right
lung are slightly over 50%, while tidal impedance changes of the left lung are slightly below
50% during our examination course.
Spontaneously Breathing
Infants (n=11)
Right Lung Left Lung
Supine Position 52% (±9) 48% (±9)
Autotransfusion 53% (±10) 47% (±9)
Control Period 53% (±10) 47% (±10)
Left Side Position 51% (±12) 49% (±11)
Prone Position 54% (±10) 46% (±10)
Table 8 Tidal impedance distribution within the right lung and left lung in spontaneously breathing infants.

83
We further studied the distribution in between the upper lobes of the lungs and the lower
lobes of the lungs. The upper lobes of the lungs are composed by the upper right segment and
the upper left segment while the lower lobes are defined by tidal impedance changes of the
lower right segment and the lower left segment of the lungs. Lower lobes presented with tidal
impedance changes around 55%, while upper lobes showed around 45%. In table 9 our results
are described in detail. During prone position tidal impedance changes seemed to be highest
in the lower segments (59%) during the whole examination course.
Spontaneously Breathing
Infants (n=11)
Upper Lobes Lower Lobes
Supine Position 45% (±7) 54% (±7)
Autotransfusion 43% (±10) 57% (±10)
Control Period 45% (±10) 55% (±10)
Left Side Position 46% (±13) 54% (±13)
Prone Position 41% (±12) 59% (±12)
Table 9 Tidal impedance distribution within the upper lobes and lower lobes of the lungs in spontaneously breathing infants.
Spontaneously Breathing Infants – Residual Impedance
Residual impedance has been investigated in between the right lung of the infant and the left
lung to observe tidal impedance distribution. Residual impedance of the right lungs appeared
to be slightly higher (up to 55%) than residual impedance of the left lung. Fig 10 illustrates
these findings during our examination periods. Residual impedance distribution remained
relatively stable independently from the position the infant has been placed in.
.
Spontaneously Breathing
Infants (n=11)
Right Lung Left Lung
Supine Position 53% (±4) 47% (±4)
Autotransfusion 53% (±2) 47% (±2)
Control Period 55% (±4) 45% (±3)
Left Side Position 52% (±8) 48% (±8)
Prone Position 54% (±3) 46% (±3)
Fig 10 Residual impedance distribution within the right lung and the left lung in spontaneously breathing infants.
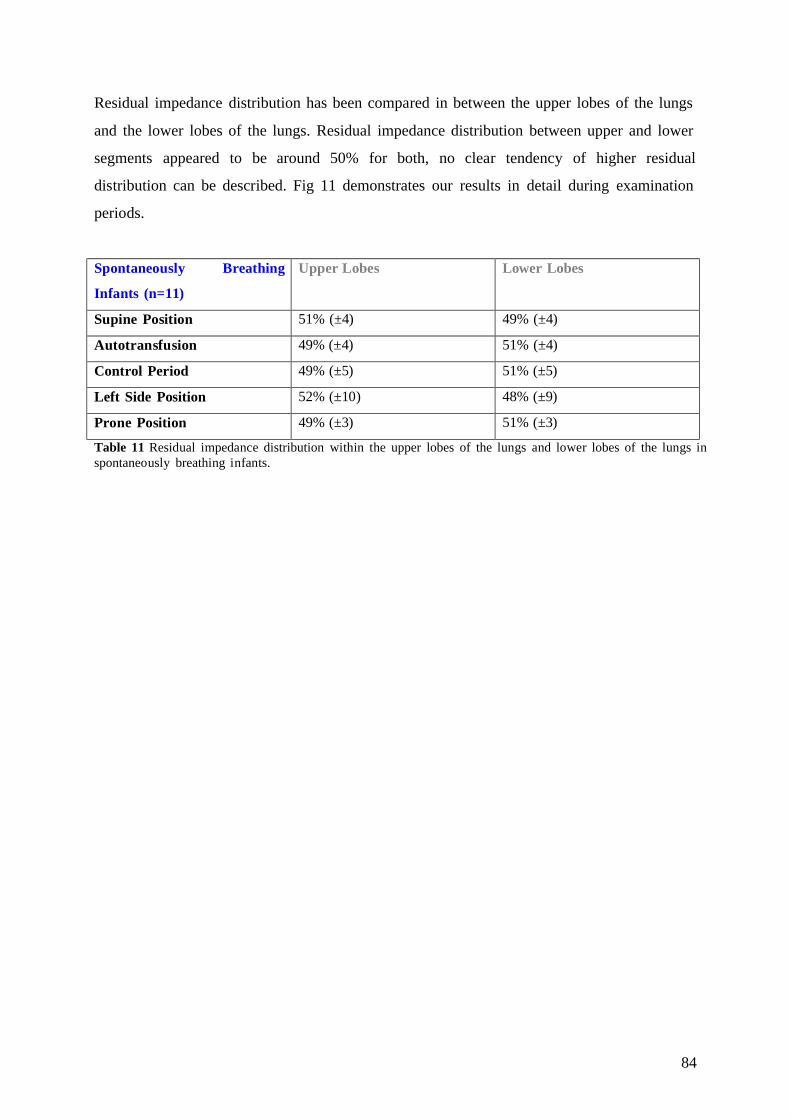
84
Residual impedance distribution has been compared in between the upper lobes of the lungs
and the lower lobes of the lungs. Residual impedance distribution between upper and lower
segments appeared to be around 50% for both, no clear tendency of higher residual
distribution can be described. Fig 11 demonstrates our results in detail during examination
periods.
Spontaneously Breathing
Infants (n=11)
Upper Lobes Lower Lobes
Supine Position 51% (±4) 49% (±4)
Autotransfusion 49% (±4) 51% (±4)
Control Period 49% (±5) 51% (±5)
Left Side Position 52% (±10) 48% (±9)
Prone Position 49% (±3) 51% (±3)
Table 11 Residual impedance distribution within the upper lobes of the lungs and lower lobes of the lungs in spontaneously breathing infants.

85
3.1.5 Summary of Spontaneously Breathing Infants We examined 11 spontaneously breathing infants with a body weight of 2659g (±903g) and a
gestational age of 35 weeks (±4). Tidal impedance and residual impedance have been
investigated and the infants have been studied as described above. (See “2.4.6 Course of
Examination”)
Tidal Impedance
In supine position we tested the distribution of tidal impedance within our 4 segments.
According to our hypothesis the highest tidal impedance changes are found in the lower right
segment of the lungs. A student’s t-test has been performed to test the significance of tidal
impedance distribution in all segments referring to the lower right segment.
In the upper left segment we found a mean (±SD) of 36,79 % (±10,24) and in the lower right
segment the mean was 44,52% (±9,63), which show no significant difference of tidal
impedance distribution (p= 0,157). Upper right 7,79% (±6,18) and lower left 10,83% (±7,13)
have a significantly lower tidal impedance compared to the lower right segment with
p<0.0001. These findings are well illustrated in Fig 64, which demonstrates the four segments
of the lungs and their median values.
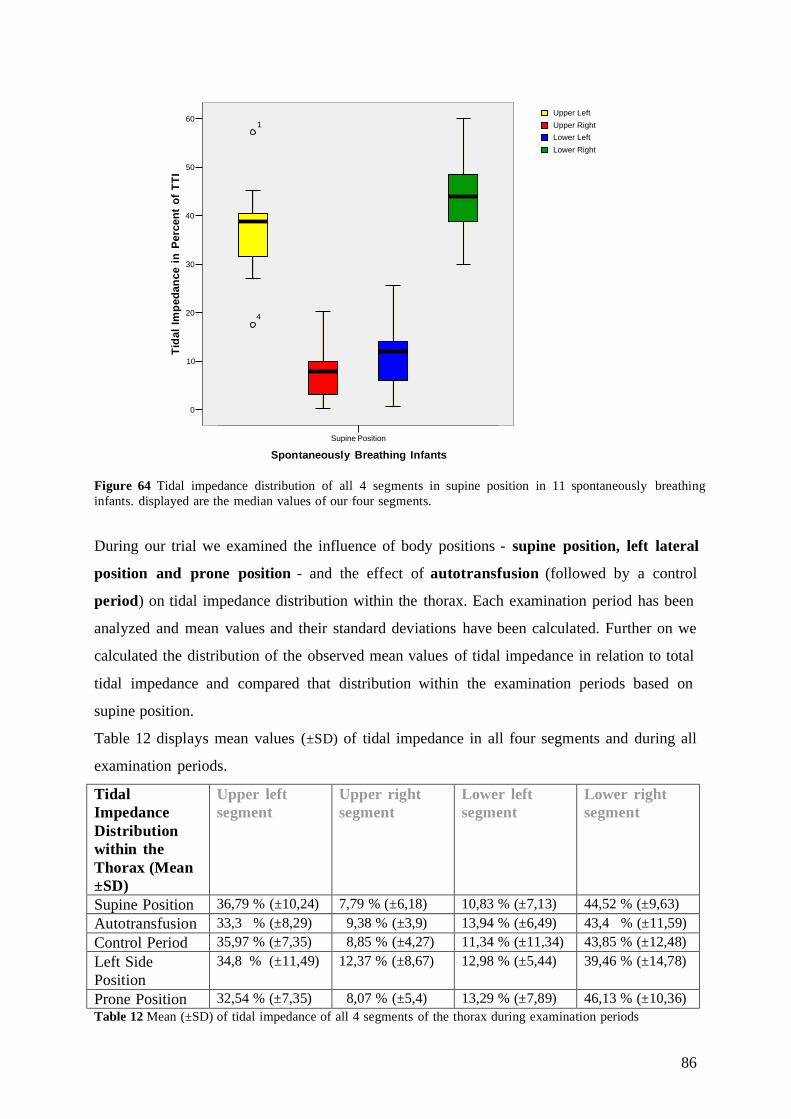
86
Supine Position
Spontaneously Breathing Infants
60
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f TT
I
1
4
Lower RightLower LeftUpper RightUpper Left
Figure 64 Tidal impedance distribution of all 4 segments in supine position in 11 spontaneously breathing infants. displayed are the median values of our four segments.
During our trial we examined the influence of body positions - supine position, left lateral
position and prone position - and the effect of autotransfusion (followed by a control
period) on tidal impedance distribution within the thorax. Each examination period has been
analyzed and mean values and their standard deviations have been calculated. Further on we
calculated the distribution of the observed mean values of tidal impedance in relation to total
tidal impedance and compared that distribution within the examination periods based on
supine position.
Table 12 displays mean values (±SD) of tidal impedance in all four segments and during all
examination periods.
Tidal Impedance Distribution within the Thorax (Mean ±SD)
Upper left segment
Upper right segment
Lower left segment
Lower right segment
Supine Position 36,79 % (±10,24) 7,79 % (±6,18) 10,83 % (±7,13) 44,52 % (±9,63) Autotransfusion 33,3 % (±8,29) 9,38 % (±3,9) 13,94 % (±6,49) 43,4 % (±11,59) Control Period 35,97 % (±7,35) 8,85 % (±4,27) 11,34 % (±11,34) 43,85 % (±12,48) Left Side Position
34,8 % (±11,49) 12,37 % (±8,67) 12,98 % (±5,44) 39,46 % (±14,78)
Prone Position 32,54 % (±7,35) 8,07 % (±5,4) 13,29 % (±7,89) 46,13 % (±10,36) Table 12 Mean (±SD) of tidal impedance of all 4 segments of the thorax during examination periods

87
During all examination periods the highest tidal impedance changes have been detected in the
lower right segment of the thorax, followed by the upper left segment. The upper right
segment and the lower left segment of the thorax show lower tidal impedance changes. As
described in supine position above (Fig 64) the significance of tidal impedance distribution
stayed the same during all examination periods. No significant distribution of tidal impedance
can be detected between the lower right segment and the upper left segment (Autotransfusion
p= 0,114; control period p= 0,210; left side position p= 0,553; prone position p= 0,077)
Tidal impedance distribution of the lower right segment of the thorax was significantly higher
than the tidal distribution of the upper right segment throughout all examination periods
(p<0.0001). Tidal impedance of the lower right segment was significantly higher than the
tidal impedance of the lower left segment of the thorax. (p<0.0001) Table 12 and Fig 65
illustrate the tidal impedance distribution within the thorax.
UR PronePosition
UR Left SidePosition
UR ControlPeriod
URAutotransfusion
Upper Right
70
60
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f TT
I
6
UL PronePosition
UL Left SidePosition
UL ControlPeriod
ULAutotransfusion
Upper Left
70
60
50
40
30
20
10
Tida
l Im
peda
nce
in P
erce
nt o
f TT
I
44
LR PronePosition
LR Left SidePosition
LR ControlPeriod
LRAutotransfusion
Lower Right
70
60
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f TT
I
46
9
LL PronePosition
LL Left SidePosition
LL ControlPeriod
LLAutotransfusion
Lower Left
70
60
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f TT
I
6
113
Figure 65 Tidal impedance changes in all 4 quadrants during all examination periods. Red= upper right segment, yellow= upper left segment, blue= lower left segment, green= lower right segment of the thorax. Examination periods have been performed in the following order: Supine position – Autotransfusion – Control period – Left side position – Prone position. (n=10)

88
Additionally we investigated the significance of tidal distribution changes in the lower right
segment throughout the examination periods. Every examination period has been compared to
the tidal impedance distribution of the lower right segment in supine position. Even we
detected minimal changes in tidal distribution during our examination periods [supine position
(36,79%) - autotransfusion (33,3%) p= 0,463/ SPg - control period (35,97%) p= 460 /SP - left
side position (34,8%) p= 0,244 and SP - prone position (32,54%) p=0,970], tidal impedance
distribution in the lower right thorax was not mainly influenced by body position.
Residual Impedance
In supine position we tested the distribution of residual impedance within our 4 segments.
According to our hypothesis the highest residual impedance changes are found in the upper
right segment of the lungs. A student’s t-test has been performed to test the significance of
residual impedance distribution in all segments referring to the upper right segment.
Residual impedance showed a mean (±SD) in the upper right segment of 32,81% (±8,06) and
in the lower left segment of 29% (±7,58) with a p= 0,86, therefore no significance in residual
impedance distribution could be found between these two segments. On the contrary upper
left segment presents a lower residual impedance with 18,09% (±7,3) and lower right segment
displays a residual impedance of 20,09% (7,62), both with a significant p<0,05. Fig 66
demonstrates these findings as residual impedance changes are significantly higher in the
upper right segment compared to upper left and lower right segment.
g SP= Supine Position

89
Lower RightLower LeftUpper RightUpper Left
60
50
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f Tot
al R
esI
Figure 66 Residual impedance in all segments of the thorax in supine position in spontaneously breathing infants (n=11)
During our trial we examined the influence of body positions - supine position, left lateral
position and prone position - and the effect of autotransfusion (followed by a control
period) on residual impedance distribution within the thorax. Each examination period has
been analyzed and mean values and their standard deviations have been calculated. Further on
we calculated the distribution of the observed mean values of residual impedance in relation
to total residual impedance.
Table 13 illustrates mean (±SD) of residual impedance during all examination periods:
Residual Impedance Distribution within the Thorax (Mean ±SD)
Upper left segment
Upper right segment
Lower left segment
Lower right segment
Supine Position 18,09 % (±7,3) 32,81 % (±8,06) 29 % (±7,58) 20,09 % (±7,62) Autotransfusion 17,2 % (±6,64) 31,8 % (±7,2) 29,8 % (±6,49) 21,2 % (±6,86) Control Period 17,5 % (±6,9) 31,8 % (±6,49) 28,5 % (±7,07) 22,6 % (±6,46) Left Side Position
20 % (±13,8) 29,2 % (±8,67) 27,8 % (±7,7) 21,5 % (±6,81)
Prone Position 17,2 % (±8,18) 31,1 % (±8,02) 29 % (±8,53) 22,5 % (±8,23) Table 13 Mean (±SD) of residual impedance of all 4 segments of the thorax during examination periods
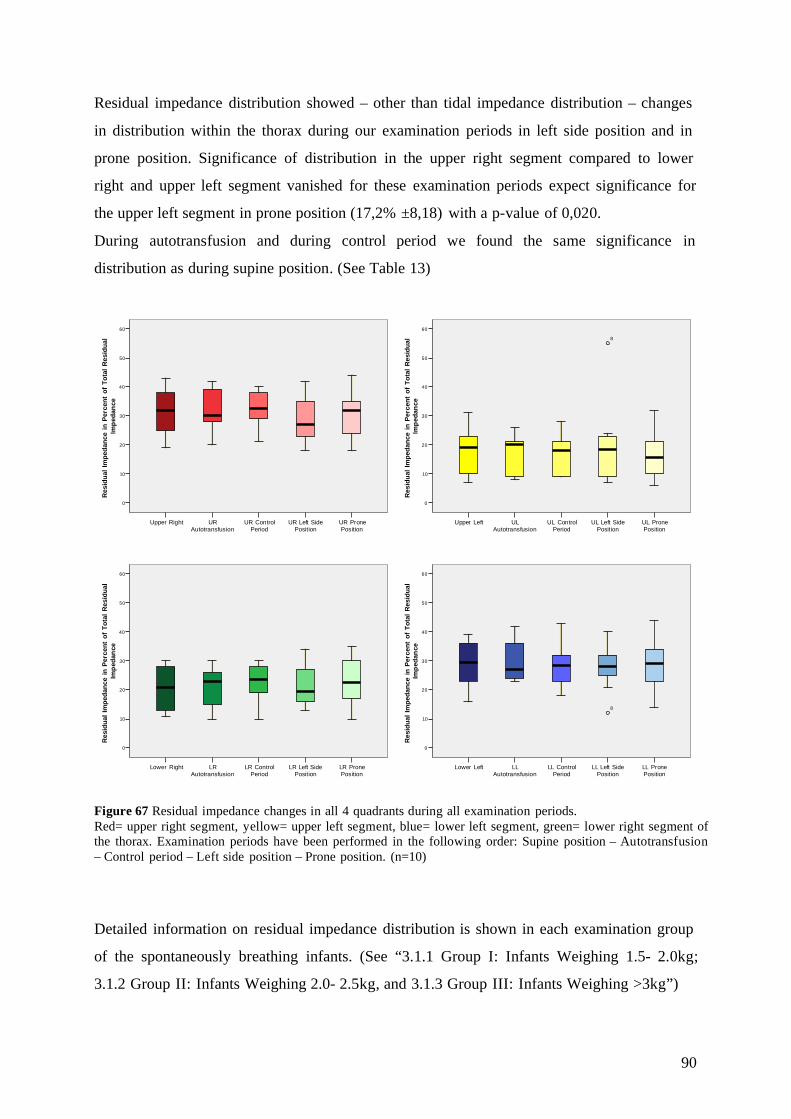
90
Residual impedance distribution showed – other than tidal impedance distribution – changes
in distribution within the thorax during our examination periods in left side position and in
prone position. Significance of distribution in the upper right segment compared to lower
right and upper left segment vanished for these examination periods expect significance for
the upper left segment in prone position (17,2% ±8,18) with a p-value of 0,020.
During autotransfusion and during control period we found the same significance in
distribution as during supine position. (See Table 13)
UR PronePosition
UR Left SidePosition
UR ControlPeriod
URAutotransfusion
Upper Right
60
50
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f To
tal R
esid
ual
Impe
danc
e
UL PronePosition
UL Left SidePosition
UL ControlPeriod
ULAutotransfusion
Upper Left
60
50
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f To
tal R
esid
ual
Impe
danc
e
8
LR PronePosition
LR Left SidePosition
LR ControlPeriod
LRAutotransfusion
Lower Right
60
50
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f To
tal R
esid
ual
Impe
danc
e
LL PronePosition
LL Left SidePosition
LL ControlPeriod
LLAutotransfusion
Lower Left
60
50
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f To
tal R
esid
ual
Impe
danc
e
8
Figure 67 Residual impedance changes in all 4 quadrants during all examination periods. Red= upper right segment, yellow= upper left segment, blue= lower left segment, green= lower right segment of the thorax. Examination periods have been performed in the following order: Supine position – Autotransfusion – Control period – Left side position – Prone position. (n=10)
Detailed information on residual impedance distribution is shown in each examination group
of the spontaneously breathing infants. (See “3.1.1 Group I: Infants Weighing 1.5- 2.0kg;
3.1.2 Group II: Infants Weighing 2.0- 2.5kg, and 3.1.3 Group III: Infants Weighing >3kg”)

91
3.2 Infants with Assisted Ventilation
3.2.1 Infants with SIMV
In this study group we investigated four infants requiring assisted ventilation, one infant with
CPAP therapy and three infants with SIMV during their stay in our NICU. These infants had a
mean (±SD) gestational age of 33,75 (±5,56) weeks and a mean body weight of 2430g (±777)
on the day of examination. Vital parameters and respiratory parameters have been recorded
during every examination period every three minutes and the mean value of these findings in
supine position is displayed as sample below. Vital parameters and respiratory parameter
remained stable. In this group examination periods have been performed in the following
order:
Supine position, PEEP of 4.5 cm H2O
1. Supine position, PEEP decrease of 1 cm H2O to 3.5cm H2O
2. Supine position, PEEP increase of 2 cm H2O to 5.5cm H2O
3. Supine position, PEEP decrease of 1 cm H2O to 4.5 cm H2O
4. Supine position, PEEP consistent at 4.5 cm H 2O during Autotransfusion
5. Supine position, PEEP consistent at 4.5 cm H 2O during Control Period
Parameters of interest and studied by electrical impedance segmentography are tidal
impedance and residual impedance.
Vital parameters of this study group are shown in table 15 (See “Residual Impedance”)
Tidal Impedance
Tidal impedance distribution has been tested in three infants during all examination periods
and in four infants in supine position. We stated that we expect the highest tidal impedance
changes in the lower right segment compared to the remaining three segments of the thorax.
On contrary to the spontaneously breathing infants group we did not find a significant
difference (p<0,05) in tidal impedance distribution in infants receiving assisted ventilation.
The only significance in tidal impedance distribution we could detect in infants with assisted
ventilation was during autrotransfusion when a significant difference in tidal impedance was

92
observed between the lower right segment with 44,67% (±5,54) and the lower left segment
with 11,33% (±11,15) resulting in p=0,047. During assisted ventilation tidal impedance seems
to be more equally distributed than during spontaneous breaths.
Fig 68 displays tidal impedance of all four segments of the thorax in supine position at
PEEP 4.5cm H2O.
Lower RightLower LeftUpper RightUpper Left
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f Tot
al T
idal
Impe
danc
e
Figure 68 Tidal impedance in four segments of the thorax in infants with assisted ventilation at a PEEP of 4.5cm H2O in supine position. (n=4) We studied the effect of alternation of PEEP level (decrease of PEEP 1cm H2O followed by
increase of PEEP 2cm H2O) on tidal impedance and its distribution. This manoeuvre affected
tidal impedance in each of the three infants with assisted ventilation differently; therefore
these infants have been analyzed in detail below. (See “Infant I 2100g”, “Infant II 2910g”,
and “Infant III 3210g”). The different effect of PEEP level alternation on infants is as well
demonstrated in Fig 69. In one infant a clear fall in tidal impedance in the upper left segment
of the thorax occurred through the decrease of PEEP and remained low through all
examination periods. (See “Infant 2910g”)

93
UR PEEP 4.5 CPUR PEEP 4.5 ATUR PEEP 4.5UR PEEP 5.5UR PEEP 3.5Upper Right
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f Tot
al T
idal
Impe
danc
e
UL PEEP 4.5 CPUL PEEP 4.5 ATUL PEEP 4.5UL PEEP 5.5UL PEEP 3.5Upper Left
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f Tot
al T
idal
Impe
danc
e
LR PEEP 4.5 CPLR PEEP 4.5 ATLR PEEP 4.5LR PEEP 5.5LR PEEP 3.5Lower Right
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f Tot
al T
idal
Impe
danc
e
LL PEEP 4.5 CPLL PEEP 4.5 ATLL PEEP 4.5LL PEEP 5.5LL PEEP 3.5Lower Left
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f Tot
al T
idal
Impe
danc
e
Figure 69 Tidal impedance distribution in four segments of the thorax in infants with assisted ventilation during examination periods. (n=3) Table 14 shows tidal impedance distribution during examination periods in four segments of
the thorax. After the alternation of PEEP to 3.5cm H2O tidal impedance distribution remained
the same and was not affected by later PEEP increase of 2 cm H2O nor autotransfusion.
Tidal Impedance
[Mean ±SD]
Upper left
segment
Upper right
segment
Lower left
segment
Lower right
segment
PEEP 4.5cm H2O 31,7 % (±9,53)* 22,75 % (±5,67)* 17,75 % (±7,54)* 27,75 % (±6,34)*
PEEP 3.5cm H2O 31 % (±25,15) 17,33 % (±15,04) 11,33 % (±11,93) 40,67 % (±9,5)
PEEP 5.5cm H2O 31,33% (±25,48) 16,67 % (±15,17) 11,33 % (±11,15) 40,67 % (±9,5)
PEEP 4.5cm H2O 29,33% (±23,67) 16,33 % (±14,04) 12 % (±11,35) 42,67 % (±7,5)
PEEP 4.5cm H2O Autotransfusion
28,33% (±22,94) 15,67 % (±13,01) 11,33 % (±11,15) 44,67 % (±5,5)
PEEP 4.5cm H2O Control Period
28,33% (±23,07) 16,67 % (±15,56) 12 % (±11,35) 42,67 % (±5,5)
Table 14 Tidal impedance in infants with assisted ventilation during examination periods, mean (±SD), (*n=4 in supine position, PEEP 4.5cm H2O, n=3 during all other examination periods)

94
Residual Impedance
Residual impedance has been tested in three infants during all examination periods and in four
infants in supine position. On contrary to the spontaneously breathing infants group we did
not find a significant difference (p<0,05) in residual impedance distribution in infants
receiving assisted ventilation.
Upper left segment showed a residual impedance with a mean (±SD) of 26,16% (±9,09),
upper right segment result in 28% (±4,23), lower left segment displayed 27,21% (±6,36) and
only lower right segment was slightly lower with 18,61% (±7,37).
Fig 70 demonstrates residual impedance distribution in all four segments of the thorax during
assisted ventilation with PEEP of 4.5cm H2O in supine position.
Lower RightLower LeftUpper RightUpper Left
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f Res
I
Figure 70 Residual impedance distribution in 4 infants requiring assisted ventilation and a mean body weight of 2430g.
Vital parameters and respiratory parameters have been recorded and represent following
results for these four infants given in table 15. Vital parameters remained stable throughout all
examination periods.

95
Parameter N Mean Std. Deviation
Blood pressureh 4 46,05 8,33
Breathing Frequency (=Breaths per Minute)
4 49 24,93
Saturation of Oxygeni 4 95,25 4,5
Tidal Volume (ml) 3 17,8 5,24
Heart Rate (=Beats per Minute)
4 129,75 33,63
Table 15 Vital parameters and respiratory parameters in 4 infants with assisted ventilation at a PEEP of 4.5cm H2O in supine position. According to our protocol we decreased PEEP to 3.5cm H2O in the three infants receiving
SIMV as we further on studied the effect of PEEP decrease and increase on residual
impedance distribution. Fig 71 visualizes and table 16 illustrates residual impedance in all
four segments of the thorax during examination periods.
h Mean arterial pressure has been calculated by monitoring systolic and diastolic blood pressure. MAP= Diastolic Pressure + 1/3(Systolic Pressure – Diastolic Pressure) i On room air

96
UR PEEP4.5 CP
UR PEEP4.5 AT
UR PEEP4.5
UR PEEP5.5
UR PEEP3.5
Upper Right
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f To
tal R
esI
UL PEEP 4.5AT
UL PEEP 4.5UL PEEP 5.5UL PEEP 3.5Upper Left
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f R
esI
LR PEEP 4.5CP
LR PEEP 4.5AT
LR PEEP 4.5LR PEEP 5.5LR PEEP 3.5Lower Right
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f To
tal R
esI
LL PEEP 4.5CP
LL PEEP 4.5AT
LL PEEP 4.5LL PEEP 5.5LL PEEP 3.5Lower Left
40
30
20
10
0
Res
idua
l Im
peda
nce
in P
erce
nt o
f To
tal R
esI
Figure 71 Residual impedance distribution in all four segments of the thorax during examination periods. Red= upper right segment, yellow= upper left segment, green= lower right segment and blue= lower left segment of the thorax. Examination periods have been performed and are presented in the given order: 1.)Supine position PEEP 4.5cm H2O, 2.) SPj PEEP 3.5cm H2O, 3.) SP PEEP 5.5cm H2O, 4.) SP PEEP 4.5cm H2O, 5.) SP PEEP 4.5cm H2O during autotransfusion and 6.) SP PEEP 4.5cm H2O during control period. UL= upper left segment of the thorax, UR= upper right segment, LL= lower left segment and LR= lower right segment.
Residual impedance distribution remained stable throughout all examination periods and the
change of PEEP level did not influence residual impedance distribution within the thorax.
(See “Table 16”)
j SP= Supine position

97
Residual
Impedance
[Mean ±SD]
Upper left
segment
Upper right
segment
Lower left
segment
Lower right
segment
PEEP 4.5cm H2O 26,16 % (±9,09)* 28 % (±4,23)* 27,21 % (±6,36)* 18,61 % (±7,37)*
PEEP 3.5cm H2O 24,48 % (±9,73) 29,27 % (±3,59) 29,44 % (±5,73) 16,79 % (±7,87)
PEEP 5.5cm H2O 23,97 % (±9,96) 29,06 % (±3,53) 29,47 % (±5,75) 17,49 % (±8,36)
PEEP 4.5cm H2O 23,44 % (±10,18) 28,88 % (±3,57) 30,17 % (±6,6) 17,15 % (±8,29)
PEEP 4.5cm H2O Autotransfusion
24,07 % (±10,63) 28,75 % (±3,69) 30,07 % (±6,57) 17,1 % (±8,38)
PEEP 4.5cm H2O Control Period
23,72 % (±10,58) 28,75 % (±3,69) 30,07 % (±6,57) 17,1 % (±8,38)
Table 16 Residual impedance in infants with assisted ventilation during examination periods, mean (±SD),*n=4 in supine position at PEEP 4.5cm H2O, n=3 during all other examination periods.
We investigated only three infants on SIMV and one infant receiving CPAP during this pilot
trial, therefore each infant has been studied more closely (see below) and not just similarities
in between the infants have been of interest but details of each single infant have been studied.
Residual impedance distribution varied in between the infants – as displayed in Fig 72 – and
the underlying cause for ventilation in these infants never was the same. Even there were
difference in residual impedance distribution within the infants; their single distribution of
residual impedance within the thorax remained stable as shown in fig 71 and table 16.
3500,003000,002500,002000,001500,00
Body Weight (g)
40,00
30,00
20,00
10,00
Res
idua
l Im
peda
nce
in P
erce
nt o
f To
tal R
esI
Lower RightBody Weight (g)
Lower LeftBody Weight (g)
Upper RightBody Weight (g)
Upper LeftBody Weight (g)
Figure 72 Residual impedance distribution in 4 segments of the thorax in infants with assisted ventilation based on body weight (n=4)

98
Infant I – 2100g
We examined one male infant born at 28 weeks of gestational age. At the day of examination
the boy was 2 months old (corrected age 36 weeks) with a current body weight of 2100g. The
infant has been admitted to the NICU because of prematurity and has been ventilated (SIMV,
PEEP 4.5cm H2O) after a shunt operation due to a hydrocephalus. This infant did not show
any respiratory disease.
The infant was stable on the day of examination and during our examination periods. The
following vital signs have been noticed and remained constant during our examination course
(See “2.4.6 Course of Examination”):
Heart rate 157, breathing frequency 77, SaO2 89%, tidal volume 13 and blood pressure 82/59.
We observed the infant’s tidal impedance changes as well as residual impedance changes
during our examination periods and additionally monitored the infant during extubation of
this infant.
Tidal impedance changes showed a few changes during our examination periods which are
of interest, but mostly tidal impedance stayed the same:
During a PEEP level of 5.5cm H2O, tidal impedance changes were lowest with a total tidal
impedance of 87,17, the lowest tidal impedance changes we could find during the whole
examination course. Interestingly tidal impedance decreased in the beginning of our
examination in the upper left segment from 27,56 (PEEP 4.5cm H2O) to 1,68 (PEEP 3.5cm
H2O) and remained very low during the further examination course on the ventilator.
Most impressive tidal impedance changes have been detected during extubation of the infant
followed by spontaneous breathing of the infant. Immediately after extubation total tidal
impedance changes increased from 108,19 during PEEP 4.5cm H2O to 257,56 after extubation
breathing spontaneously which is an increase of 138% of total tidal impedance. Highest
changes in regional tidal impedance during extubation have been detected in the upper left
segment, in which tidal impedance increased from 10 (PEEP 4.5cm H2O) to 62,54 (breathing
spontaneously). All other segments showed as well a clear increase of regional tidal
impedance after extubation, tidal impedance changes of the lower right segment increased
from 42,88 during PEEP 4.5 cm H2O to a tidal impedance of 100 after extubation. If tidal
impedance distribution is observed before and after extubation, it radically changed through
that manoeuvre in all four segments.

99
During PEEP 4.5 cm H2O regional tidal impedance changes followed this order starting with
the highest (and remained like this through all examination periods on SIMV): LRk – URl –
LLm – ULn. Extubation changed this order to:
LRk-ULn-LLm-URl. Exactly this order of tidal impedance distribution has been described in
our spontaneously breathing infants group
Residual impedance changes have been monitored through all examination periods in this
infant as well as during extubation of this infant. Visualized in fig 73 and tabulated in table 17
residual impedance decreased slightly but constantly during our examination periods when
PEEP levels where changed. The fall of residual impedance in all four segments was not
depending on neiter increase of PEEP or decrease of PEEP. The fall in residual impedance
interestingly remained when it stayed at PEEP 4.5cm H2O for a longer while during our
autotransfusion manoeuvre followed by a control period. Further on a significant fall of
residual impedance in all four segments has been observed during nursing procedures of the
infant while tidal impedance increased at the same time.
More clearly a decrease of residual impedance is detected after extubation during
spontaneously breathing of the infant and displayed in fig 73 and table 17. The decrease in
residual impedance is very impressive in the upper left segment and a fall from 7720 to 4430
is shown, which is a decrease in residual impedance of 74%. While the total residual
impedance decreased as well, a slight increase of residual impedance in the upper right and
lower left segment of the thorax has been recorded. Residual impedance of the lower right
segment of the thorax mainly stayed the same.
k LR= Lower right segment of the thorax l UR= Upper right segment of the thorax m LL= Lower left segment of the thorax n UL=Upper left segment of the thorax
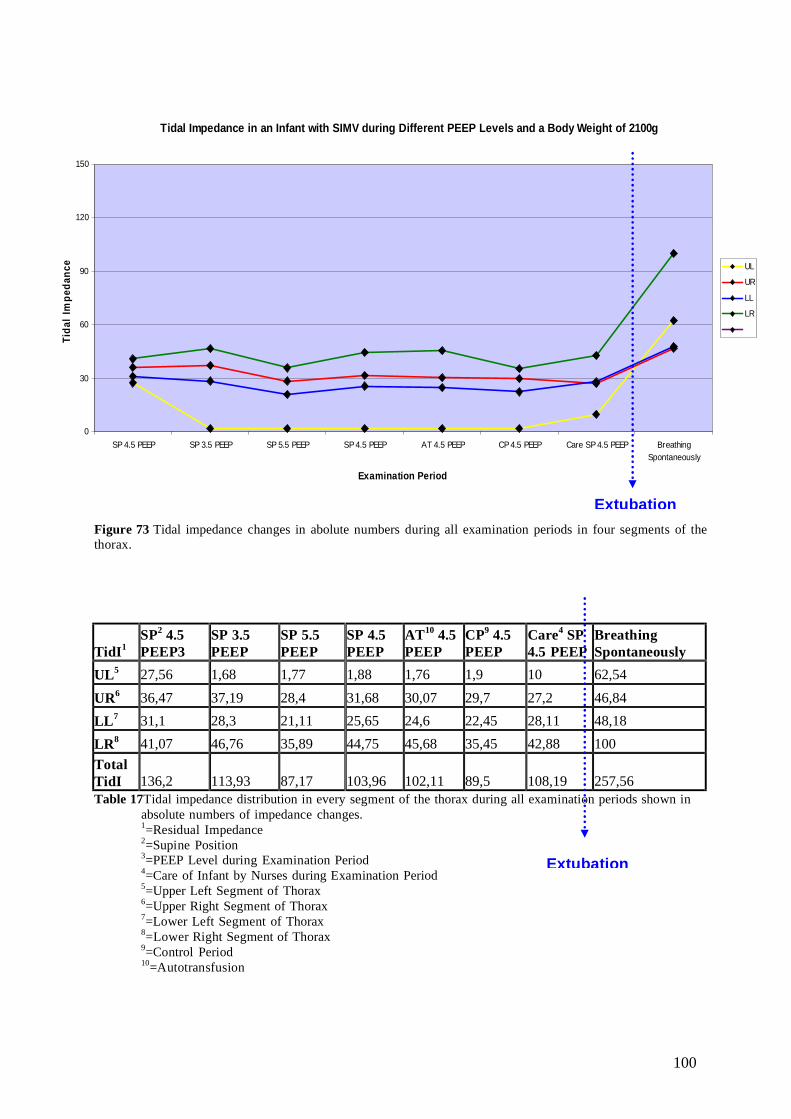
100
Figure 73 Tidal impedance changes in abolute numbers during all examination periods in four segments of the thorax.
TidI1 SP2 4.5 PEEP3
SP 3.5 PEEP
SP 5.5 PEEP
SP 4.5 PEEP
AT10 4.5 PEEP
CP9 4.5 PEEP
Care4 SP 4.5 PEEP
Breathing Spontaneously
UL5 27,56 1,68 1,77 1,88 1,76 1,9 10 62,54
UR6 36,47 37,19 28,4 31,68 30,07 29,7 27,2 46,84 LL7 31,1 28,3 21,11 25,65 24,6 22,45 28,11 48,18 LR8 41,07 46,76 35,89 44,75 45,68 35,45 42,88 100 Total TidI 136,2 113,93 87,17 103,96 102,11 89,5 108,19 257,56 Table 17Tidal impedance distribution in every segment of the thorax during all examination periods shown in absolute numbers of impedance changes. 1=Residual Impedance 2=Supine Position 3=PEEP Level during Examination Period 4=Care of Infant by Nurses during Examination Period 5=Upper Left Segment of Thorax 6=Upper Right Segment of Thorax 7=Lower Left Segment of Thorax 8=Lower Right Segment of Thorax 9=Control Period 10=Autotransfusion
Tidal Impedance in an Infant with SIMV during Different PEEP Levels and a Body Weight of 2100g
0
30
60
90
120
150
SP 4.5 PEEP SP 3.5 PEEP SP 5.5 PEEP SP 4.5 PEEP AT 4.5 PEEP CP 4.5 PEEP Care SP 4.5 PEEP BreathingSpontaneously
Examination Period
Tida
l Im
peda
nce UL
UR
LL
LR
Extubation
Extubation
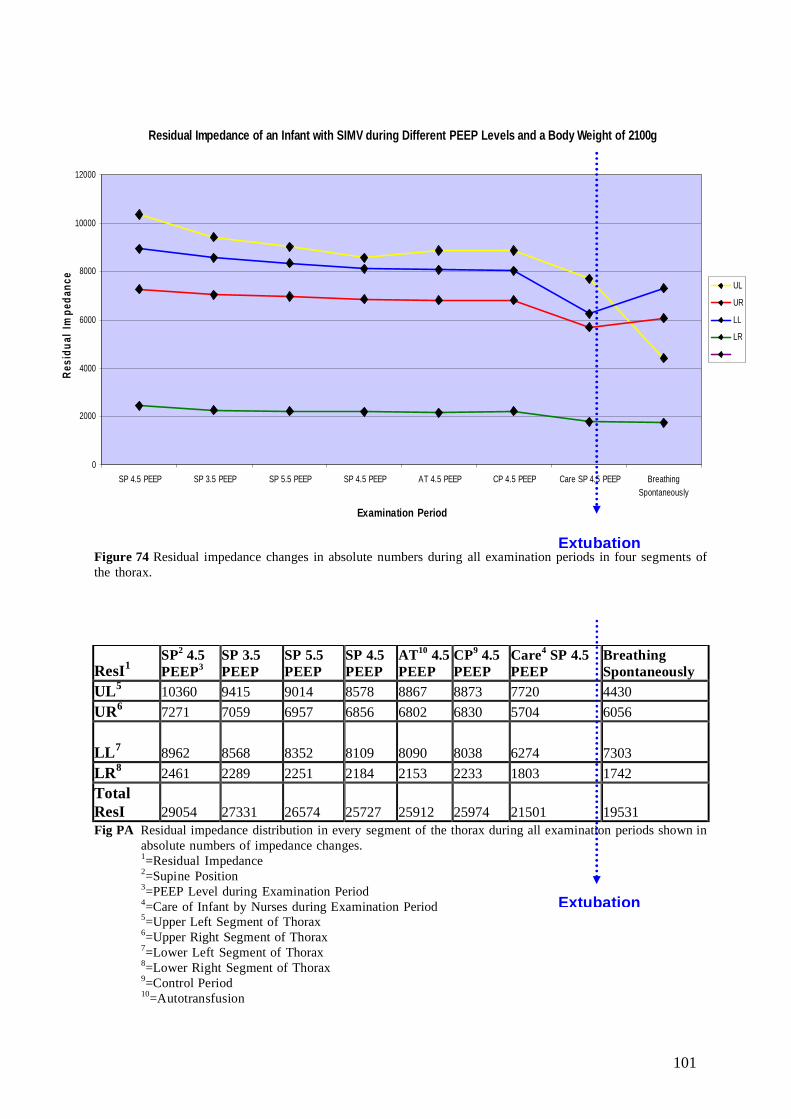
101
Figure 74 Residual impedance changes in absolute numbers during all examination periods in four segments of the thorax.
Fig PA Residual impedance distribution in every segment of the thorax during all examination periods shown in absolute numbers of impedance changes. 1=Residual Impedance 2=Supine Position 3=PEEP Level during Examination Period 4=Care of Infant by Nurses during Examination Period 5=Upper Left Segment of Thorax 6=Upper Right Segment of Thorax 7=Lower Left Segment of Thorax 8=Lower Right Segment of Thorax 9=Control Period 10=Autotransfusion
ResI1 SP2 4.5 PEEP3
SP 3.5 PEEP
SP 5.5 PEEP
SP 4.5 PEEP
AT10 4.5 PEEP
CP9 4.5 PEEP
Care4 SP 4.5 PEEP
Breathing Spontaneously
UL5 10360 9415 9014 8578 8867 8873 7720 4430 UR6 7271 7059 6957 6856 6802 6830 5704 6056
LL7 8962 8568 8352 8109 8090 8038 6274 7303 LR8 2461 2289 2251 2184 2153 2233 1803 1742 Total ResI 29054 27331 26574 25727 25912 25974 21501 19531
Residual Impedance of an Infant with SIMV during Different PEEP Levels and a Body Weight of 2100g
0
2000
4000
6000
8000
10000
12000
SP 4.5 PEEP SP 3.5 PEEP SP 5.5 PEEP SP 4.5 PEEP AT 4.5 PEEP CP 4.5 PEEP Care SP 4.5 PEEP BreathingSpontaneously
Examination Period
Resi
dual
Impe
danc
e
UL
UR
LL
LR
Extubation
Extubation

102
Infant II - 2910g
The second infant we investigated on SIMV and a PEEP of 4.5cm H2O at the start of our
examination has been admitted to the NICU presenting with a mild pneumothorax of the left
lung. This male infant was born at 38 weeks of gestational age and presented with a current
body weight of 2910g on the day of examination which was the fifth day of life of this infant.
The newborn remained stable during our examination course. Vital signs were observed and
stayed constant during our examination course:
Heart rate 149, breathing frequency 56, saturation of oxygen 95%, tidal volume 17, and blood
pressure 67/36.
As already described in all other infants, tidal impedance changes and residual impedance
changes have been of major interest. PEEP level have been changed in this infant and the
effect of autotransfusion followed by a control period has been studied and additionally
suction has been performed by the nursing staff twice during our examination course. The
effect of hiccups on our measurements has been observed in this infant.
Tidal impedance changes have been recorded throughout all examination periods. Shortly
after we started our measurements, the infant had bad and continuous hiccups, which
obviously lead to an immediate increase of tidal impedance changes in the lower left segment
of the thorax. The other three segments as well showed an increase in tidal impedance
changes but a less impressive one. Further on we decreased PEEP to 3.5cm H2O which lead to
a clear fall in tidal impedance in all four segments and they did not increase anymore
throughout the rest of the examination course unrelated to the manoeuvre we have performed.
The first suction at a PEEP of 5.5cm H2O increased tidal impedance but just a little in all four
segments. The newborn needed a second suction during our measurements when the PEEP
level was set back to 4.5cm H2O, here only the upper segments showed an increase in tidal
impedance changes after suction has been performed.
After the fall of tidal impedance during PEEP was set to 3.5cm H2O, tidal impedance changes
in every segment of the thorax remained stable.

103
Residual impedance changes were monitored during all examination periods. Other than
tidal impedance, residual impedance was not influenced by the infant’s continuous hiccups at
the beginning of our examination course.
The first suction only increased residual impedance of the upper right and lower left segment,
those which primarily showed the higher residual impedance anyway. Lower right and upper
left residual impedance further on felt during the first suction. During our second suction
manoeuvre residual impedance in all four segments increased.
PEEP increase and PEEP decrease manoeuvres during our examination periods did not
mainly influence our observation in stable residual impedance values as only changes of a
total of 2cm H2O could be performed in infants receiving assisted ventilation in our NICU.
Fig 76 displays and table 19 demonstrates these findings.

104
Figure 75 Tidal impedance changes in absolute (measured) numbers during all examination periods in four segments of the thorax.
TidI1 SP2 4.5 PEEP3
SP 4.5 PEEP Hiccup
SP 3.5 PEEP
SP 5.5 PEEP
SP 5.5 PEEP Suction
SP 4.5 PEEP
SP 4.5 PEEP Suction
AT9 4.5 PEEP
CP8 4.5 PEEP
UL4 84 96,55 26,07 26,97 28,8 24,58 24,7 25,98 28,5
UR5 54,78 59,15 1,92 1,91 1,94 1,57 1,85 1,56 1,49
LL6 45,52 102,76 1,72 1,74 1,79 2,23 1,97 1,7 2,42
LR7 64,94 78,82 29,3 26,04 31,6 29,16 28,38 29,14 31,06
Total TidI 249,24 337,28 59,01 56,66 64,13 57,54 56,9 58,38 63,47 Table 18 Tabulated tidal impedance changes in absolute (measured) numbers during all examination periods in four segments of the thorax. 1=Residual Impedance 2=Supine Position 3=PEEP Level during Examination Period 4=Upper Left Segment of Thorax 5=Upper Right Segment of Thorax 6=Lower Left Segment of Thorax 7=Lower Right Segment of Thorax 8=Control Period 9=Autotransfusion
Tidal Impedance in an Infant during Different PEEP Levels and a Body Weight of 2910g
0
20
40
60
80
100
120
SP 4.5 PEEP SP 4.5 PEEPHickup
SP 3.5 PEEP SP 5.5 PEEP SP 5.5 PEEPSuction
SP 4.5 PEEP SP 4.5 PEEPSuction
AT 4.5 PEEP CP 4.5 PEEP
Examination Period
Tida
l Im
peda
nce UL
UR
LL
LR

105
Figure 76 Residual impedance changes in absolute (measured) numbers during all examination periods in four segments of the thorax.
ResI1 SP2 4.5 PEEP3
SP 4.5 PEEP Hiccup
SP 3.5 PEEP
SP 5.5 PEEP
SP 5.5 PEEP Suction
SP 4.5 PEEP
SP 4.5 PEEP Suction
AT9 4.5 PEEP
CP8 4.5 PEEP
UL4 4162 4138 4049 3849 3509 3664 3791 3782 3856
UR5 9668 9680 9493 9285 9536 9347 9503 9442 9510
LL6 9933 9932 9794 9716 10118 10098 10310 10235 10311
LR7 5418 5392 5278 5326 5202 5245 5310 5340 5348
Total ResI 29181 29142 28614 28176 28365 28354 28914 28799 29025 Table 19 Tabulated residual impedance changes in absolute (measured) numbers during all examination periods in four segments of the thorax. 1=Residual Impedance 2=Supine Position 3=PEEP Level during Examination Period 4=Upper Left Segment of Thorax 5=Upper Right Segment of Thorax 6=Lower Left Segment of Thorax 7=Lower Right Segment of Thorax 8=Control Period 9=Autotransfusion
Residual Impedance in an Infant at Different PEEP Levels and a Body Weight of 2910g
0
2000
4000
6000
8000
10000
12000
SP 4.5 PEEP SP 4.5 PEEPHickup
SP 3.5 PEEP SP 5.5 PEEP SP 5.5 PEEPSuction
SP 4.5 PEEP SP 4.5 PEEPSuction
AT 4.5 PEEP CP 4.5 PEEP
Examination Period
Resi
dual
Impe
danc
e
UL
UR
LL
LR
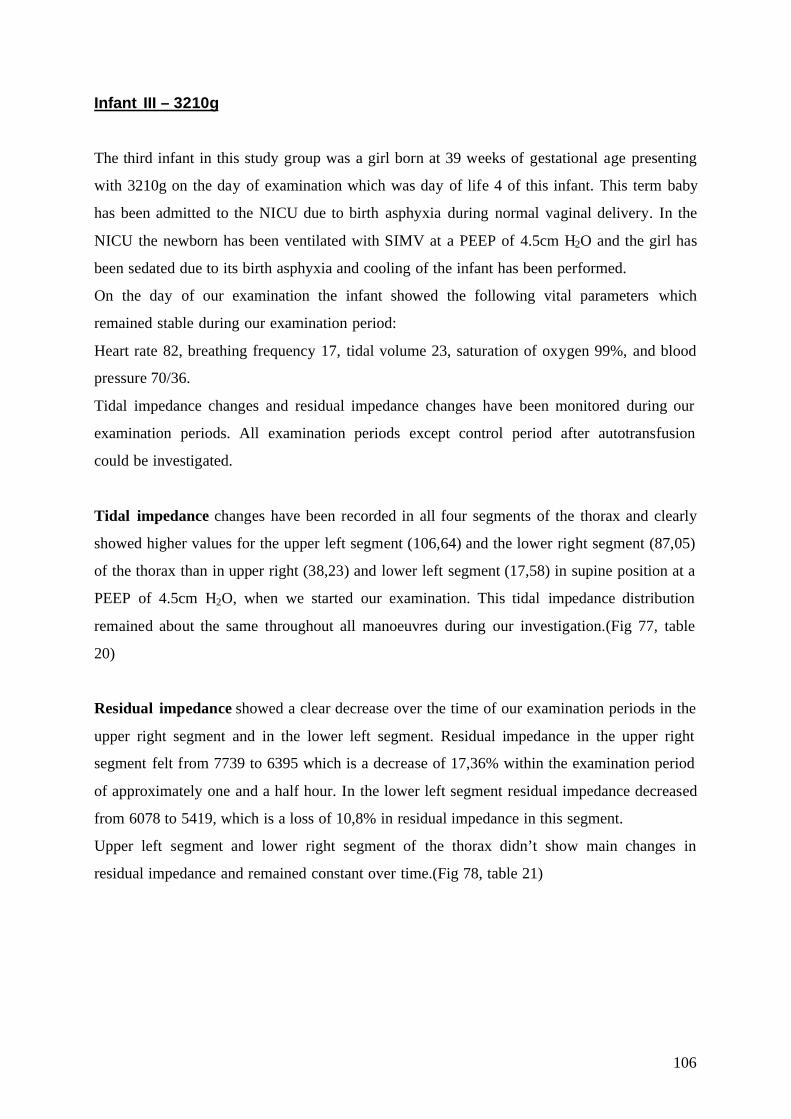
106
Infant III – 3210g The third infant in this study group was a girl born at 39 weeks of gestational age presenting
with 3210g on the day of examination which was day of life 4 of this infant. This term baby
has been admitted to the NICU due to birth asphyxia during normal vaginal delivery. In the
NICU the newborn has been ventilated with SIMV at a PEEP of 4.5cm H2O and the girl has
been sedated due to its birth asphyxia and cooling of the infant has been performed.
On the day of our examination the infant showed the following vital parameters which
remained stable during our examination period:
Heart rate 82, breathing frequency 17, tidal volume 23, saturation of oxygen 99%, and blood
pressure 70/36.
Tidal impedance changes and residual impedance changes have been monitored during our
examination periods. All examination periods except control period after autotransfusion
could be investigated.
Tidal impedance changes have been recorded in all four segments of the thorax and clearly
showed higher values for the upper left segment (106,64) and the lower right segment (87,05)
of the thorax than in upper right (38,23) and lower left segment (17,58) in supine position at a
PEEP of 4.5cm H2O, when we started our examination. This tidal impedance distribution
remained about the same throughout all manoeuvres during our investigation.(Fig 77, table
20)
Residual impedance showed a clear decrease over the time of our examination periods in the
upper right segment and in the lower left segment. Residual impedance in the upper right
segment felt from 7739 to 6395 which is a decrease of 17,36% within the examination period
of approximately one and a half hour. In the lower left segment residual impedance decreased
from 6078 to 5419, which is a loss of 10,8% in residual impedance in this segment.
Upper left segment and lower right segment of the thorax didn’t show main changes in
residual impedance and remained constant over time.(Fig 78, table 21)

107
Figure 77 Tidal impedance changes in absolute (measured) numbers during all examination periods in four segments of the thorax.
TidI1 SP2 4.5 PEEP3 SP 3.5 PEEP SP 5.5 PEEP SP 4.5 PEEP AT9 4.5 PEEP
UL4 106,64 112,44 104,94 83,1 81,78
UR5 38,23 35,72 35,27 28,91 31,87
LL6 17,58 15,05 16,05 13,89 14,92
LR7 87,05 74 84,38 69,6 82,7
Total TidI 249,5 237,21 240,64 195,5 211,27 Table 20 Tabulated tidal impedance changes in absolute (measured) numbers during all examination periods in four segments of the thorax. 1=Residual Impedance 2=Supine Position 3=PEEP Level during Examination Period 4=Upper Left Segment of Thorax 5=Upper Right Segment of Thorax 6=Lower Left Segment of Thorax 7=Lower Right Segment of Thorax 8=Control Period 9=Autotransfusion
Tidal Impedance in an Infant during Different PEEP Levels and a Body Weight of 3210g
0
20
40
60
80
100
120
SP 4.5 PEEP SP 3.5 PEEP SP 5.5 PEEP SP 4.5 PEEP AT 4.5 PEEP CP 4.5 PEEP
Examination Period
Tida
l Im
peda
nce UL
UR
LL
LR
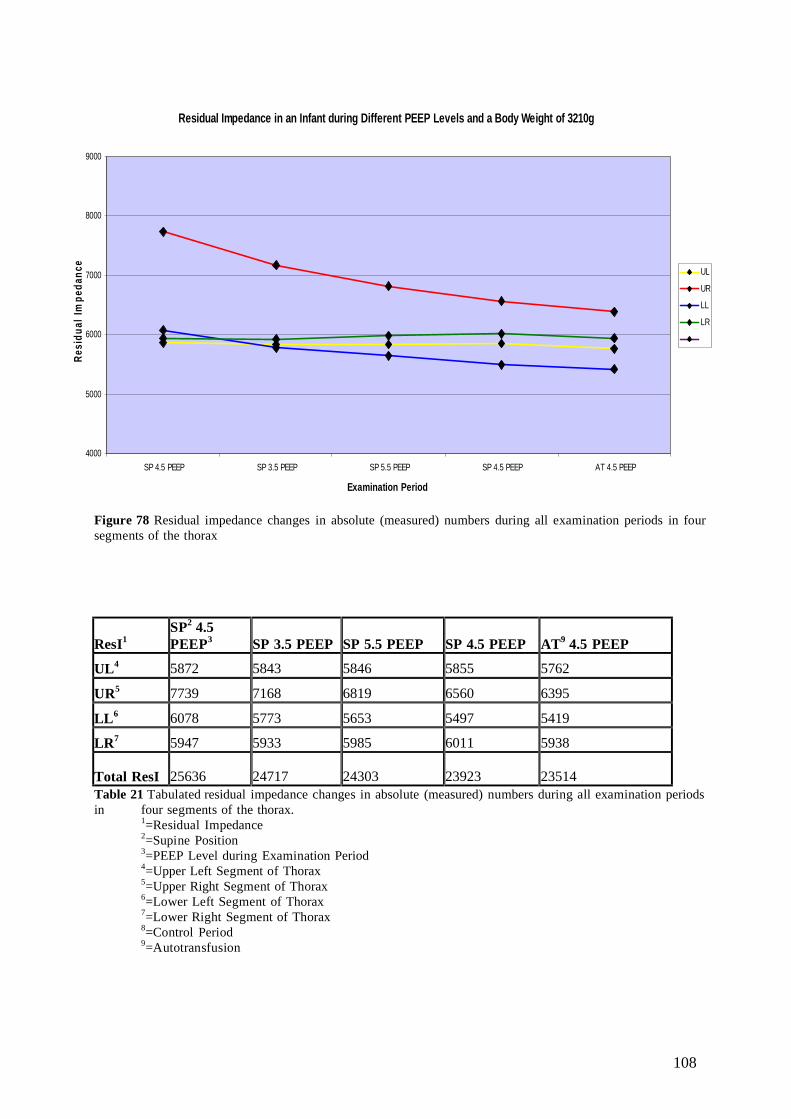
108
Figure 78 Residual impedance changes in absolute (measured) numbers during all examination periods in four segments of the thorax
ResI1 SP2 4.5 PEEP3 SP 3.5 PEEP SP 5.5 PEEP SP 4.5 PEEP AT9 4.5 PEEP
UL4 5872 5843 5846 5855 5762
UR5 7739 7168 6819 6560 6395
LL6 6078 5773 5653 5497 5419
LR7 5947 5933 5985 6011 5938
Total ResI 25636 24717 24303 23923 23514 Table 21 Tabulated residual impedance changes in absolute (measured) numbers during all examination periods in four segments of the thorax. 1=Residual Impedance 2=Supine Position 3=PEEP Level during Examination Period 4=Upper Left Segment of Thorax 5=Upper Right Segment of Thorax 6=Lower Left Segment of Thorax 7=Lower Right Segment of Thorax 8=Control Period 9=Autotransfusion
Residual Impedance in an Infant during Different PEEP Levels and a Body Weight of 3210g
4000
5000
6000
7000
8000
9000
SP 4.5 PEEP SP 3.5 PEEP SP 5.5 PEEP SP 4.5 PEEP AT 4.5 PEEP
Examination Period
Resi
dual
Impe
danc
e
UL
UR
LL
LR

109
3.2.2 The Infant with CPAP During our investigations we examined one infant with a current body weight of 1500g
requiring CPAP (Dräger ®, Babylog 8000) at 4.5cm H2O. This infant has been admitted to
the NICU presenting with prematurity at 30 weeks of gestational age and respiratory distress
syndrome after c-section due to maternal preeclampsia. On the day of examination the infant
was stable, on CPAP and presented with a heart rate of 135 (±11), respiratory rate 56 (±14),
stable blood pressure of 72/38, and a saturation of oxygen of 96% (±1.7).
We examined the infant on CPAP in supine position, during “autotransfusion” and control
period, on its left side, and in prone position as well as during “kangaroo care” with the
mother (=prone position) during an interval without CPAP breathing spontaneously.
(Fig 79)
Figure 79 Decrease of resI in all 4 segments of the thorax during disconnection of CPAP followed by a period of spontaneous breaths in a 1.5kg infant
End of CPAP
Upper right segment
Lower right segment
Upper left segment
Lower left segment

110
Residual Impedance
We observed resI changes with the following order in all 4 segments of the thorax during all
examination periods (supine position, autotransfusion, control period, left side, and prone
position and during “kangaroo care” in prone position) starting with the highest:
Upper left segment – lower right segment – upper right segment – lower left segment.
The shift of body positions during our examinations influenced the regional residual
impedance as well as the total residual impedance, but the descending order of upper left –
lower right – upper right – lower left was consistent throughout all 6 examination periods.
(See Fig 80-81, table 22).
The change of body positions either increased or decreased the impedance signal. To better
compare regional impedance changes of the 4 segments of the thorax total residual impedance
of each examination period was set 100% and detected regional residual impedance changes
which were calculated in percent of total residual impedance. This describes even more
precisely the distribution of residual impedance within the 4 segments following the same
order. Upper left impedance changes vary a total of 5%; all other segments (upper right, lower
left, and lower right) showed deviations of 2% in distribution within the segments.
The upper left segment of the thorax has the highest residual impedance throughout all
examination periods, followed by lower right segment, upper right segment and lower left
segment.
Total residual impedance changes in descending order during our examination of the infant on
CPAP were the following: Prone position – Supine position – Left side – Control period –
Autotransfusion – Spontaneous breathing in prone position.
Most impressive is the decrease of 30% of the initial total residual impedance during a
subsequent spontaneous breathing period in prone position. The residual impedance in the
upper left segment decreases extremely during the spontaneous breathing period, less obvious
but the residual impedance decreases in upper right, lower right, and lower left to the same
extent. The total residual impedance decreases 30% of the initial residual impedance; the
impedance distribution within the 4 segments is constant even during the high decrease of
30% at the end of examination.

111
Examination Course of all 4 Segments of the Thorax
4000
5000
6000
7000
8000
9000
10000
11000
12000
13000
SP AT CP LS PP CPAP disc. PP
Examination Period
Res
idua
l Im
peda
nce
ULURLLLR
Figure 80 Examination course of all 4 segments of the thorax during our investigation. SP= Supine position,AT= Autotransfusion, CP= Control period, LS= Left side, PP= Prone position, CPAP disc. PP= After disconnection of CPAP, examination in prone position, UL= Upper left segment of the thorax, UR= Upper right, segment of the thorax, LL= Lower left segment of the thorax, and LR= Lower right segment of the thorax.
Examination Course in Percent of Total Residual Impedance
15
20
25
30
35
40
SP AT CP LS PP CPAP disc. PP
Examination Period
Perc
ent o
f Tot
al R
esid
ual I
mpe
danc
e
ULURLLLR
Figure 81 Examination course in all 4 segments of the thorax during our investigation. Regional residual impedance showed in percent of total residual impedance. SP= Supine position, AT= Autotransfusion, CP= Control period, LS= Left side, PP= Prone position, CPAP disc. PP= After disconnection of CPAP, examination in prone position, UL= Upper left segment of the thorax, UR= Upper right segment of the thorax, LL= Lower left segment of the thorax, and LR= Lower right segment of the thorax.

112
RESIDUAL IMPEDANCE
Upper left Upper right Lower left Lower right Total Impedance
Supine Position 10275 (±36) 8021 (±33) 6426 (±29) 8414 (±25) 33136 Autotransfusion (SP)*
10133 (±40) 7407 (±18) 6459 (±26) 7761 (±25) 31760
Control Period (SP)*
10647 (±94) 7256 (±139) 6645 (±97) 7760 (±93) 32308
Left Side 12033(±101) 7377 (±64) 6139 (±213) 7474 (±82) 33023 Prone Position 12252(±41) 7827 (±80) 7442 (±61) 8186 (±78) 35707 PP – No CPAP 8206(±120) 5648 (±49) 4762 (±37) 6194 (±66) 24810 RESIDUAL IMPEDANCE %
Upper left Upper right Lower left Lower right Total Impedance
Supine Position 31 (±0.10) 24 (±0.09) 20 (±0.09) 25 (±0.08) 100 Autotransfusion (SP)*
32 (±0.13) 23 (±0.06) 20 (±0.08) 25 (±0.08) 100
Control Period (SP)*
33 (±0.30) 22 (±0.43) 21 (±0.30) 24 (±0.29) 100
Left Side 36 (±0.30) 22 (±0.19) 19 (±0.64) 23 (±0.24) 100 Prone Position 34 (±0.11) 22 (±0.22) 21 (±0.17) 23 (±0.21) 100 PP – No CPAP 33 (±0.48) 23 (±0.20) 19 (±0.15) 25 (±0.27) 100 Table 22 Regional residual impedance in all 4 segments of the thorax and total residual impedance in absolute numbers (above) and regional residual impedance in percent of total residual impedance (below). SDo is shown in brackets.
Tidal Impedance
Regional tidal impedance changes did not show such clear distribution within the 4 segments
of the thorax as regional residual impedance did.
Total and regional tidal impedance is determined by tidal volume and cardiovascular changes
within the thorax. Therefore tidal impedance changed with the body position. During supine
position under CPAP therapy we observed the highest tidal impedance changes in the upper
left segment at 30% of total tidal impedance, followed by the upper right and than the lower
segments.
Autotransfusion caused a clear decrease of tidal impedance of the upper right segment down
to 16% of total tidal impedance, but a clear increase in the lower left segment of 29% of total
tidal impedance occurs. During the control period, meaning that the infant was back in supine
position, tidal impedance of the upper right segment increased suddenly back up to 23% while o SD= standard deviation
113
tidal impedance of the lower left segment decreases down to 21% of total tidal impedance
again. Turned to the left side lower right segment showed the highest tidal impedance changes
at 31% of total tidal impedance while all three other segments’ tidal impedance was 23%
each. In prone position we detected high tidal impedance changes in the lower segments
(lower right: 40% of TTI and lower left: 24% of TTI) both taken together at 64% of TTI. In
prone position nearly 2/3 of tidal breathing took place in the lower segments. In all other
positions more than 50% of tidal impedance changes where detected in the upper segments.
Exception is autotransfusion, where the upper segments have 49% versus 51% of total tidal
impedance in the lower segments.
Subsequently we examined the infant during weaning of CPAP in prone position and
therefore breathing spontaneously. Tidal impedance of the upper left segment increased from
19% during CPAP therapy to 43% of total tidal impedance during spontaneous breathing and
only 40% of total tidal impedance were found in the lower segments. (LL: 17% and LR:
23%). In absolute numbers there was an enormous increase in tidal impedance during
spontaneously breathing from 266 to 508, which is an increase of 91%. At the same time a
decrease of 30% of total residual impedance was observed. (See fig 82-83, table 23)

114
Examination Course of all 4 Segments of the Thorax
40
90
140
190
240
SP AT CP LS PP CPAP disc. PP
Examination Period
Tida
l Im
peda
nce
ULURLLLR
Figure 82 Examination course of all 4 segments of the thorax during our investigation. SP= Supine position, AT= Autotransfusion, CP= Control period, LS= Left side, PP= Prone position, CPAP disc. PP=After disconnection of CPAP, examination in prone position, UL= Upper left segment of the thorax, UR= Upper right segment of the thorax, LL= Lower left segment of the thorax, and LR= Lower right segment of the thorax
Examination Course in Percent of Total Tidal Impedance
15
20
25
30
35
40
45
SP AT CP LS PP CPAP disc. PP
Examination Period
Tida
l Im
peda
nce
in P
erce
nt
ULURLLLR
Figure 83 Examination course in all 4 segments of the thorax during our investigation. Regional tidal impedance shown in percent of total tidal impedance SP= Supine position, AT= Autotransfusion, CP= Control period, LS= Left side, PP= Prone position, CPAP disc. PP= After disconnection of CPAP, examination in prone position, UL= Upper left segment of the thorax, UR= Upper right segment of the thorax, LL= Lower left segment of the thorax, and LR= Lower right segment of the thorax

115
TIDAL IMPEDANCE
Upper left Upper right Lower left Lower right Total Impedance
Supine Position 109 (±30) 98 (±24) 85 (±25) 76 (±22) 368 Autotransfusion (SP)*
129 (±29) 63 (±12) 113 (±23) 87 (±21) 392
Control Period (SP)*
125 (±54) 92 (±33) 87 (±31) 101 (±38) 405
Left Side 69 (±23) 71 (±20) 71 (±24) 95 (±32) 306 Prone Position 51 (±30) 45 (±23) 63 (±26) 107 (±28) 266 PP – No CPAP 223 (±61) 85 (±23) 84 (±30) 116 (±35) 508 TIDAL IMPEDANCE %
Upper left Upper right Lower left Lower right Total Impedance
Supine Position 30 (±8.15) 27 (±6.52) 23 (±6.79) 20 (±5.98) 100 Autotransfusion (SP)*
33 (±7.40) 16 (±3.06) 29 (±5.87) 22 (±5.36) 100
Control Period (SP)*
31 (±13.3) 23 (±8.15) 21 (±7.65) 25 (±9.38) 100
Left Side 23 (±7.52) 23 (±6.54) 23 (±7.84) 31 (±10.46) 100 Prone Position 19 (±11.28) 17 (±8.65) 24 (±9.77) 40 (±10.52) 100 PP – No CPAP 43 (±12.00) 17 (±4.53) 17 (±5.90) 23 (±6.89) 100 Table 23 Regional tidal impedance in all 4 segments of the thorax and total residual impedance (above) and regional tidal impedance in percent of total residual impedance (below). SDp is shown in brackets.
p SP= Supine Position
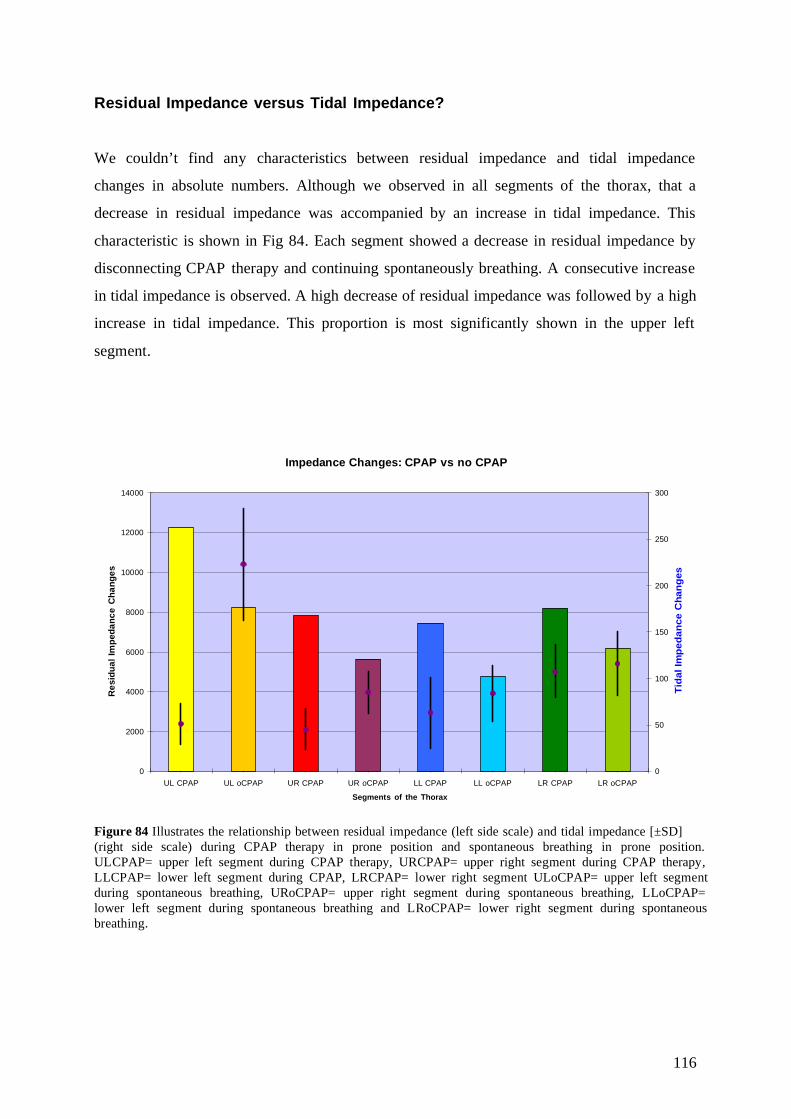
116
Residual Impedance versus Tidal Impedance? We couldn’t find any characteristics between residual impedance and tidal impedance
changes in absolute numbers. Although we observed in all segments of the thorax, that a
decrease in residual impedance was accompanied by an increase in tidal impedance. This
characteristic is shown in Fig 84. Each segment showed a decrease in residual impedance by
disconnecting CPAP therapy and continuing spontaneously breathing. A consecutive increase
in tidal impedance is observed. A high decrease of residual impedance was followed by a high
increase in tidal impedance. This proportion is most significantly shown in the upper left
segment.
Impedance Changes: CPAP vs no CPAP
0
2000
4000
6000
8000
10000
12000
14000
UL CPAP UL oCPAP UR CPAP UR oCPAP LL CPAP LL oCPAP LR CPAP LR oCPAP
Segments of the Thorax
Res
idua
l Im
peda
nce
Cha
nges
0
50
100
150
200
250
300
Tida
l Im
peda
nce
Cha
nges
Figure 84 Illustrates the relationship between residual impedance (left side scale) and tidal impedance [±SD] (right side scale) during CPAP therapy in prone position and spontaneous breathing in prone position. ULCPAP= upper left segment during CPAP therapy, URCPAP= upper right segment during CPAP therapy, LLCPAP= lower left segment during CPAP, LRCPAP= lower right segment ULoCPAP= upper left segment during spontaneous breathing, URoCPAP= upper right segment during spontaneous breathing, LLoCPAP= lower left segment during spontaneous breathing and LRoCPAP= lower right segment during spontaneous breathing.

117
CPAP Therapy versus Spontaneous Breathing
Total residual impedance during CPAP therapy in prone position was measured 35707 and
decreasing down to 24810 during spontaneous breathing in prone position which is a decrease
of nearly 31%. Tidal impedance increased from 266 to 508 at the same time, which is an
increase of 91% of total tidal impedance. Fig 85 demonstrates the decrease of residual
impedance of each segment of the thorax.
0
2000
4000
6000
8000
10000
12000
14000
Residual Impedance
Segments of the Thorax
Residual Impedance during CPAP Therapy and during Sponateous Breaths
UL CPAP
UR CPAP
LL CPAP
LR CPAP
UL
UR
LL
LR
Figure 85 Residual impedance in the 4 segments of the thorax. The bar graph shows eight columns, the first four on the left side illustrate residual impedance during CPAP therapy; the 4 from the right side illustrate residual impedance changes during spontaneous breaths. One color has been chosen for each segment of the thorax. We measured a decrease of total residual impedance during our investigation, but observed no
change in residual impedance distribution within the thorax from CPAP therapy to
spontaneous breathing. Decrease of residual impedance was detected in all 4 segments and
residual impedance distribution persisted. (Fig 86 & fig 87)

118
Residual Impedance Distribution in Percent of Total Residual Impedance during CPAP Therapy
Prone Position of the Infant in the Incubator, Head turned to the Left Side of the Infant
UL C P APUR C P APLL C P APLR C P AP
Residual Impedance in Percent of Total Residual Impedance during Sponateously Breathing
Prone Position during "Kangaroo Care", Head Turned to the Left Side of the Infant
UL oCPAPUR oCPAPLL oCPAPLR oCPAP
Figure 86 ResI distribution within the 4 segments Figure 87 ResI distribution within the 4 segments during CPAP therapy. UL= yellow segment, during spontaneous breathing. UL= yellow UR= red segment, LL= blue segment and segment, UR= red segment, LL= blue segment, LR= green segment, total residual impedance and LR= green segment, total residual impedance 35707 24810. Fig 88 and 89 show the proportions of tidal impedance during CPAP therapy and the
proportions during spontaneous breathing. There is a clear shifting from tidal impedance of
the lower right segment to the upper left segment during spontaneous breathing as well as a
little shifting from the lower left to the upper left, the upper right segment remains the same.
Tidal Volume in Percent of Total Tidal Impedance during CPAP Therapy-Prone Position in Incubator, Head Turned to the Left Side of the Infant
UL CP APUR CP APLL CP APLR CP AP
Tidal Impedance in Percent of Total Tidal Impedance during Sponateously Breathing-Prone Position during "Kangaroo Care", Head Turned to the Left Side of the Infant
UL o CP APUR o CP APLL oC PAPLR oCP AP
Figure 88 TidI distribution within the 4 segments Figure 89 TidI distribution within the 4 segments during CPAP therapy. UL= yellow segment, during spontaneous breathing. UL= yellow UR= red segment, LL= blue segment and segment, UR= red segment, LL= blue segment, LR= green segment and LR= green segment.

119
3.2.3 Summary of Infants with Assisted Ventilation
Infants with assisted ventilation did not show any clear distribution in tidal impedance nor
residual impedance during all examination periods like spontaneously breathing infants did.
Tidal impedance characteristic followed a clear order in supine position at a PEEP of 4.5cm
H2O which was the following: Upper left segment – lower right segment – upper right
segment – lower left segment. During decreasing PEEP to 3.5cm H2O tidal impedance in
every infant was affected differently and these characteristics diminished.
Residual impedance of the upper segments and the lower left segment showed about the same
distribution, only residual impedance of the lower right segment was lower in supine position.
This distribution of residual impedance in infants with assisted ventilation remained stable
through all examination periods and was not affected by a PEEP decrease or increase within a
period of 15 minutes for every examination period.
3.2.4 Spontaneously Breathing Infants versus Infants with Assisted
Ventilation
All spontaneously breathing infants showed a clear tendency in tidal impedance distribution
independently from body weight. Tidal impedance showed the following sequence starting
with the highest: Lower right segment – upper left segment – lower left segment and finally
upper right segment. We could not find this tendency in distribution in infants with assisted
ventilation. As we only studied four infants in the assisted ventilation infants group more
investigations may be necessary to detect any similarities in tidal impedance distribution
within individuals.
All spontaneously breathing infants with a body weight over 3kg displayed the same sequence
in residual impedance distribution, showing the following (starting with the segment of
highest residual impedance changes): Upper right segment – lower left segment – lower right
segment and finally upper left segment. This order could not be described in all infants with
assisted ventilation or all spontaneously breathing infants with less than 3kg.

120
3.2.5 Tidal Impedance and Residual Impedance Before and After
Extubation/ Weaning of CPAP
During our examinations we investigated two infants during extubation and weaning of
CPAP. (See “3.2 Infants with Assisted Ventilation”) Two infants is clearly not enough data to
come to a conclusion about the characteristics of both tidal impedance and residual
impedance. We have observed an increase in tidal impedance during weaning/ extubation
manoeuvre simultaneously with a decrease of residual impedance in the same segment. These
findings are most impressive in the upper left segment and the lower right segment of the
thorax, a fall of residual impedance leads to an increase of tidal impedance. Fig 90 displays
our observations in both infants before and after extubation/weaning of CPAP.
250,00200,00150,00100,0050,000,00
Tidal Impedance
12500,00
10000,00
7500,00
5000,00
2500,00
0,00
Res
idua
l Im
peda
nce
LRResISLRTidIS
LLResISLLTidIS
URResISURTidIS
ULResISULTidIS
LRResILRTidI
LLResILLTidI
URResIURTidI
ULResIULTidI
Figure 90 Tidal impedance and residual impedance in 2 infants during extubation/weaning manoeuvre and marked at their point of intersection (ResI+TidI). Four segments of the thorax are shown for both infants before and after extubation/ weaning. ULResI, ULTidI = Intersection of upper left residual impedance and upper left tidal impedance. ResI= Residual impedance on ventilation, ResIS= Residual impedance during spontaneous breaths, TidI= Tidal impedance on ventilation and TidIS= Tidal impedance during spontaneous breaths, UR= upper right segment, LL=lower left segment, and LR= lower right segment.
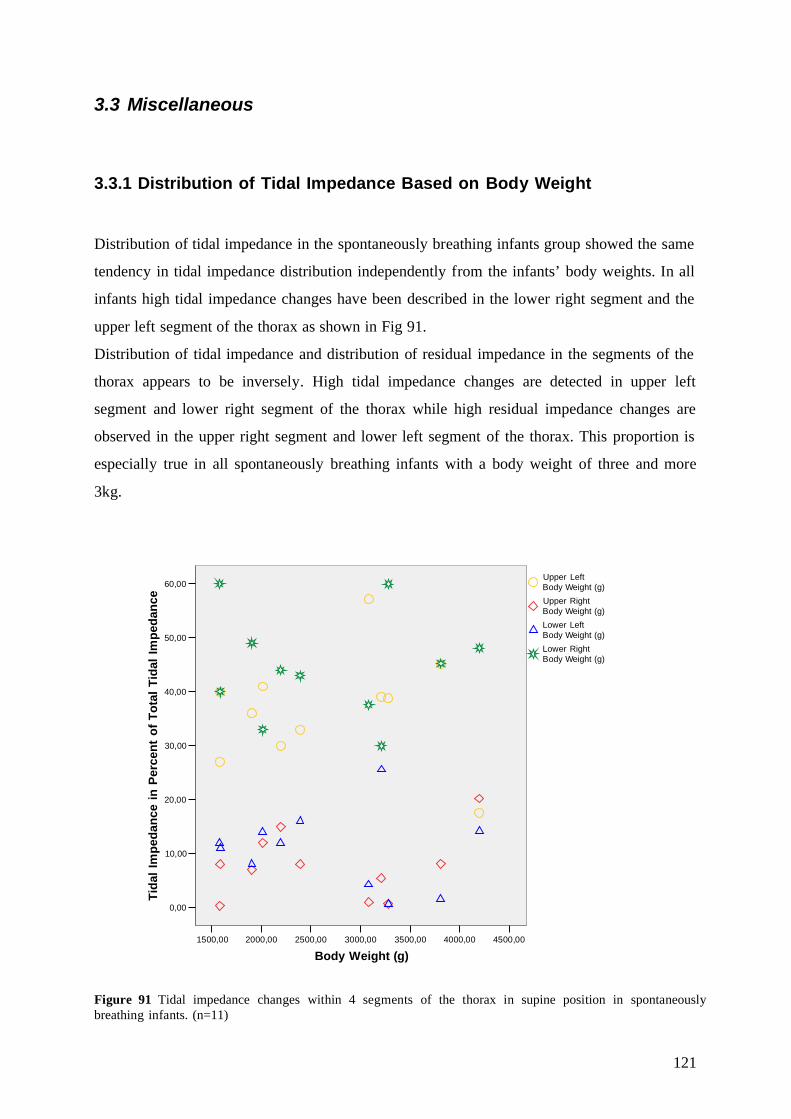
121
3.3 Miscellaneous
3.3.1 Distribution of Tidal Impedance Based on Body Weight
Distribution of tidal impedance in the spontaneously breathing infants group showed the same
tendency in tidal impedance distribution independently from the infants’ body weights. In all
infants high tidal impedance changes have been described in the lower right segment and the
upper left segment of the thorax as shown in Fig 91.
Distribution of tidal impedance and distribution of residual impedance in the segments of the
thorax appears to be inversely. High tidal impedance changes are detected in upper left
segment and lower right segment of the thorax while high residual impedance changes are
observed in the upper right segment and lower left segment of the thorax. This proportion is
especially true in all spontaneously breathing infants with a body weight of three and more
3kg.
4500,004000,003500,003000,002500,002000,001500,00
Body Weight (g)
60,00
50,00
40,00
30,00
20,00
10,00
0,00
Tida
l Im
peda
nce
in P
erce
nt o
f Tot
al T
idal
Impe
danc
e
Lower RightBody Weight (g)
Lower LeftBody Weight (g)
Upper RightBody Weight (g)
Upper LeftBody Weight (g)
Figure 91 Tidal impedance changes within 4 segments of the thorax in supine position in spontaneously breathing infants. (n=11)

122
3.3.2 Distribution of Residual Impedance Based on Body Weight
Residual impedance distribution showed different results according to body weight of the
infants. Infants with a body weight less than 2,5kg did not show a uniform residual impedance
distribution, while infants in our study group >3kg showed a consistent distribution. Residual
impedance of all infants weighing 3kg and more was higher in the upper right segment and
the lower left segment and residual impedance in the upper left segment and the lower right
segment was consistently lower. For detail see fig.92.
4500,004000,003500,003000,002500,002000,001500,00
Body Weight (g)
40,00
30,00
20,00
10,00Res
idua
l Im
peda
nce
in P
erce
nt o
f Tot
al R
esI
Lower RightBody Weight (g)
Lower LeftBody Weight (g)
Upper RightBody Weight (g)
Upper LeftBody Weight (g)
Figure 92 Distribution of residual impedance changes within the thorax based on body weight of spontaneously breathing infants (n=11)

123
3.3.3 Effect of Incorrectly Placed Electrodes on the Results
In one spontaneously breathing infant with a body weight of 3210g electrode positions have
been changed on the front side of the thorax. The switched electrodes were the lower right and
lower left electrode. Therefore the signal recorded in between these 4 lower electrodes
changed and affect the result of both tidal impedance and residual impedance changes. Fig 93
visualizes the common electrode position during our measurements (left) and the new
electrode position in this examination (right).
.
Total tidal impedance decreased from supine position with the common electrode position to
supine position with the replaced electrode position 67,71% in total, in the upper left segment
31,41%, in upper right segment 84,48%, in lower left 85,49%, and in lower right segment
96,87%. Electrode replacement (and therefore electrode misplacement) clearly changed tidal
impedance changes in all four segments of the thorax but to a different extent in each
segment. (Fig 94-95) Tidal impedance distribution showed the following order before the
replacement of the electrodes, which has been observed in spontaneously breathing infants as
described above: Tidal impedance changes of the upper left segment and upper right segment
are higher than tidal impedance changes of the upper right segment and the lower left
segment.
Lower right electrodes
Lower left electrodes
Figure 93 The lower electrodes in the front of the thorax have been switched and therefore signals have been detected through the cross-section of the thorax at the 5th intercostal space.
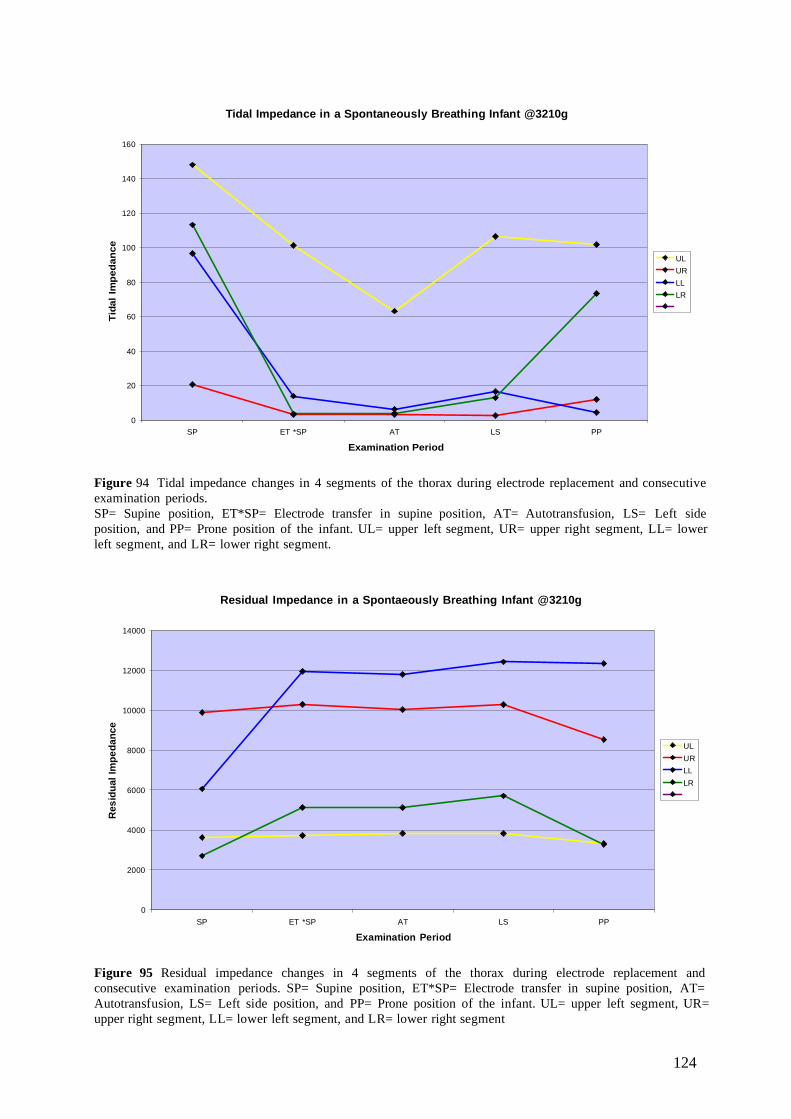
124
Tidal Impedance in a Spontaneously Breathing Infant @3210g
0
20
40
60
80
100
120
140
160
SP ET *SP AT LS PP
Examination Period
Tida
l Im
peda
nce
ULURLLLR
Figure 94 Tidal impedance changes in 4 segments of the thorax during electrode replacement and consecutive examination periods. SP= Supine position, ET*SP= Electrode transfer in supine position, AT= Autotransfusion, LS= Left side position, and PP= Prone position of the infant. UL= upper left segment, UR= upper right segment, LL= lower left segment, and LR= lower right segment.
Residual Impedance in a Spontaeously Breathing Infant @3210g
0
2000
4000
6000
8000
10000
12000
14000
SP ET *SP AT LS PP
Examination Period
Res
idua
l Im
peda
nce
ULURLLLR
Figure 95 Residual impedance changes in 4 segments of the thorax during electrode replacement and consecutive examination periods. SP= Supine position, ET*SP= Electrode transfer in supine position, AT= Autotransfusion, LS= Left side position, and PP= Prone position of the infant. UL= upper left segment, UR= upper right segment, LL= lower left segment, and LR= lower right segment
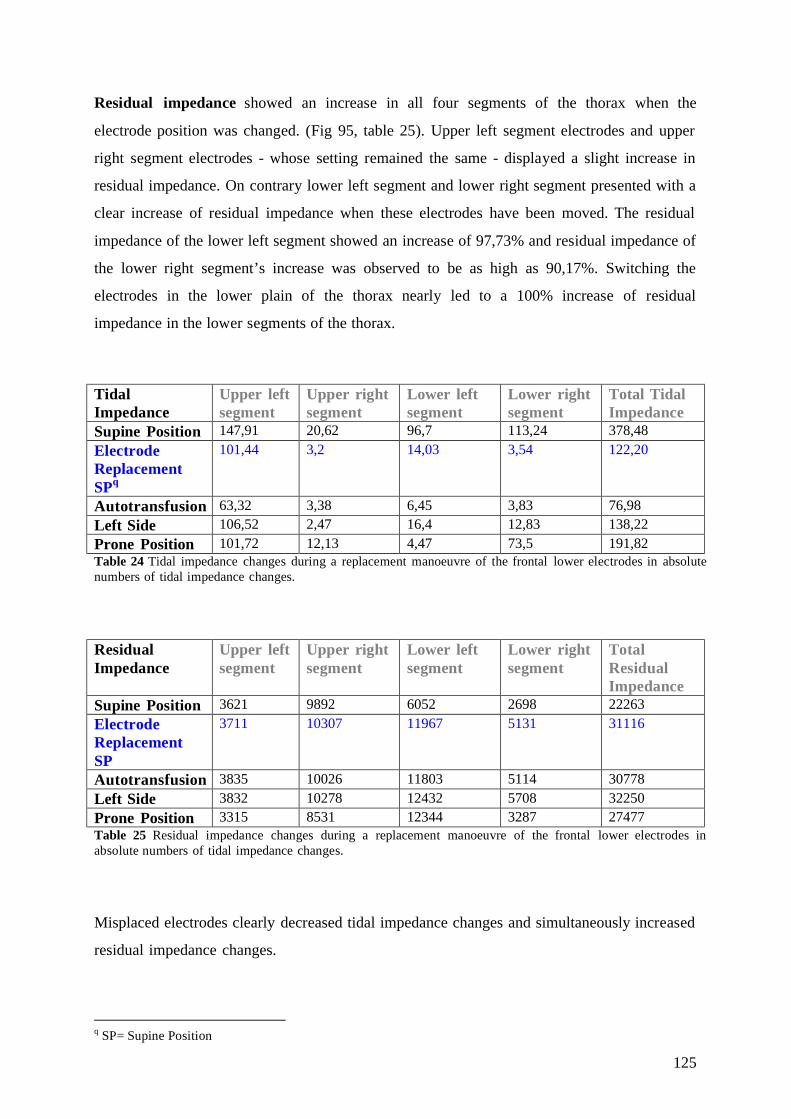
125
Residual impedance showed an increase in all four segments of the thorax when the
electrode position was changed. (Fig 95, table 25). Upper left segment electrodes and upper
right segment electrodes - whose setting remained the same - displayed a slight increase in
residual impedance. On contrary lower left segment and lower right segment presented with a
clear increase of residual impedance when these electrodes have been moved. The residual
impedance of the lower left segment showed an increase of 97,73% and residual impedance of
the lower right segment’s increase was observed to be as high as 90,17%. Switching the
electrodes in the lower plain of the thorax nearly led to a 100% increase of residual
impedance in the lower segments of the thorax.
Tidal Impedance
Upper left segment
Upper right segment
Lower left segment
Lower right segment
Total Tidal Impedance
Supine Position 147,91 20,62 96,7 113,24 378,48 Electrode Replacement SPq
101,44 3,2 14,03 3,54 122,20
Autotransfusion 63,32 3,38 6,45 3,83 76,98 Left Side 106,52 2,47 16,4 12,83 138,22 Prone Position 101,72 12,13 4,47 73,5 191,82 Table 24 Tidal impedance changes during a replacement manoeuvre of the frontal lower electrodes in absolute numbers of tidal impedance changes.
Residual Impedance
Upper left segment
Upper right segment
Lower left segment
Lower right segment
Total Residual Impedance
Supine Position 3621 9892 6052 2698 22263 Electrode Replacement SP
3711 10307 11967 5131 31116
Autotransfusion 3835 10026 11803 5114 30778 Left Side 3832 10278 12432 5708 32250 Prone Position 3315 8531 12344 3287 27477 Table 25 Residual impedance changes during a replacement manoeuvre of the frontal lower electrodes in absolute numbers of tidal impedance changes.
Misplaced electrodes clearly decreased tidal impedance changes and simultaneously increased
residual impedance changes.
q SP= Supine Position
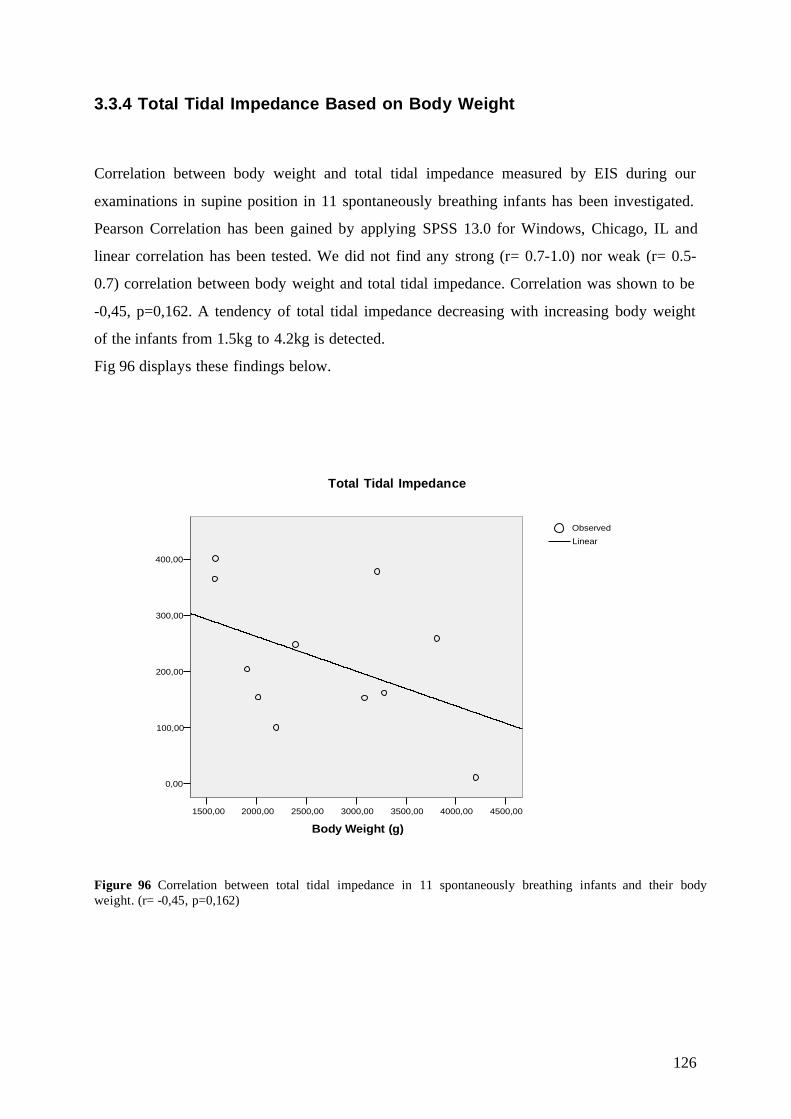
126
3.3.4 Total Tidal Impedance Based on Body Weight
Correlation between body weight and total tidal impedance measured by EIS during our
examinations in supine position in 11 spontaneously breathing infants has been investigated.
Pearson Correlation has been gained by applying SPSS 13.0 for Windows, Chicago, IL and
linear correlation has been tested. We did not find any strong (r= 0.7-1.0) nor weak (r= 0.5-
0.7) correlation between body weight and total tidal impedance. Correlation was shown to be
-0,45, p=0,162. A tendency of total tidal impedance decreasing with increasing body weight
of the infants from 1.5kg to 4.2kg is detected.
Fig 96 displays these findings below.
400,00
300,00
200,00
100,00
0,00
4500,004000,003500,003000,002500,002000,001500,00
Body Weight (g)
LinearObserved
Total Tidal Impedance
Figure 96 Correlation between total tidal impedance in 11 spontaneously breathing infants and their body weight. (r= -0,45, p=0,162)

127
3.3.5 Total Residual Impedance Based on Body Weight
Correlation between total residual impedance in 11 spontaneously breathing infants and their
body weight has been studied. An increase of total residual impedance with increasing body
weight has been observed during our investigations. Pearson correlation has been employed in
this study and a correlation of 0,55 is detected (p=0,077). Therefore weak correlation between
increase of body weight and increase in total residual impedance is given in the spontaneously
breathing infants group. Fig 97 visualizes our findings.
40000,00
30000,00
20000,00
10000,00
4500,004000,003500,003000,002500,002000,001500,00
Body Weight (g)
LinearObserved
Total Residual Impedance
Figure 97 Correlation between total residual impedance and body weight in 11 spontaneously breathing infants. (r=0,55)

128
3.3.6 Residual Impedance in the Lower Left Segment of the Thorax Based
on Body Weight
During our investigations we observed an increase of residual impedance distribution of the
lower left segment within the thorax. While residual impedance distribution in small infants
with about 1.5-2.0 kg was around 20% of total residual impedance, it decreased up to 35% in
infants around 3kg. In the lower left segment EIS measurements detect residual impedance of
both lungs and heart. Based on these observations we applied Pearson Correlation to identify
the characteristics of residual impedance in the lower left segment of the thorax and the
infants’ body weight.
R= 0,71 (p=0,013) and is considered strongly significant when residual impedance of the
lower left segment is correlated to the body weight. Fig 98 demonstrates these observations
closely.
40,00
35,00
30,00
25,00
20,00
15,00
4500,004000,003500,003000,002500,002000,001500,00
Body Weight (g)
LinearObserved
Lower Left
Figure 98 Significant correlation between residual impedance in the lower left segment of the thorax and body weight of infants. (r=0,71)

129
3.3.7 Different Breathing Pattern in Infants
Different breathing pattern during our examinations have been detected in both spontaneously
breathing infants and infants with assisted ventilation. Samples of recorded breathing pattern
are shown to display the variability of breathing in infants.
Spontaneous Breathing
Electrical impedance segmentography does not only detect the height of tidal impedance but
the characteristics of breathing. Apnea and tachypnea may be easily monitored by EIS as well
as the shape of single and multiple breaths. In most infants we observed continuous breaths
with a rate of 30-60 breaths per minute, but the shape of breaths may have varied within the
infants and examination periods. Apnea and tachypnea have been disclosed and are described
above. (See “2.5.4 Breathing Pattern”) Fig 99 visualizes a sample of spontaneously breathing
of an infant in supine position in all four segments within the thorax. Tidal impedance
changes and their height (red lines) are shown over one minute.
Figure 99 Spontaneously breathing infant over one minute, breathing frequency 47, tidal impedance in 4 segments of the lungs.

130
Turning the Head from the Right Side to the Left Side of the Body
A spontaneously breathing infant (1.5kg) has been examined in prone position while the
infant’s head was turned to the right side of the newborn. Fig 100 shows tidal impedance
recorded in four segments of the thorax during this examination.
Figure 100 Infant (1.5kg) breathing spontaneously in prone position, head turned to the right side of the infant.
After the head of the infant has been turned to the left side of the infant by the investigator,
breathing pattern of the infant changed significantly and tidal impedance signal of the upper
right segment and the lower right segment appeared to be “mirrored” to the other two
segments of the thorax.
Figure 101 Infant (1.5kg) breathing spontaneously in prone position, head turned to the left side of the infant.
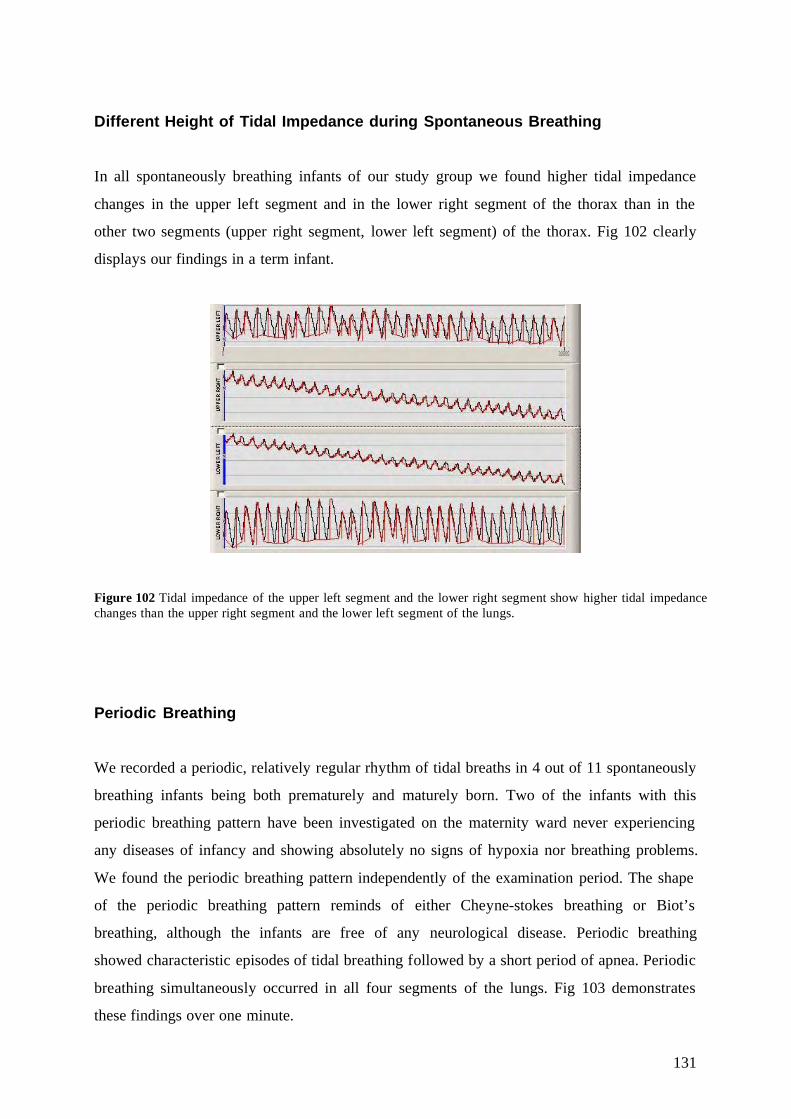
131
Different Height of Tidal Impedance during Spontaneous Breathing
In all spontaneously breathing infants of our study group we found higher tidal impedance
changes in the upper left segment and in the lower right segment of the thorax than in the
other two segments (upper right segment, lower left segment) of the thorax. Fig 102 clearly
displays our findings in a term infant.
Figure 102 Tidal impedance of the upper left segment and the lower right segment show higher tidal impedance changes than the upper right segment and the lower left segment of the lungs.
Periodic Breathing
We recorded a periodic, relatively regular rhythm of tidal breaths in 4 out of 11 spontaneously
breathing infants being both prematurely and maturely born. Two of the infants with this
periodic breathing pattern have been investigated on the maternity ward never experiencing
any diseases of infancy and showing absolutely no signs of hypoxia nor breathing problems.
We found the periodic breathing pattern independently of the examination period. The shape
of the periodic breathing pattern reminds of either Cheyne-stokes breathing or Biot’s
breathing, although the infants are free of any neurological disease. Periodic breathing
showed characteristic episodes of tidal breathing followed by a short period of apnea. Periodic
breathing simultaneously occurred in all four segments of the lungs. Fig 103 demonstrates
these findings over one minute.

132
Figure 103 Periodic breathing in a 1.5kg premature infant without any respiratory or neurological disease.
Fig 104 displays a periodic breathing pattern with crescendo-decrescendo alternation of tidal
impedance and short apneic episodes. Fig 105 visualizes these findings during breastfeeding
by the mother in left side position of the infant over one minute.
Figure 104 Periodic breathing in a 3.8kg infant Figure 105 Periodic breathing in the same infant during left side position. during breastfeeding.
Fig 106 illustrates crescendo-decrescendo alternation of tidal breaths without apneic episodes
over one minute in a 2kg premature infant.
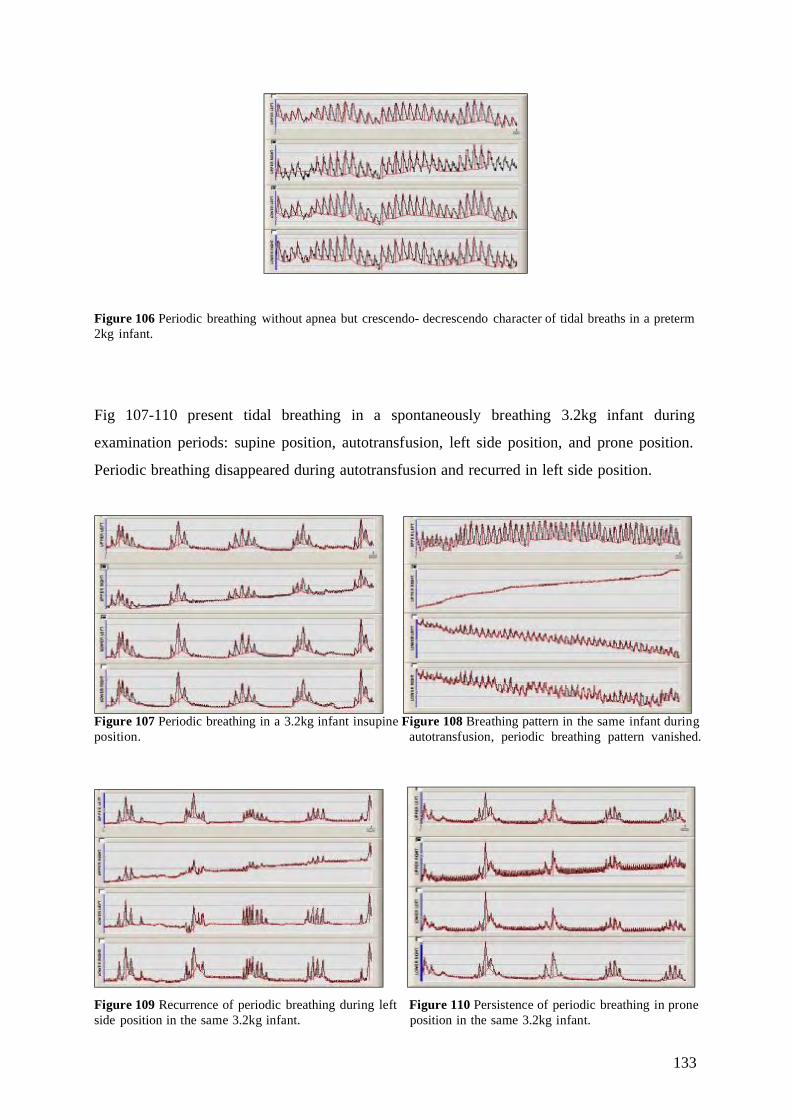
133
Figure 106 Periodic breathing without apnea but crescendo- decrescendo character of tidal breaths in a preterm 2kg infant.
Fig 107-110 present tidal breathing in a spontaneously breathing 3.2kg infant during
examination periods: supine position, autotransfusion, left side position, and prone position.
Periodic breathing disappeared during autotransfusion and recurred in left side position.
Figure 107 Periodic breathing in a 3.2kg infant in supine Figure 108 Breathing pattern in the same infant during position. autotransfusion, periodic breathing pattern vanished.
Figure 109 Recurrence of periodic breathing during left Figure 110 Persistence of periodic breathing in prone side position in the same 3.2kg infant. position in the same 3.2kg infant.

134
Breathing Pattern on CPAP
During CPAP (4.5cm H2O) of a 1.5kg premature infant no significant breathing pattern has
been observed. Recorded data of tidal impedance resembles tidal impedance changes during
spontaneous breathing. Fig 111 demonstrates these finding over one minute with a breathing
frequency of 53.
Figure 111 1.5kg premature infant on CPAP over one minute.
Breathing Pattern during Synchronized Intermittent Mandatory Ventilation
We studied three infants on SIMV during our investigation. Two were free of respiratory
disease, which have been ventilated 1.) due to a shunt operation of a hydrocephalus and 2.)
due to birth asphyxia. The third infant presented with a pneumothorax and is described in
detail below. SIMV displays a characteristic breathing pattern in all four segments of the
thorax due to its trigger function. Fig 112 illustrates these findings in a 3.2kg asphyxiated
infant on SIMV with PEEP 5.5cm H2O.

135
Figure 112 Tidal impedance changes in a 3.2kg infant on SIMV with birth asphyxia.
Fig 113 visualizes our recordings of a 2kg infant on SIMV with PEEP 4.5cm H2O after shunt
operation displaying the same characteristics of tidal impedance as in Fig 112.
Figure 113 Tidal impedance changes in a 2kg infant on SIMV after shunt operation.

136
Breathing Pattern in an Infant on SIMV Presenting with a Pneumothorax
An alternation of the breathing pattern has been observed in a male infant (2.9kg) presenting
with pneumothorax on SIMV with PEEP 4.5cm H2O. During our investigation we decreased
PEEP to 3.5cm H2O and increased PEEP after 15min to 5.5cm H2O. In this boy breathing
pattern changed when we decreased PEEP and remained in its new pattern, it did not changes
back to a more characteristic pattern for SIMV when PEEP was increased again. (Fig 114-
116)
Figure 114 Tidal impedance changes in a 2.9kg infant on SIMV and PEEP 4.5cm H2O due to a pneumothorax.
Figure 115 Tidal impedance changes in a 2.9kg infant Figure 116 Tidal impedance changes in a 2.9kg infant on SIMV and PEEP 3.5cm H2O. on SIMV and PEEP 5.5cm H2O
137
3.3.8 The Impact of Feeding on Tidal Impedance and Residual Impedance
During our investigations of a spontaneously breathing dizygotic twin boy (1905g, GA 31+2
wks and day of life 21) in left side position, he has been incidentally feed through the
nasogastric tube by the nurse in charge. He received 20ml of breast milk over 15-20 minutes.
The feeding was performed when the infant has been examined in left side position. Although
this observation was erring from our protocol, the result recorded is rather interesting.
Tidal Impedance
Tidal impedance changes have been recorded in this boy and observations erring from the
main observations have been made during left side position when the infant was fed
unintentionally. Tidal impedance of the upper left segment of the thorax increased from
61,89 during control period to 99,45 in left side position when the infant was fed through a
NG tube. We detected an increase of tidal impedance in the upper left segment of 32,7% by
the feeding manoeuvre. While tidal impedance of the upper right segment and the lower left
segment remained stable and were not affected by the feeding of the infant, tidal impedance
of the lower right segment fell from 66,19 during control period to 34,19 during feeding in
left side position, which is a decrease of tidal impedance of 48,34%. Interestingly total tidal
impedance was hardly affected by feeding. (Total tidal impedance in control period: 160,76;
left side position: 168,79) After the 15minutes examination period the infant was turned back
to prone position. The 15 th minute of prone position has been used for analysis in which tidal
impedance of the upper left segment decreased and tidal impedance of the lower right
segment came back up again. Fig 117 visualizes these findings and table 25 shows our
observations.

138
Tidal Impedance in a Sponateously Breathing Infant @1905g
0
20
40
60
80
100
120
SP AT CP LS PP
Examination Period
Tida
l Im
peda
nce
ULURLLLR
Figure 117 Tidal impedance in a spontaneously breathing infant with a body weight of 1905g during examination periods when feeding was performed in left side position. UL= upper left segment, UR= upper right segment, LL= lower left segment, LR= lower right segment. SP= supine position, AT= autotransfusion, CP= control period, LS= left side position, and PP= prone position.
Tidal Impedance Supine Position Autotransfusion
Control Period
Left Side Position
Prone Position
UL 73,33 70,31 61,89 99,45 53,7 UR 14,33 16,3 16 14 10,93 LL 15,72 20,72 16,68 21,15 16 LR 100,78 87,3 66,19 34,19 42,24 Total TidI 204,16 194,63 160,76 168,79 122,87
Table 25 Tabulated tidal impedance changes in assessed numbers in a spontaneously breathing premature with a body weight of 1905g. UL= upper left segment, UR= upper right segment, LL= lower left segment, LR= lower right segment, TidI= Tidal impedance.

139
Residual Impedance At the same time when tidal impedance increased residual impedance of the upper left
segment increased from 2139 during control period to 12251 in left side position when the
infant was fed. Feeding caused an increase of 472% in residual impedance. The other three
segments were not majorly affected by the feeding of the infant. Turning the newborn back to
prone position, residual impedance of the upper left segment immediately decreased to 2899.
Fig 118 displays these findings below and table 26 illustrates the results.
Residual Impedance in a Spontaneously Breathing Infant @1905g
0
2000
4000
6000
8000
10000
12000
14000
SP AT CP LS PP
Examination Period
Res
idua
l Im
peda
nce
ULURLLLR
Figure 118 Residual impedance in a spontaneously breathing infant with a body weight of 1905g during examination periods when feeding was performed in left side position. UL= upper left segment, UR= upper right segment, LL= lower left segment, LR= lower right segment. SP= supine position, AT= autotransfusion, CP= control period, LS= left side position, and PP= prone position.
Residual Impedance Supine Position Autotransfusion
Control Period
Left Side Position Prone Position
UL 2992 2706 2139 12251 2899 UR 4562 4245 3296 3915 4514 LL 3477 3380 2592 2747 3295 LR 4108 3616 3032 3347 3845 Total ResI 15139 13947 11059 22260 14553
Table 26 Tabulated residual impedance changes in assessed numbers in a spontaneously breathing premature with a body weight of 1905g. UL= upper left segment, UR= upper right segment, LL= lower left segment, LR= lower right segment, ResI= residual impedance.

140
3.3.9 The Effect of Crying on Tidal Impedance and Residual Impedance
In our spontaneously breathing infants group we examined one 5-day-old healthy term boy
with a birth weight of 3810g and a gestational age of 38+2 weeks. We investigated this infant
during its postnatal stay in our maternity ward. Usually mothers of the term infants in the
maternity ward have breast fed their infants before we have started our investigations to more
likely observe a period of sleep and therefore mostly free of motion artifacts. This term boy
showed us at least 10 minutes of continuously crying after breastfeeding by the mother. In this
boy we decided to further assess impedance changes by EIS during breastfeeding by the
mother and the followed period of crying.
Tidal Impedance
Tidal impedance changes have been monitored during supine position, left side position
(while the infant first has been breastfed by the mother and secondly crying intensely), and in
prone position. We observed stable total tidal impedance during feeding in that term infant,
regional tidal impedance increased in the upper left segment from 116,6 in supine position to
139,29 during breastfeeding in left side position of the infant while regional tidal impedance
decreased from 20,89 in supine position to 4,03 in left side position. In the upper left segment
we detected an increase of tidal impedance of 19,4% during breastfeeding while tidal
impedance of the upper right segment decreased 80,7% of its initial value in supine position.
Tidal impedance of the lower right segment increased about the same amount as tidal
impedance in the upper left segment, which was from 117,19 in supine position to 130,91
which is an increase of 11,7%. Tidal impedance of the lower left segment remained stable.
Furthermore the effect of crying has been studied in this infant. Interestingly tidal impedance
immediately increased during crying of the infant in all four segments and to the following
extent: Left Side Feeding Left Side Crying Increase % of TidI
Upper left segment 139,29 153,7 10,3 % Upper right segment 4,03 100,54 2394 % Lower left segment 2,96 23,93 708% Lower right segment 130,91 144,11 10,1% Total Tidal Impedance 277,19 422,28 52,34%

141
A very impressive increase of tidal impedance of the upper right segment is discovered and
we have disclosed a nearly as impressive increase of tidal impedance in the lower left
segment. Fig 119 clearly illustrates these results and table 27visualizes these findings.
Tidal Impedance in a Spontaneously Breathing Infant @3810g
0
20
40
60
80
100
120
140
160
180
SP LS *feeding LS crying PP
Examination Period
Tida
l Im
peda
nce
ULURLLLR
Figure 119 Tidal impedance changes in a spontaneously breathing, healthy 3.8kg infant during placement in left side position and prone position. Left side position (LS) crying and left side position feeding took a time period of 15 min for both, the same as supine position (SP) and prone position (PP) each. UL= upper left segment, UR= upper right segment, LL= lower left segment, LR= lower right segment
Tidal Impedance
Supine Position
Left Side *feeding
Left Side *crying
Prone Position
UL 116,6 139,29 153,7 86,84 UR 20,89 4,03 100,54 6,3 LL 4,12 2,96 23,93 1,88 LR 117,19 130,91 144,11 63,89 Total TidI 258,8 277,19 422,28 158,91
Table 27 Tabulated tidal impedance changes in assessed numbers in a spontaneously breathing premature with a body weight of 1905g. UL= upper left segment, UR= upper right segment, LL= lower left segment, LR= lower right segment, TidI= Tidal impedance.

142
Residual Impedance
Residual impedance has been observed first in supine position and secondly when the infant
was breastfed by the mother in left side position. As observed above (See “3.3.8 The Impact
of Feeding on Tidal Impedance and Residual Impedance”) regional residual impedance of the
upper left segment increased from 6777 in supine position to 9219 in left side position during
feeding which presents with an increase of 26,48%. Regional residual impedance of the lower
right segment increased from 4884 in supine position to 6817 during breastfeeding in left side
position which is an increase of 28,35%. Regional residual impedance of the upper right
segment and the lower left segment remained stable. Total residual impedance increased from
37835 in supine position to 41456 during breastfeeding in left side position displaying an
overall residual impedance increase of 8,73%.
Furthermore we investigated residual impedance during crying continuously in left side
position. Crying of the infant mainly showed a decrease in regional residual impedance in the
upper left segment of the thorax of 21,41% and a decrease in the upper right segment of
28,3%. Total residual impedance decreased 15,35% while the infant was crying intensely.
Detailed information about residual impedance decrease is given below:
Left Side Feeding Left Side Crying Decrease % of ResI Upper left segment 9219 7245 21,41% Upper right segment 12703 8981 29,3% Lower left segment 12717 12248 3,68% Lower right segment 6817 6622 2,86% Total Residual Impedance 41456 35096 15,35%
Fig 120 demonstrates these findings and table 28 presents our results in a term infant during
feeding and crying in left side position.
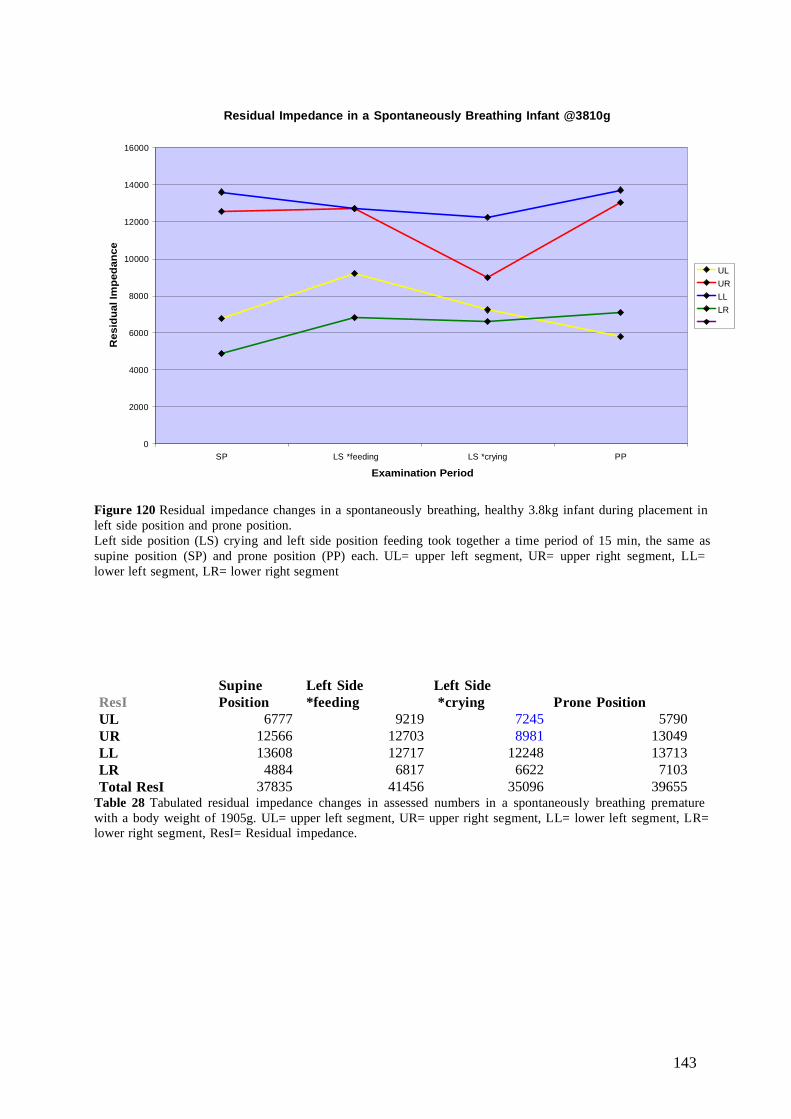
143
Residual Impedance in a Spontaneously Breathing Infant @3810g
0
2000
4000
6000
8000
10000
12000
14000
16000
SP LS *feeding LS *crying PP
Examination Period
Res
idua
l Im
peda
nce
ULURLLLR
Figure 120 Residual impedance changes in a spontaneously breathing, healthy 3.8kg infant during placement in left side position and prone position. Left side position (LS) crying and left side position feeding took together a time period of 15 min, the same as supine position (SP) and prone position (PP) each. UL= upper left segment, UR= upper right segment, LL= lower left segment, LR= lower right segment
ResI Supine Position
Left Side *feeding
Left Side *crying Prone Position
UL 6777 9219 7245 5790 UR 12566 12703 8981 13049 LL 13608 12717 12248 13713 LR 4884 6817 6622 7103 Total ResI 37835 41456 35096 39655
Table 28 Tabulated residual impedance changes in assessed numbers in a spontaneously breathing premature with a body weight of 1905g. UL= upper left segment, UR= upper right segment, LL= lower left segment, LR= lower right segment, ResI= Residual impedance.
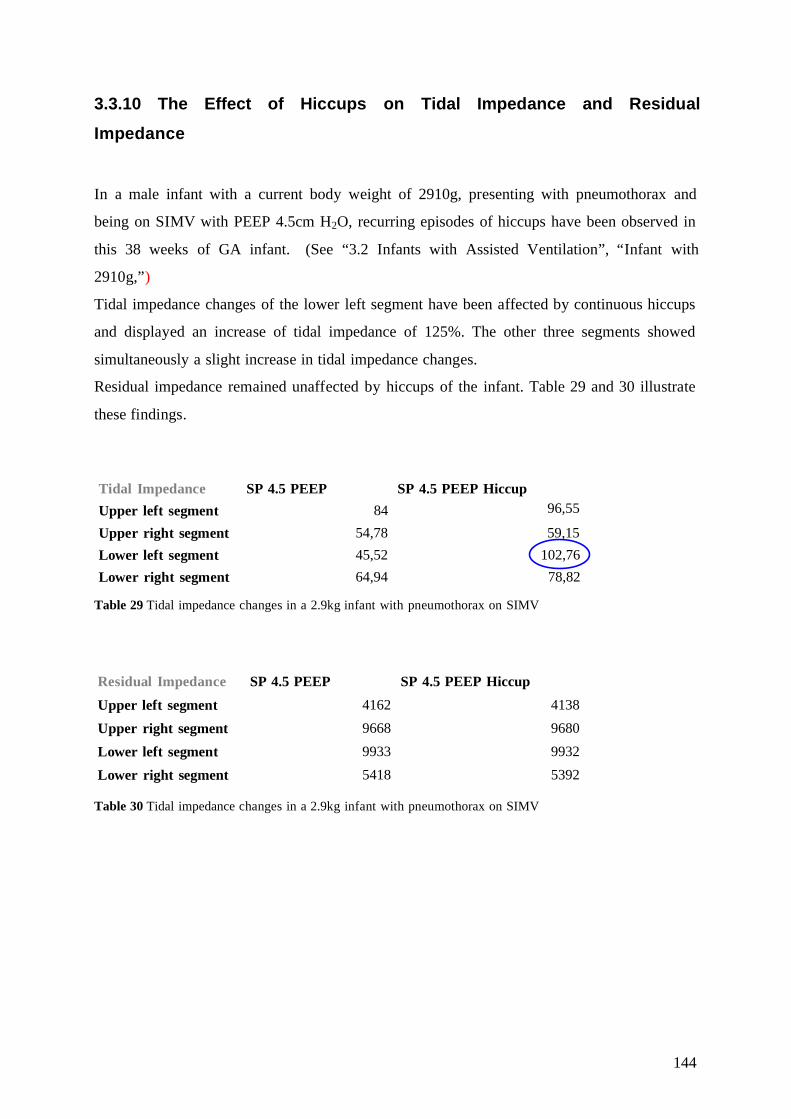
144
3.3.10 The Effect of Hiccups on Tidal Impedance and Residual
Impedance
In a male infant with a current body weight of 2910g, presenting with pneumothorax and
being on SIMV with PEEP 4.5cm H2O, recurring episodes of hiccups have been observed in
this 38 weeks of GA infant. (See “3.2 Infants with Assisted Ventilation”, “Infant with
2910g,”)
Tidal impedance changes of the lower left segment have been affected by continuous hiccups
and displayed an increase of tidal impedance of 125%. The other three segments showed
simultaneously a slight increase in tidal impedance changes.
Residual impedance remained unaffected by hiccups of the infant. Table 29 and 30 illustrate
these findings.
Table 29 Tidal impedance changes in a 2.9kg infant with pneumothorax on SIMV
Residual Impedance SP 4.5 PEEP SP 4.5 PEEP Hiccup Upper left segment 4162 4138
Upper right segment 9668 9680
Lower left segment 9933 9932
Lower right segment 5418 5392 Table 30 Tidal impedance changes in a 2.9kg infant with pneumothorax on SIMV
Tidal Impedance SP 4.5 PEEP SP 4.5 PEEP Hiccup Upper left segment 84 96,55
Upper right segment 54,78 59,15 Lower left segment 45,52 102,76 Lower right segment 64,94 78,82

145
IV. Discussion
4.1 Electrical Impedance Segmentography: A New Generation in
Bedside Lung Control of Newborns?
4.1.1 Spontaneously Breathing Infants
Electrical impedance segmentography has been employed in this study to investigate the
lungs of eleven spontaneously breathing infants. We subdivided the spontaneously breathing
infants into three groups according to their current body weight to observe both similarities
and particular findings in detail.
The aim of our investigation was to test whether tidal impedance and residual impedance can
be assessed by EIS in infants and to find any similarities in both tidal impedance and residual
impedance distribution. Regional functional residual capacity (FRC) and tidal volume (V T) of
the lungs remain unknown until today but information about both regional tidal volume
distribution and regional FRC distribution would significantly improve mechanical ventilation
and continuous positive airway pressure therapy.25
Methods to Monitor FRC of the Lungs
FRC is the only static lung volume which can be measured in infants. Several methods have
been developed to assess FRC in human lungs.
Bodyplethysmography has been used to obtain FRC of the lungs of infants, collection of
reference data is suggested and standard values for comparison of data are requested.31 FRC
can be reliably obtained by bodyplethysmography, although it can only detect a total value for
FRC and regional FRC distribution remains unknown.
Gas dilution, such as helium dilution technique, provides information about total FRC within
the lungs. It is a labor-intensive procedure, requiring trained personnel and may be invasive in
an unstable infant.32 Therefore assessing FRC of the lungs in infants is limited so far and
regional FRC cannot be estimated. Ventilator settings are adjusted according to x-ray findings
and a dire need for more accurately adjustment options is given.

146
Methods to Monitor VT of the Lungs
Electrical impedance tomography (EIT) was first described by Brown et al6 as a reliable
method to assess tidal volume changes and obtain cross-section scans of the thorax within one
plain to achieve information of the lungs. Several studies have been performed in the last 30
years to assess infants’ lungs by EIT. 6-12
EIT has been studied in premature infants by Dunlop et al 7, and Frerichs et al. 14. Distribution
of lung ventilation has been observed in both spontaneously breathing infants and infants with
assisted ventilation. EIT has been applied to determine the effect of irregular breathing pattern
and posture on the spatial distribution of ventilation within the lungs. 14 Frerichs et al observed
regional lung ventilation meaning they compared the ventilation of the right lung with the
ventilation of the left lung. Furthermore comparison between our EIS device and conventional
EIT measurements is limited, EIT gains information of cross-section scans in one horizontal
plain. We investigated four segments of the thorax and detected more lung tissue but are
unable to differentiate between dependent and independent parts of the lungs. Independently
from the method applied it can be clearly stated that lung ventilation is not homogenous
distributed. We investigated tidal impedance and residual impedance in 11 spontaneously
breathing infants. Our tidal impedance distribution showed the following order starting with
the highest (See “3.1.5 Summary of Spontaneously Breathing Infants”): Lower right segment
– upper left segment – upper right segment – lower left segment independently from the
position the infant was investigated in. Literature on tidal impedance distribution within the
lungs is extremely limited. One pilot trial has been performed by Guerrero et al33 in 3 grown-
ups to study tidal ventilation distribution by 4D-CT. r The authors described tidal volume
distribution as uniform within each individual. In our examinations we found a clear tendency
of tidal impedance distribution but still including slight individual variability, therefore we
support the idea of a uniform tidal impedance distribution within the lungs.
Guerrero et al visualized their findings with an example of their examinations. Tidal volume
distribution in this picture correlates in distribution hierarchy with our findings of tidal
impedance distribution within the thorax. (Fig 121-122) These physiologic findings in tidal
volume and tidal impedance distribution within the lungs have to be investigated in further
studies.
r 4D-CT= Four-Dimensional Computed Tomography

147
Figure 121 This figure illustrates the 4D CT ventilation image set of a grown-up patient (coronal sections). A pair of CT images was used for each ventilation image. Each image was paired with the maximum expiration images to calculate the difference in fraction of air with respect to the maximum expiration. The images from the top row represent inspiration and the bottom row represents expiration. [From Guerrero T, Sanders K, Castillo E, Zhang Y, Bidaut L, Pan T, Komaki R (2006) Dynamic ventilation imaging from four-dimensional computed tomography. Phys. Med. Biol. 51 (2006) 777-791, retrieved May 25, 2009]
Supine Position
Spontaneously Breathing Infants
60
50
40
30
20
10
0
Tida
l Im
peda
nce
in P
erce
nt o
f TT
I
1
4
Low er RightLow er LeftUpper RightUpper Left
Figure 122 4D-CT findings of tidal ventilation compared to our four segments of the lungs at the peak of inspiration. [Modified from Guerrero T, Sanders K, Castillo E, Zhang Y, Bidaut L, Pan T, Komaki R (2006) Dynamic ventilation imaging from four-dimensional computed tomography. Phys. Med. Biol. 51 (2006) 777-791, retrieved May 25, 2009]

148
Electrode Positions in EIT versus EIS
EIT measurements place electrodes around the chest circumference to obtain cross-section
scans of the thorax; therefore a total of at least 16 electrodes is needed. According to the little
size of thoraces and the limited space for electrode placing, time course signals studied were
very noisy when applying EIT measurements to prematurely born infants7. Indeed very small
premature babies are in dire need of lung control. EIS is limited to a number of 10 electrodes
which are placed on the thorax to obtain impedance signals. We did not find any irritations of
electrode signals nor signal transmission within the electrodes during our examinations.
Thoraces have to be free of lotions or any kind of body care products to guarantee optimal
freezing of the electrodes. In EIS the placing of electrodes still has to be improved to be
applicable in daily NICU routines. (See “4.1.5 Practicability of a New Method in Neonatal
Intensive Care”).
Differences in electrode positions of EIT and EIS conclude that lung tissue assessed by these
measurements do not correlate and comparison between these methods remains challenging.
Signal Transmission of Electrodes
Electrodes didn’t show any interactions in signal transmission or signal noises. The amplitude
of tidal impedance and the height of residual impedance varied within the infants therefore
comparison in absolute numbers was not possible within all groups. While impedance is
influenced by composition of tissue, air and fluids within the thorax, 18 it has to be further
investigated if the kind of electrodes (needle electrodes, gold-disc electrodes, and self-
adhesive electrodes) placed on the thorax have an obvious effect on the impedance signal.
Petrofsky et al34 recently stated in a trial by employing both needle electrodes and surface
electrodes that the thickness of the subcutaneous fat layer was directly related to signal loss
from the skin. Therefore impedance signals recorded in extremely low birth weight infants
would differ from term babies, as their body weight is about three times lower and the
subcutaneous fat layer much thinner. Furthermore impedance signal of the skin may be
affected by body care products of the infants.
A rather interesting phenomenon has been recorded in infants when tidal impedance changes
have been extremely low. We observed a “mirrored” impedance signal mostly in the upper
right segment and lower left segment of the thorax which we’ve named “mirrored impedance

149
signal” (See “2.6.8. Mirrored Impedance Signals”). That signal occurred independently from
our electrode settings or misplacement and may have arisen and vanished within the same
examination period in one infant in both spontaneously breathing infants and infants with
assisted ventilation.
Tidal Impedance Distribution versus Residual Impedance Distribution
According to our knowledge no trial has been conducted in infants so far to compare neither
the relationship of regional tidal impedance distribution and regional residual impedance
distribution nor the regional relationship between tidal volume and functional residual
capacity of the lungs. We investigated the relationship between tidal impedance and residual
impedance within each segment and compared right to left lung and the upper lobes to the
lower lobes of the lungs while the infants were sleeping. (See “3.1.4 Relationship between
Tidal Volume and Functional Residual Capacity”) Residual impedance was detected high
when simultaneously tidal impedance was low compared to tidal impedance changes of the
other segments of the lungs. Interestingly the two right segments of the lungs and the two left
segments of the lungs in both tidal impedance and residual impedance account for around
50% each, right lung showing slightly higher data in both tidal impedance and residual
impedance of the lungs.
Frerichs et al14 conducted a trial in 12 preterm and term infants (mean 2465g, 34 weeks of
gestational age) and described tidal breathing in supine, right lateral, prone, and the infant
returned to supine position. They detected tidal ventilation of the right lungs of 54.5±8.3% in
supine position, 55.2±10.5% in right lateral position, 59.9±8.4% in prone position and
54.2±8.5% returned to supine position. Our findings of tidal impedance of the right lung in 11
spontaneously breathing infants of approximately the same age and weight was 52±9% in
supine position, 53±10% during autotransfusion, 53±10% during control period, 51±12% in
left side position and 54±10% in prone position. Our overall findings are slightly higher and
deviations are slightly wider. Still the right lung definitely displayed the higher tidal
impedance distribution in both EIT and EIS. Maybe the difference is caused by the influence
of the upper segments on our measurements, an area which is undetected by EIT as EIT
assesses lung ventilation in a plain around the chest around the 4. th or 5.th intercostal space.
Residual impedance remains hard to compare with any other method to monitor FRC as the
effects on residual impedance within the thorax are not fully disclosed yet. After observation

150
of each segment of the lungs and description of tidal impedance and residual impedance
inhomogeneties in each segment, it seems like upper and lower lobes as well as right and left
lungs leads to a nearly homogeneous distribution within the lungs in spontaneously breathing
infants.
We recorded high residual impedance changes to be mostly accompanied by low tidal
impedance changes; this is especially true in quiet infants. We observed one infant during
crying when tidal impedance of the upper right segment immediately increased enormously
when residual impedance was falling simultaneously. These findings are as well recorded
during weaning of CPAP and during extubation, a severe decrease of residual impedance is
followed by an immediate increase of tidal impedance.
Is there a Correlation between Body Weight and Residual Impedance?
Besides the conclusion that residual impedance is probably affected by more factors than
functional residual capacity, it still remains one of the most important factors to determine
residual impedance. Plenty of investigations over the years have been performed to determine
functional residual capacity (ml/kg) in infants by bodyplethysmography. An absolute value
for functional residual capacity could not be defined so far, but a decline in FRC has been
observed over the last three decades.35 We investigated residual impedance in correlation to
body weight of the infants and described a weak correlation of residual impedance increase
with body weight increase. (See “3.3.5 Total Residual Impedance Based on Body Weight”)
Body weight may affect residual impedance together with other factors, such as sleep of the
infant, crying, feeding, signal transmission of the electrodes and surface conditions of the
skin.
Is there a Correlation between Body Weight and Residual Impedance of the
Lower Left Segment?
Interestingly correlation between residual impedance of the lower left segment and body
weight was definitely higher (r= 0,71) than correlation between total residual impedance and
body weight.(r= 0,55). (See “3.3.6 Residual Impedance in the Lower Left Segment of the
151
Thorax Based on Body Weight”) Residual impedance of the lower left segment increased
with body weight of the infants. It is suggest that the size and tissue composition (fat, muscle,
and blood) of the heart effects residual impedance observed in the lower left segment as we
detected fairly high residual impedance changes in that segment with increasing body weight.
This finding has to be further investigated to clearly interpret our observations.
Effect of Body Positions on Tidal Impedance and Residual Impedance
Distribution
Body positions did not mainly affect the distribution of neither tidal impedance nor residual
impedance within the thorax. Tidal impedance distribution and residual impedance
distribution remained stable. (See “3.1.5 Summary of Spontaneously Breathing Infants” and
“3.1.4 Relationship between Tidal Volume and Functional Residual Capacity”) Lower
segments (59%) showed the highest tidal impedance distribution during prone position which
may be caused by better ventilation and respiratory synchrony39 of the infant and a more
uniform perfusion of the lungs in prone position of the infants, 40 which would lower the
impedance signal in the upper lobes simultaneously.
Effect of Feeding on Tidal Impedance and Residual Impedance
One of our preterm infants has been fed during the examinations in left side position. We
found an increase of regional tidal impedance of 32,7% in the upper left segment
simultaneously with a decrease of regional tidal impedance of the lower right segment of
48,34% in left side position during feeding the infant 20ml breast milk over a 15-20 minutes
through the NG tube. Total tidal impedance did not show any changes. At the same time we
detected an increase in regional residual impedance of 472% in the upper left segment, while
residual impedance of all other segments remained the same. (See “3.3.8 The Impact of
Feeding on Tidal Impedance and Residual Impedance”) Recent literature of the effect of
feeding on pulmonary mechanics remains limited although one study by Blondheim et al 36 in
1993 showed the following: Infants with respiratory distress syndrome receiving intermittent
feeding have been compared to infants with RDS who got continuous feeds. Our infant has
received intermittent feeds of 20ml over a 15-20minutes. In the study of Blondheim 36 they

152
observed in the infants with intermittent feeding that a decrease of tidal volume (38%), minute
ventilation (44%), and dynamic compliance (28%) occurred during feeding. On contrary
pulmonary resistance increased 100%. They suggested that intermittent feeding may lead to
airflow and pulmonary instability in very premature infants (in this study: current weight 1.2
+/- 0.3 kg; gestational age 30.5 +/- 1.1 weeks). Our infant (1905g) was not as small as the
infants in this study above and we did not detect a decrease of total tidal impedance during
feeding but an increase in the regional tidal impedance of the upper left segment and
simultaneously a decrease of regional tidal impedance in the lower left segment. These
findings have to be reproduced and further investigated. The increase of the upper left
segment’s tidal impedance may be related to the fact that the baby has been fed and the
stomach is widening according to its filling with breast milk and compressing the lungs. On
the other hand the baby was placed in left side position therefore tidal impedance changes in
the lower right segment may have been exacerbated due to weakness of premature respiratory
muscles and gravity effect. Pulmonary resistance was described to increase 100% in that trial,
we observed an increase of residual impedance of 472% in the upper left segment and as
residual impedance in all other segments of the lungs remained stable during feeding,
calculated as total residual impedance we found an increase in total residual impedance from
11059 during control period to 22260 during feeding in left side position which is an increase
of 101%.
Besides the preterm infant we studied during NG tube feeding, we examined one healthy term
infant on the maternity ward. (See “3.3.9 The Effect of Crying on Tidal Impedance and
Residual Impedance“) The 5 day-old and 3810g term boy presented with an increase of
regional tidal impedance of 19,4% in the upper left segment during feeding as well as an
increase in the lower right segment of 11,7%. Interestingly a synchronized decrease of 80,7%
regional tidal impedance has been disclosed in the upper right segment. Total tidal impedance
remained stable during feeding in left side position of a healthy term infant. The increase in
the lower right segment which was detected in the term boy but not in the preterm boy who
displayed a decrease of regional tidal impedance during feeding may be caused by the
maturity of the respiratory muscles in the healthy term boy, but further investigations remain
necessary to be able to detect any cause of this phenomenon.
Mizuno et al37 conducted a trial in which they investigated the effect of body positions in
ELBW infants before and after tube feeding. In this study tidal volume was only shown to
increase in prone position before feeding, but tidal volume did not increase in prone position

153
after feeding. According to our protocol we turned the infant from the left side (where it was
fed), to prone position and observed a decrease of tidal impedance from 168,79 during left
side position to 122,87 in prone position after feeding, which is a decrease in total tidal
impedance of 27,2%.
These are observations which causes remain unknown so far and our speculations about the
causes need further investigations. It is obvious that we may detect lung and stomach
physiology by employing EIS. We conclude that optimal positioning before and after feeding
may influence the well-being of premature infants.
Effect of Crying on Tidal Impedance and Residual Impedance
A rather interesting finding has been disclosed in a healthy term boy with a body weight of
3810g on the day of examination which was the 5th day of life for the infant. The infant was
crying after breastfeeding in left side position and kept crying for over ten minutes. (See
“3.3.9 The Effect of Crying on Tidal Impedance and Residual Impedance”) During the crying
of the infant we observed an increase of total tidal impedance of 52,34%. Increase of total
tidal impedance was generated in all four segments of the thorax, most impressively in the
upper right segment where an increase of 2394% was detected, meaning an increase from
hardly any tidal impedance changes to high tidal impedance changes caused by the crying of
the infant. Unfortunately there is hardly any literature on the effect of crying on tidal volume.
Javorka et al38 observed the lungs of 22 premature infants and found an increase of ventilation
of 255% in infants during crying compared to quiet periods. We detected a regional tidal
impedance increase of 52,34% mostly monitored in the upper right segment and lower left
segment, exactly the segments of the thorax with hardly show tidal impedance changes during
normal breathing in spontaneously breathing healthy newborns. It occurs that a reservoir of
tidal impedance (volume?) has been activated in the upper right and lower left segment of the
thorax during continuously crying of a term infant.
On contrary to tidal impedance, total residual impedance decreased during crying 15,35%.
Regional residual impedance decrease has been observed in the upper left segment (21,41%)
and the upper right segment (29,3%) while regional residual impedance of the lower segments
remained stable during crying of the infant. These observations match the findings of Javorka
et al38 who described an increase in ventilation during crying of infants.

154
Effect of Hiccups on Tidal Impedance and Residual Impedance
Continuously occurring hiccups over ten minutes have been observed in an infant with SIMV
during our investigations. (See “3.3.10 The Effect of Hiccups on Tidal Impedance and
Residual Impedance”).
Hiccups present as contractions of the diaphragm and inspiratory intercostal muscles, along
with a transient closure of the glottis.42 During the episode of hiccups we disclosed an
increase of tidal impedance mainly in the lower left segment, where tidal impedance increase
was 125%. In the three remaining segments tidal impedance increased slightly.
Hiccups can be easily detected as increasing factor of tidal impedance and has to be thought
of when detecting an inexplicable, immediate increase of tidal impedance in an infant.
Residual impedance has not been affected by hiccups during our examination.
Different Breathing Pattern
EIS was shown to reliably detect different breathing pattern in infants. (See “2.5.4 Breathing
Pattern” and “3.3.7 Different Breathing Pattern in Infants”). Periodic breathing and apnea
occur in premature infants and are treated successfully with theophylline on a daily basis in
NICUs.41 EIS could further serve as an apnea monitor while recording regional tidal
impedance changes and regional residual impedance changes of the lungs by detecting apneic
and/or periodic breathing pattern.
Interestingly periodic breathing has been observed in two healthy term infants in this study.
Cardiovascular Changes Observed by EIS
Cardiovascular changes may be seen in EIS measurements especially during apneic episodes
(See “2.5.4 Breathing Pattern”) of the infants. We observed cardiovascular impedance
changes, which need to be investigated in the future to test their relevance in EIS monitoring.

155
Can We Detect Misplaced Electrodes?
During our investigation electrode position of one infant has been switched to test the effect
of this manoeuvre on our measurements. (See “3.3.3 Effect of Incorrectly Placed Electrodes
on the Results”) Total tidal impedance decreased 67,71% during the switching of the
electrodes, simultaneously total residual impedance increased 39,76% by changing the
electrode position. This may be explained by the increased diameter within the measuring
electrodes which is assessed by EIS when electrode position is changed. These findings match
with our observations that tidal impedance has a tendency to decrease with increasing body
weight (as the chest circumference increases with body weight and therefore the diameter to
disclose by EIS gets longer), and residual impedance increases with increasing body weight as
the lung and cardiac tissue to discover within the thorax becomes larger with increasing size
of the infant.
Electrodes which are misplaced or switched during measurements may be easily detected.
More likely is the misplacement of electrodes before the start of the measurements, which can
not be discovered so far according to lack of reference data and experience. Developing of an
electrode vest/onesie where misplacement of electrodes is simply avoided is recommended.

156
4.1.2 Infants with Assisted Ventilation
In our study we enclosed 4 infants with mean (±SD) gestational age of 33,75 (±5,56) weeks
and a mean body weight of 2430g (±777) on the day of examination, receiving assisted
ventilation: Three infants required SIMV with PEEP 4.5cm H2O and one infant was on CPAP
with PEEP 4.5cm H2O. The three infants on SIMV have been ventilated due to birth asphyxia,
post shunt-op due to a hydrocephalus, and due to a pneumothorax. The infant on CPAP
presented with respiratory distress syndrome. The underlying causes for ventilation
differencies within our study group, the findings in regional tidal impedance distribution and
regional residual impedance distribution varied within these infants.
Positive end-expiratory pressure – which has been increased and decreased in this study group
(See “2.4.8 The Course of Examination”) – is known to prevent alveolar collapse, to maintain
lung volume (FRC), and to improve the ventilation-perfusion relationship. PEEP effects tidal
volume and with increasing PEEP decreasing VT is expected. The use of high PEEP (>6cm
H2O) may decrease lung compliance, could impair venous return, decrease cardiac output, and
decrease oxygen transport.43 Appropriate ventilator settings have to be made for every single
infant individually as PEEP requirements are different for every infant on assisted ventilation
due to the different degree of pulmonary disease.44
EIS could help to monitor tidal volume settings of the respirator and to observe the affect of
respiratory parameters on FRC. Tidal impedance and residual impedance have been studied in
four infants at various PEEP level.
Tidal Impedance and Residual Impedance in Infants with Assisted Ventilation
Tidal impedance changes have been studied during alternation of PEEP level in three infants
on SIMV. We started with a PEEP of 4.5cm H2O, decreased PEEP to 3.5cm H2O, increased
PEEP to 5.5cm H2O, and decreased PEEP back to 4.5cm H2O. Tidal impedance has been
described to correlate with tidal volume (r2= 0,98; p<0.01, Pearson Correlation) in a former
animal experiment in which EIS has been employed.3 In this study a decrease of tidal
impedance has been detected by an increase of PEEP level. During our investigations only a
decrease of 1cm H2O and an increase of 1 cm H2O according to baseline at 4.5cm H2O have
been performed.

157
Infant I: 2100g – The Extubation of an Infant
A male Caucasian infant ventilated due to a shunt operation has been studied and tidal
impedance has been observed during PEEP alternations. At the end of the examination period
the infant has been extubated and this manoeuvre was successfully recorded by EIS. Tidal
impedance showed an interesting result when a decrease of PEEP has been conducted. We
observed a decrease of tidal impedance in the upper left segment which remained low through
the whole examination period. In the lower left segment a decrease of tidal impedance has
been monitored on contrary to the right lung, where an increase in both upper right segment
and lower right segment was detected. Total tidal impedance decreased from 136,2 during
PEEP 4.5cm H2O to 113,93 during PEEP 3.5cm H2O. The decrease was mostly determined
by the upper left segment. We further increased PEEP to 5.5cm H2O and three (UR, LL, LR)
of four segments showed a decrease in tidal impedance, indeed tidal impedance increase of
the upper left segment was fairly low from 1,68 to 1,77 during PEEP 5.5cm H2O. Total tidal
impedance was lowest during that examination period with 87,17 and a PEEP of 5.5cm H2O.
By decreasing PEEP back to 4.5cm H2O an increase in total tidal impedance to 103,96 has
been observed, and increase occurred in all four segments of the thorax. It has to be further
investigated if such a fall in tidal impedance is caused by quality and conductance of self-
adhesive electrodes or if tidal impedance mainly disappeared during the decrease of PEEP.
Most impressive was an increase of tidal impedance of 138% when the infant started to breath
spontaneously, and even tidal impedance of the upper left segment increased immediately.
We observed high tidal impedance changes in the upper left segment of the lungs during
spontaneous breathing in infants. Simultaneously a decrease of residual impedance of the
upper left segment has been observed. Our infant was free of respiratory disease but
mechanical ventilation showed to distribute tidal impedance differently from spontaneous
breaths. The observation that tidal impedance immediately increased during spontaneous
breathing weaken the idea of the decreasing signal conductivity of the electrodes.
Residual impedance decreased simultaneously during weaning manoeuvre and is described in
detail in “4.1.4 Residual Impedance as Surrogate for Residual Functional Capacity?”

158
Infant II: 2910g – Suction of an Infant with a Pneumthorax
We investigated an infant admitted to the NICU due to a pneumothorax of the left lung and
ventilated with SIMV at PEEP 4.5cm H2O. Rather interestingly tidal impedance in all four
segments decreased enormously when PEEP was reduced to 3.5cm H2O and then remained
relatively stable, tidal impedance was little increased by suction during PEEP 5.5cm H2O but
not alternating PEEP level. Simultaneously to this observation in tidal impedance decrease at
PEEP 3.5cm H2O a change in breathing pattern has been observed which remained changed
throughout the rest of the examination. (See “3.3.7 Different Breathing Pattern in Infants”)
There are trials to demonstrate the benefits of HFPPV and triggered ventilation compared to
conventional mechanical ventilation in neonates to prevent or at least reduce the risk of air
leak syndromes51, more detailed studies about the effect of PEEP in pneumothorax itself once
it occurred, remains unknown.
This infant has been suctioned twice, primarily at a PEEP level of 5.5cm H2O and secondly
when PEEP was set 4.5cm H2O. There was a slight increase in residual impedance by suction
of the lungs in the upper right segment and lower left segment of the lungs. Simultaneously
upper left segment and lower right segment residual impedance decreased and total residual
impedance nearly remained stable by suction of the lungs.
Morrow et al52 searched through 118 trials from 1962 to 2007 to find evidence data of the
positive effect of suctioning of the lungs. They concluded that there is no clear data to show a
positive, profitable effect for the patients (infants, children, and grown-ups), but suctioning
may cause a range of potentially serious complications.
Infant III: 3210g – How Do Narcotic and Analgetic Drugs Affect Functional Residual Capacity?
Four infants with assisted ventilation have been studied in this trial; in two of these four
infants (See “Infant 2100g” and “Infant 3210g”) a continuous decrease of residual impedance
has been observed during this investigation. None of the spontaneously breathing infants
displayed these findings nor the infant on CPAP or the other infant on SIMV. In a former
study in which residual impedance has been investigated by employing EIS, a continuous
decrease of residual impedance was described in six ventilated and narcotized piglets. 45 In this
former trial residual impedance of piglets has been observed during various PEEP level
(PEEP 4cm H2O – PEEP 2cm H2O – PEEP 4cm H2O – PEEP 6cm H2O – PEEP 8cm H2O and

159
PEEP 4cm H2O). Löb45 showed a continuous decrease of residual impedance over time during
their experiment. PEEP is known to increase FRC29 of the lungs and therefore an increase in
residual impedance - as an increase of lung volume (= air) occurs - would be expected to be
detected by EIS. Löb described a continuous decrease in residual impedance independently of
PEEP increase or decrease manoeuvre. We observed this characteristic in residual impedance
in two of our infants.
What is the difference of the two ventilated infants with the continuous decrease compared to
the two ventilated infants without the continuous decrease? And why do spontaneously
breathing infants not display these finding? One explanation could be that residual impedance
signal is inversely displayed to functional residual volume or increase in air volume. In this
case we would have to detect a continuous decrease in all infants and narcotized piglets as
well as ventilated infants would have a continuous increase in functional residual capacity
over time.
The amplifier of the EIS device may affect impedance signal in several ways, but as our
findings are only shown in a few infants and the piglets, it is unlikely to be caused by the
amplifier. The same is true for the effect of PEEP/CPAP on newborn lungs as we found the
continuous decrease only in two out of four infants.
What do two infants admitted to a NICU have in common with six narcotized piglets in an
animal experiment?
Infant I (2100g) and Infant III (3210g) were admitted to NICU 1.) due to a shunt-operation in
a hydrocephalus (first post-operative day) and 2.) due to birth asphyxia in a term baby. Drugs
may have an effect on functional residual capacity of the lungs.
Löb45 administered the following narcotics during her trial to anesthetize the piglets:
ü Ketamin (10mg/kg)
ü Fentanyl (5µg/kg)s
ü Propofol (1mg/kg)t
ü Phenobarbital (20mg/kg)
ü [Ampicillin (200mg/kg)]
Anaesthesia was maintained by
ü Phenobarbital (20mg/kg/h)
ü Fentanyl (10 µg/kg/h)
ü [Ringerlactat 40ml + Glucose (33%) 10ml (6ml/kg/h)
sDoes effect FRC tDoes effect FRC
160
Muscle relaxation was achieved by application of
ü Rocuronium (1mg/kg/h)u
Unfortunately we didn’t make any notes of the infants’ medications during our investigations,
but both a post-op infant and an infant with birth asphyxia are favourable candidates for one
of the following drugs46 which may be given in both cases:
Analgetic drugs: Opiate
ü Tramal (0,25mg/kg/h)
ü Vendal (10-30μg/kg/h)
ü Fentanyl (1-5μg/kg/h)
ü Sufentanil (0,5-5μg/kg/h)
Sedation: Benzodiazepine
ü Dormicum (0,06mg/kg/h)v
Relaxants: Vecuronium
ü Norcuron (0,05mg/kg/h)
Propofol47, Rocuronium30, Fentanyl48, and Midazolam49 were shown to decrease FRC of the
lungs. There was no data available about the effect of phenobarbital on functional residual
capacity. Von Ungern-Sternberg et al47 described a highly significant decrease of FRC in the
lungs of school children free of any cardio-respiratory disease undergoing surgery when
anesthesia was induced with propofol 120mg/kg/min followed by a bolus of propofol 1mg/kg,
furthermore a propofol infusion at 240 mg/kg/min was given.
Cox et al30 investigated anesthetized infants undergoing clubfoot surgery who received
rocuronium 1mg/kg and detected that static compliance and dynamic compliance decreased
significantly when they placed the infants in prone position compared to supine position.
Chawla et al48 administered fentanyl 0.5µg/kg in nine women undergoing minor
gynaecological procedures and found a significant decrease in FRC of their patients’ lungs.
They suggested an increased activity of expiratory muscles and an increase in intra-abdominal
pressure as possible cause for their findings.
Midazolam as premedication before surgery has been described to affect FRC in children by
von Ungern-Sternberg et al.49 In their study 0.3mg/kg midazolam were given in 21 children at
the age 3-8yrs. FRC has been determined by sulphur-hexal-fluoride multiple breath washout
and a significant decrease in FRC (-6.5%) and VT (-3%) has been observed.
u Does effect FRC v Does effect FRC

161
According to the literature available about the effect of anagetic drugs and our observations
during our measurements, compared to the animal experiment of Löb45, we suggest that
analgetic drugs may decrease residual impedance and therefore decrease FRC of the lungs in
infants. The continuous decrease of residual impedance in two of our infants and in the study
of Löb45 may have been caused by medications and their effect on FRC may have been higher
than the effect of increasing PEEP. In the animal experiment the dose of fentanyl applied was
10-times higher than in the study of Chawla et al.48
Löb45 explained these findings by a possible edema of the lungs caused by increasing PEEP
level. According to the observations in our trial and the effect of analgetic drugs (the piglets
received 3 drugs which are known to decrease FRC), the influence of these medications in
reducing FRC is much more likely than developing an edema from PEEP alternations.
These findings need to be further studied by EIS and furthermore EIS may be a reliable tool to
monitor FRC decrease in patients with analgetic therapy.
The Infant on CPAP with 1500g
We studied one infant with 1500g presenting with respiratory distress syndrome on CPAP
(4.5cm H2O) and during weaning from CPAP breathing spontaneously. A decrease of 30% of
total residual impedance (See “3.2 Infants with Assisted Ventilation”) and a simultaneous
increase of tidal impedance of 91% have been disclosed. These findings were most impressive
in the upper left segment. According to our findings in spontaneously breathing infants and
infants with assisted ventilation residual impedance of the upper left segment was higher in
infants with assisted ventilation than in infants breathing spontaneously and decreased
enormously in both infants who have been weaned of ventilation. (See “3.2.5 Tidal
Impedance and Residual Impedance Before and After Extubation/ Weaning of CPAP”)
Why do infants with assisted ventilation show higher residual impedance in the upper left
segment of the lungs and why does this residual impedance suddenly decrease during weaning
from ventilation? In grown-ups a PEEP of ≥10cm H2O is known to increase the areas of the
lungs where ventilation is physiologically higher than perfusion, namely the upper parts in an
upright position, findings which were well described by West. 50 During mechanical
ventilation and a PEEP high enough further distension of these areas may occur. A PEEP of
4.5cm H2O in an infant is unlikely to cause this phenomenon, still literature about this

162
observation is lacking. Anatomy of the trachea, lungs and heart may have an impact on the
residual impedance distribution within the lungs and need to be further observed by
employing EIS.
163
4.1.3 Tidal Impedance as Surrogate for Tidal Volume?
Löb45 tested the correlation between tidal impedance and tidal volume and described a
correlation of r2= 0,98 (p<0.01, Pearson Correlation) for EIS measurements. These findings
have been taken into account in the underlying work. It may kept in mind that the heart affects
tidal impedance signal by first increasing tidal impedance signal slightly and further through
opening the aortic/pulmonary valves during heart cycle and consecutive blood flow through
the aorta decreasing impedance signal.18 Though this effect of the heart on tidal impedance is
very little. Filters may be used to suppress this phenomenon during measurements, in the
underlying study only raw data has been analyzed.
The effect of body weight, feeding, crying, body position, and misplaced electrodes on tidal
impedance has been well described above. (See “4.1.1 Spontaneously Breathing Infants”)
Tidal impedance might act as a reliable surrogate for tidal volume as described by Löb in a
former animal experiment employing EIS.45

164
4.1.4 Residual Impedance as Surrogate for Functional Residual Capacity? Functional residual capacity (FRC) is the lung volume which remains within the lungs after
expiration and may be used as a parameter for alveolar gas exchange within the lungs.25 One
of the aims of EIS is to regionally detect residual impedance changes and to observe the
development of lung disease which presents either with an increase or decrease in functional
residual capacity. FRC can be determined by washout techniques21, which are labour-
intensive and cannot monitor lungs continuously at beside. FRC needs to be determined to
adjust ventilator settings properly to the infants’ needs and to adequately detect the
development of lung disease. EIS does not only determine total residual impedance but
records regional residual impedance changes within four segments of the thorax.
We investigated the regional and total residual impedance of eleven spontaneously breathing
infants with a mean (±SD) body weight of 2659 (±903g) and a gestational age of 35 (±4)
weeks on the day of examination. Additionally residual impedance of four infants with
assisted ventilation and a mean (±SD) body weight of 2430g (±777) and a mean gestational
age of 33,75 (±5,56) weeks has been studied. A clear tendency in residual impedance
distribution was described for the spontaneously breathing infants group (See “3.1.5 Summary
of Spontaneously Breathing Infants”) showing the following order in residual impedance
distribution within the thorax starting with the highest:
Upper right segment – Lower left segment – Lower right segment – Upper left segment. Data
about functional residual capacity in “healthy” (without any signs of lung disease) preterm
and healthy term newborns is very limited. The distribution of residual impedance we have
found in our investigations is unlikely to be only determined by air distribution within the
lungs but affected by all dynamic changes within the thorax.
FRC itself is determined by multiple factors inside the lungs such as maturation of the lungs in
preterm infants at the time of birth, surfactant production and antenatal steroid application
before preterm labour.26 Furthermore prematurely born infants with chronic lung disease
showed lower FRC values than a healthy control group.27 Factors outside the lungs but within
the thorax may have an impact on FRC: Flow and volume delivery decrease if the patient’s
respiratory drive and respiratory muscle strength are weak.28 Resistance and compliance
majorly affect FRC of the lungs.25 During mechanical ventilation PEEP increases FRC in the
lungs at birth by improving liquid clearance and aeration of the distal airways and furthermore
preventing airway collapse at end-expiration.29 Medications such as muscle relaxants (e.g.

165
rocuronium) may decrease FRC during sedation of an infant25 and the extent of decrease in
FRC may be influenced by body position of the infant during muscle relaxation.30
FRC is not the only parameter responsible for optimal gas exchange and oxygenation of the
lungs even if it is suggested as an indicator for alveolar gas exchange of the lungs. Optimal
ventilation, optimal perfusion and optimal diffusion of the lungs determine gas exchange and
oxygenation of the lungs.25
In a former animal experiment with the EIS device1,3 residual impedance has been suggested
as surrogate for FRC. Residual impedance is definitely an important parameter to be
evaluated by EIS and may provide powerful information about thoracic dynamic changes.
Still it should not be used as a surrogate for functional residual impedance, primarily because
functional residual impedance (and functional residual capacity) is determined by multiple
factors as described above and therefore definition of residual impedance in absolute numbers
to find a value to rely or orientate on may be hard to define. From our observations we
suggest that residual impedance changes detected by EIS are a good parameter to regionally
monitor the lungs additionally to the observation of vital signs of the infant, signs of
respiratory disease and other respiratory parameters which are provided by ventilator settings.
Detection of changes in intrathoracic dynamics [i.e. 1) ventilation in the means of FRC and
tidal volume decrease/increase, 2.) fluids increase in the means of an edema and 3.) others]
might be easier to early detect by observing residual impedance by EIS at bedside. Residual
impedance should be a surrogate for intrathoracic dynamic changes. In an animal experiment
the development of a pneumothorax was recorded and an increase of residual impedance has
been described.45 Pneumothorax means collapse of lung tissue and air gets trapped within the
pleural space, electrical impedance segmentography would clearly detect an increase in
residual impedance during the development of this pneumothorax. Precisely defined the
increase of residual impedance in a pneumothorax is caused by air in the pleural space and not
by an increase of functional residual capacity of the lungs. Therefore we suggest abandoning
from using residual impedance as the surrogate of FRC. Regardless of this exact definition
electrical impedance segmentography was able to detect an increase in residual impedance in
a piglet with a pneumothorax in which an increase of air within the thorax arises45. These
findings could be well used in early diagnosis of a pneumothorax.
Residual impedance has been observed in all 15 infants of this study. In our assisted
ventilation group we recorded residual impedance changes during weaning of CPAP, in a
second infant we monitored residual impedance changes during extubation from SIMV.

166
The infant on CPAP was a Caucasian boy born prematurely at 30 weeks of gestational age,
presented with 1500g on the day of examination and has been treated with CPAP due to
respiratory distress syndrome. (See “3.2. Infants with Assisted Ventilation” and “3.2.2 The
Infant with CPAP”) This boy showed a decrease of total residual impedance within the thorax
from 35707 in prone position on CPAP 4.5cm H 2O to a total residual impedance of 24810
during spontaneously breathing in prone position which displays an overall residual
impedance decrease of 30% through weaning of CPAP. EIS clearly detected a fall of residual
impedance during weaning which most probably is related to an alveolar derecruitement. 28
Unfortunately literature of FRC characteristics during weaning of CPAP/PEEP remains
limited until today. Heinze et al28 described a decrease of FRC from BiPAP 10cm H2O to
CPAP 7cm H2O in seven healthy grown-ups after cardiac surgery during weaning maneuver
tested by oxygen washout technique. (LUFU System, Dräger Medical, Lübeck, Germany).
Observed was a decrease of FRC from 3,6l during BiPAP to 2,7l during CPAP which is a
decrease in FRC of 25%.
The second male Caucasian infant free of respiratory disease - in whom extubation has been
monitored - was admitted to the NICU at 28 weeks of gestational age and has been assigned
to our study group at 36 weeks of corrected age with a current body weight of 2100g being
ventilated after a shunt operation due to a hydrocephalus. Extubation was performed at the
end of our examination period, therefore we unfortunately could only use two minutes of data
after extubation for analysis. During that period we found a decrease in total residual
impedance of nearly 10% from 21501 during SIMV at PEEP 4.5cm H2O to 19351 during
consecutive spontaneously breathing of this infant. Further characteristics of residual
impedance changes of the lungs in this infant in the following hours after extubation remain
unknown.
In both infants the most impressive decrease of residual impedance was observed in the upper
left segment of the thorax where a high decrease of 33% in the CPAP infant and 42% in the
SIMV infant was shown while simultaneously total tidal impedance and regional tidal
impedance of the upper left segment significantly increased. (See “3.2 Infants with Assisted
Ventilation” and “3.2.5 Tidal Impedance and Residual Impedance Before and After
Extubation/ Weaning of CPAP”)
Residual impedance detects dynamic changes within the thorax which may provide an easier
and quicker diagnose during the development of lung disease, identification of harmful
ventilation, and detecting misplaced tubes and the optimal moment for extubation. ´

167
4.1.5 Practicability of a New Method in Neonatal Intensive Care
Practicability of the EIS device is of major interest if the method should be applied in a daily
routine, starting it most probably during an admission to the NICU when time is limited. The
EIS device itself is a small machine which could be easily placed in NICUs next to the
infant’s incubator/bed.
Electrode placing has to be improved to quicker provide the observation of the lungs in an
emergency. In this pilot investigation electrodes have been placed carefully and properly to
the infants’ thoraces. Self-adhesive electrodes (Blue Sensor, BRS-50-k, Ambu®, Denmark)
have been used during our trial. Each electrode out of a total of 10 electrodes had to be put
separately on the infant’s thorax. Symmetry in distance between the electrodes and correct
positioning is essential for comparing results. Furthermore electrodes can get misplaced easily
in a stressful situation and would affect our outcome measures. (See “3.3.3 Effect of
Incorrectly Placed Electrodes on the Results”). Efforts need to be made to find an optimal
solution to avoid electrode misplacement and provide quick and correct positioning. The
development of an electrode vest has been suggested and as enhance to that idea the
development of an electrode onesie has been described above. (See “2.4.6 Electrode Vest”,
and “2.4.7 Electrode Onesie – A Future Concept?”)

168
4.2 The Role of Lung Anatomy and Lung Physiology in EIS
Measurements
4.2.1 Is EIS a New Method to Study Lung Function?
Primarily there is a dire need in neonatal intensive care medicine to develop a method to
monitor lung function of newborn infants to apply less harmful ventilation.21 Knowledge
about physiological lung function in infants is still little and further investigations have to be
made. EIS is a reliable method to monitor lungs in spontaneously breathing infants and infants
with assisted ventilation, and the findings of this investigation have to be further tested. A
decision should be made about the definite field of application of EIS. We employed EIS in
both spontaneously breathing infants and infants with assisted ventilation in our pilot trial, to
test whether we can describe tidal impedance changes and residual impedance changes in
both. A reasonable field of application has to be found and further investigations should be
conducted in that area.
4.2.2 Control of Lung Physiology of every Infant Admitted to the NICU or
Simply Control of Lung Pathophysiology under Mechanical Ventilation?
Which technical skills should EIS include? Should EIS be a monitoring tool of every infant
admitted to the NICU to early detect the development of respiratory disease or simply monitor
infants on ventilators at bedside?
We suggest the development of a device to monitor every infant at risk for developing lung
disease of any origin both spontaneously breathing infants and infants with assisted
ventilation. Primarily to early detect the onset of disease and to intervene early enough to
provide adequate treatment. Monitoring of infants with respiratory disease is required in
NICUs to provide the least harmful ventilation; infants’ needs may not only vary within
individuals but in the same infant over time according to the actual stage of their respiratory
disease.
So far EIS is able to monitor the following parameters: Tidal volume, dynamic changes of the
thorax (mostly caused by changes in FRC), EKG, SaO2, breathing pattern of the infant, flow

169
and pressure from the respirator if ventilated, which may additionally provide information
about lung compliance.
Anatomy of the lungs, trachea and heart may influence the distribution of functional residual
capacity within the lungs as well as the distribution of tidal volume. EIS would further be a
reliable tool to study these parameters in lungs of healthy infants to gain knowledge about
lung function.
4.2.3 What is Homogeneous Ventilation?
Homogeneous ventilation is a widely used term but hardly uniformly defined and mostly used
within a given context. Several factors have an impact on “homogeneous ventilation”. An
optimal ventilation/perfusion distribution is inevitable between gas exchange of the alveoli
and blood circulation of the lungs.50 Compliance and resistance of the lungs further determine
optimal function of the lungs and various methods have been developed over the last decades
to obtain information about lung mechanics. 53 Surfactant is a major factor for adequate lung
maturation.26
Exogenous factors such as ventilation affect lung mechanics and lead to changes in lung
volumes and further affect lung perfusion.50 The effect of analgetic and sedative drugs on
static lung volumes has been recently described by anaesthesiologists.30, 47-49
Most importantly respiratory diseases alter lung function to a major extent and 75% of all
neonatal deaths are found in premature infants, mostly suffering from respiratory diseases.54

170
4.3 Advantages and Limitations of EIS
EIS is shown to have several advantages in neonatal intensive care. Primarily its applicability
as beside monitoring during the entire stay of an infant in the NICU. Furthermore it is a
radiation-free, low cost, non-invasive monitoring tool to assess information about tidal
volume of the lung and dynamic changes (i.e. fluid and air) within the thorax. EKG, SaO2,
and breathing pattern may be obtained simultaneously when applying EIS. In ventilated
infants information about lung compliance can be achieved.
Limitations are instantly in the time consuming application of the electrodes which has to be
improved in the future. EIS assesses tidal impedance changes and residual impedance changes
of four segments of the thorax but is unable to differentiate between dependent and
independent lung segments.
171
4.4 Conclusion
Electrical impedance segmentography is a reliable method to continuously monitor tidal
impedance changes and residual impedance changes within the thorax of infants at beside.
Both parameters have to be further investigated to clearly establish their informative value as
well as their validity which is especially true for residual impedance changes. Tidal
impedance distribution and residual impedance distribution showed to be uniform within each
infant even impedance signals displayed a clear tendency of distribution in both tidal
impedance changes and residual impedance changes.
Furthermore the purpose of clinical use of the EIS device has to be more defined in detail. EIS
would be a good method for long-term monitoring of newborn lungs at the bedside as it is a
low cost, non-invasive, non-radiate monitoring tool and could help to detect changes in both
tidal impedance distribution and residual impedance distribution within the thorax. There is
still a dire need to investigate these parameters as dynamic changes within the thorax
constitute from multiple factors and severely influence our impedance measurements and the
observed results. A good understanding of the results is indispensable for applying EIS in
daily care in the NICU.
Practicability of electrode placing has to be improved to quickly but properly apply electrodes
to infants’ thoraces in an emergency situation which routinely occurs in neonatal intensive
care. EIS could be a good method to adjust optimal ventilator settings to the infants’ needs at
beside in NICUs and closely monitor and readjust these settings.
Furthermore EIS could function routinely as a monitoring tool for even detecting the
development of lung disease, misplaced tubes, and observation of extubation manoeuvres and
as a consequence avoiding reintubation.
Another advantage of EIS would be the gain of information about physiologic air distribution
within newborns’ lungs to better understand and monitor development of lung disease in
prematurely born infants, but it should be kept in mind that the nicest tool used incorrectly can
be dangerous for the infants. It still has to be tested if our EIS measurements and its findings
can be reproduced.

172
Summary BACKGROUND: In this pilot investigation electrical impedance segmentography was shown
to be a reliable method to monitor regional tidal volume of newborns’ lungs as well as
regional dynamic changes within four segments of the thorax (i.e. air, fluids), latter mostly
determined by functional residual capacity. Eleven spontaneously breathing infants with a
mean gestational age (±SD) of 35 (±4) weeks and a mean body weight of (±SD) of 2659g
(±903) and four infants with assisted ventilation (3 SIMV, PEEP 4.5cm H2O and 1 CPAP,
PEEP 4.5cm H2O) at a mean gestational age of 33, 75 (±5,56) weeks and a mean body weight
of 2430 g (±777) have been elicited in this trial.
RESULTS: Tidal volume changes reflected by tidal impedance changes in four segments of
the thorax (upper left segment, upper right segment, lower left segment and lower right
segment) in spontaneously breathing infants showed a similar distribution of tidal volume
within the thoraces of the spontaneously breathing infants. Highest tidal volume changes have
been found in the lower right segment which were significantly higher than tidal volume
changes in the upper right segment and the lower left segment (p<0.0001). No significance in
tidal volume changes could be shown between the lower right segment and the upper left
segment.(p=0,157)
Residual impedance reflects dynamic changes of the thorax mostly affected by functional
residual capacity. Findings of residual impedance were inversely to tidal impedance changes,
meaning in segments with high residual impedance changes low tidal impedance changes
were found and vice versa. Residual impedance of the upper right segment was significantly
higher than residual impedance of the lower right segment and residual impedance of the
upper left segment (p<0.05), while residual impedance changes of the lower left segment
were about the same value (p=0,86). In the four infants with assisted ventilation no significant
differences in tidal impedance or residual impedance changes could be found and more
homogenous ventilation is suggested.
Effect of positioning (supine position, left lateral position, and prone position,
“autotransfusion” and in several infants the effect of feeding and crying on tidal impedance
distribution and residual impedance distribution has been investigated. The above described
findings in tidal and residual impedance distributions remained stable during positioning, but
were influenced by feeding and crying of the infant.
In the assisted ventilation infants group the effect of PEEP alternations (PEEP decrease 1cm
H2O followed by PEEP increase 2cm H2O) on tidal and residual impedance has been studied.

173
PEEP alternations did not show any change (decrease/increase) in residual impedance, which
may be caused by the fairly small alternations of PEEP. Furthermore we observed a
continuous decrease of residual impedance in two of the four infants with assisted ventilation.
(Even by increasing PEEP which should be increasing FRC) Therefore a closer investigation
of the effects of analgetic and sedative drugs on FRC in newborns monitored by EIS
compared to a control group is suggested as we may have recorded a continuous fall in FRC
caused by analgetic drugs in these infants which may mask (and actually reduce!) the effect of
PEEP alternations.
CONCLUSION: Electrical impedance segmentography (EIS) is a reliable method to monitor
regional tidal volume and regional dynamic changes (FRC) of the lungs of infants at bedside
in the NICU. The limited number of ten electrodes (Blue Sensor BRS-50-k, Ambu®,
Denmark) to monitor the lungs is a major advantage of this method and may be applied in
extremely small infants, those who are in dire need of continuous lung control at bedside.
Further studies to show the reproducibility of these findings are needed.
174
Zusammenfassung HINTERGRUND: Eletrical Impedance Segmentography (EIS) wurde im Rahmen
vorliegender Pilotstudie in die neonatologische Intensivmedizin eingeführt und als eine für die
Zukunft viel versprechende Meßmethode der Lungen Neugeborener erstmals beschrieben.
Tidalvolumen und dynamische Veränderungen innerhalb des Thorax (i.e
Luftvolumensänderungen, Flüssigkeitsverschiebungen), letztere hauptsächlich durch das
Residualvolumen der Lunge beeinflusst, können mittels elektrischer Impedanzmessung
überwacht werden. Untersucht wurden 11 spontan atmende, reife und unreife Neugeborene in
der 35. (±4) Schwangerschaftswoche (SSW) mit einem aktuellen Körpergewicht von 2659
(±903)g. Des Weiteren wurden vier Kinder mit assistierter Beatmung (3 SIMV, PEEP 4.5cm
H2O und 1 CPAP, 4.5cm H2O) in der 33, 75 (±5,56) SSW und einem aktuellen
Körpergewicht von 2430 (±777)g untersucht.
ERGEBNISSE: Änderungen des Tidalvolumens der Lunge - ermittelt durch die
Tidalimpedanz - wurden in vier Segmenten der Lunge vermessen (namentlich: upper left
segment, upper right segment, lower left segment und lower right segment).
In der Gruppe der spontan atmenden Kinder konnte eine einheitliche Verteilung des
Tidalvolumes innerhalb der Kinder aufgezeigt werden. So befanden sich die höchsten
Tidalvolumina im unteren, rechten Segment der Lungen, welche auch signifikant größer
waren als die Tidalvolumina des oberen, rechten Segmentes als auch des unteren, linken
Segmentes der Lungen (p<0.0001). Zwischen dem oberen, linken Segment und dem unteren,
rechten Segment konnten keine großen Unterschiede des Tidalvolumen dargestellt
werden.(p=0,157)
Die Residualimpedanz stellt dynamische Veränderungen des Thorax dar, welche maßgeblich
von den Änderungen der funktionellen Residualkapazität (FRC) bestimmt werden. Die
Ergebnisse der Residualimpedanz waren spiegelbildlich zu denen der Tidalimpedanz bezogen
auf die einzelnen Segmente. Segmente mit großen Tidalvolumensänderungen zeigten
minimale Änderungen der Residualimpedanz und umgekehrt. Die Residualimpedanz des
oberen, rechten Segmentes war signifikant größer als die Residualimpedanz des unteren
rechten Segmentes und des oberen, linken Segmentes. (p<0.05). Keine Unterschiede konnten
in der Residualimpedanz zwischen dem oberen, rechten Segment und dem unteren, linken
Segment gemessen werden.(p=0,86)

175
In der Gruppe der beatmeten Neugeborenen konnte diese charakteristische Verteilung weder
der Tidalimpedanz noch der Residualimpedanz aufgezeigt werden und eine homogene
Verteilung der Lungenvolumnia durch die Beatmung muss in Betracht gezogen werden.
Die Lageänderung (Rückenlage, Linksseitenlage und Bauchlage), Durchführung der
„Autotransfusion“ und bei einigen Kindern die Vermessung von Füttern und Schreien des
Babys und die Untersuchung des Effektes dieser Vorgänge sowohl auf das Tidalimpedanz als
auch auf die Residualimpedanz wurden studiert. Die bereits oben beschriebenen Verteilungen
der Tidalimpedanz und Residualimpedanz innerhalb der Lungen wurden durch die
Lageänderung des Neugeborenen nicht beeinflusst. Beim Schreien und Füttern des Kindes
konnte durchaus eine regionale Veränderung dieser beiden Parameter aufgezeigt werden.
In der Gruppe der beatmeten Kinder wurden die Veränderungen des PEEP Levels auf die
Lungenvolumina studiert. (Erniedrigung des PEEP um 1cm H2O gefolgt von einer Erhöhung
des PEEP Levels um 2cm H2O). Durch Verstellen des PEEP Levels konnten weder eine Zu-,
noch Abnahme des PEEP Levels festgestellt werden. Dennoch wurde ein kontinuierliches
Sinken der Residualimpedanz in zwei der vier Neugeborenen mit assistierter Beatmung
beobachtet.(Bei der Erhöhung des PEEP Levels würden wir nach aktuellem Kenntnisstand
eine Erhöhung der FRC erwarten) Eine weitere Untersuchung mittels elektrischer
Impedanzmessung von Neugeborenen auf Intensivstationen unter Analgetika,- und/oder
Sedativabehandlung im Vergleich zu einer Kontrollgruppe wird vorgeschlagen, nachdem der
kontinuierliche Abfall der Residualimpedanz in unseren Messungen durch die Verabreichung
von Analgetika und Sedativa bedingt sein könnte, welche den Anstieg der Residualimpedanz
durch die PEEP Erhöhung verschleiern bzw auch antagonisieren können.
CONCLUSIO: Die Electrical Impedance Segmentography (EIS) ist eine geeignete Methode
um Tidalvolumen und dynamische Veränderungen des Thorax (FRC) kontinuierlich auf
Neugeborenen-Intensivstationen zu überwachen. Die auf nur zehn Elektroden (Blue Sensor,
BRS-50-k, Ambu®, Denmark) reduzierte Anzahl der Elektroden während der Messung macht
diese vor allem im Einsatz bei sehr kleinen Neu,- und Frühgeborenen besonders attraktiv.
Gerade diese Gruppe Frühgeborener würde ein kontinuierliches Monitoring ihrer Lungen
benötigen. In weiteren Studien muss die Reproduzierbarkeit der Ergebnisse dargestellt
werden.

176
Abbreviations ADC Analogue-to-Digital Converter BP Blood Pressure CE Conformité Européenne ch Channel of EIS measuring device CHF Congestive Heart Failure CMV Controlled Mandatory Ventilation CPAP Continuous Positive Airway Pressure CT Computed Tomography dB Decibel EI Electrical Impedance EIT Electrical Impedance Tomography EIS Electrical Impedance Segmentography EKG Electrocardiography ELBW Extremely Low Birth Weight Infants f Breathing Frequency FIFO First In, First Out fiO2 Fraction of inspired oxygen FRC Functional Residual Capacity g Gramm GA Gestational Age HFPPV High Frequency Positive Pressure Ventilation HR Heart Rate Hz Hertz IC Inspiratory Capacity IRV Inspiratory Reserve Volume MAP Mean Airway Pressure MRI Magnetic Resonance Imaging MS Microsoft NICU Neonatal Intensive Care Unit kg Kilogramm LL Lower Left Segment of the Thorax LR Lower Right Segment of the Thorax NG tube Nasogastric Tube PC Personal Computer PDA Patent Ductus Arteriosus PEEP Positive End Expiratory Pressure PiP Positive Inspiratory Pressure resI Residual Impedance SIMV Synchronized Intermittent Mandatory Ventilation TcCO2 Transcutaneous CO2 TTI Total Tidal Impdance tidI Tidal Impedance UL Upper Left Segment of the Thorax UR Upper Right Segment of the Thorax USB Universal Serial Bus

177
VT Tidal Volume vs versus wks Weeks yrs Years (age) 4D-CT Four-Dimensional Computed Tomography

178
Index of Figures FIGURE 1 SCHEME OF ELECTRICAL IMPEDANCE SEGMENTOGRAPHY [BAUER H, 2005] ............. 21 FIGURE 2 CROSS-SECTION OF THE THORAX ILLUSTRATION OF FIELD LINES AND POTENTIAL LINES WITHIN AN OBJECT. ......................................................................................... 22 FIGURE 3 CROSS-SECTION OF THE THORAX DISPLAYING ONE ORGAN TO ILLUSTRATE POTENTIAL LINES AND FIELD LINES WITHIN THE THORAX.[BAUER H, 2009] ............................... 23 FIGURE 4 SURPASS SYSTEM [BAUER H, 2005] .......................................................................... 23 FIGURE 5 EIS SOFTWARE - FRONT MASK .................................................................................. 26 FIGURE 6 FIRST EIS MEASUREMENTS IN A 2KG INFANT AND FIGURE 7 FIRST EIS MEASUREMENTS ....................................................................................................... 27 FIGURE 8 MAIN PATIENT GROUPS ............................................................................................. 30 FIGURE 9 DETAILS OF SPONTANEOUSLY BREATHING INFANTS .................................................. 31 FIGURE 10 INFANTS WITH ASSISTED VENTILATION ................................................................... 32 FIGURE 11 CROSS SECTION OF THE THORAX AT THE 2ND INTERCOSTAL SPACE AND FIGURE 12 CROSS SECTION OF THE THORAX AT THE 5TH INTERCOSTAL SPACE. ......................... 36 FIGURE 13 ELECTRODE SETTING IN A NEWBORN....................................................................... 37 FIGURE 14 ELECTRODE SETTING IN A NEWBORN ANTERIOR VIEW ............................................. 37 FIGURE 15 SCHEME OF ELECTRODE SETTING IN A NEWBORN AND FIGURE 16 SCHEME OF ELECTRODE IN A NEWBORN-POSTERIOR VIEW ............................................. 38 FIGURE 17 UNIPOLAR MODE – POSTERIOR VIEW ....................................................................... 39 FIGURE 18 CROSS SECTION OF THE THORAX AT THE 5TH INTERCOSTAL SPACE .......................... 39 FIGURE 19 “ELECTRODE- ONESIE”: THE CONCEPT ................................................................... 41 FIGURE 20 SYRINGE WITH A STUMP NEEDLE FIGURE 21 ELECTRODES WITHIN THE FABRIC 42 FIGURE 22 EXAMINATION COURSE IN SPONTANEOUSLY BREATHING INFANTS .......................... 44 FIGURE 23 EXAMINATION COURSE IN INFANTS WITH ASSISTED VENTILATION .......................... 45 FIGURE 24 SCHEME OF NORMAL BREATHING PATTERN IN A NEWBORN. .................................... 46 FIGURE 25 BREATHING PATTERN IN A SPONTANEOUSLY BREATHING INFANT. .......................... 46 FIGURE 26 TIDAL IMPEDANCE CHANGES MAY PRIMARILY BE REGULAR AND THAN BECOME OVERLAPPING WITH CARDIOVASCULAR CHANGES. ................................................. 47 FIGURE 27 TIDAL IMPEDANCE CHANGES OF THE LOWER RIGHT SEGMENT OF THE LUNGS IN A SPONTANEOUSLY BREATHING 1.5KG INFANT .......................................................... 48 FIGURE 28 RESIDUAL IMPEDANCE (BLUE LINES) IN 4 SEGMENTS OF THE LUNGS IN A SPONTANEOUSLY BREATHING 1.5KG INFANT .......................................................... 49 FIGURE 29 TIDAL IMPEDANCE OF THE LOWER LEFT QUADRANT OF THE THORAX IN A 1.5KG INFANT ON CPAP .................................................................................................. 51 FIGURE 30 DISPLAYS AN IMAGINARY LINE TO DEMONSTRATE THE CHANGE OF RESIDUAL IMPEDANCE IN THE LOWER LEFT SEGMENT OF THE LUNGS ....................................... 52 FIGURE 31 IMPEDANCE CHANGES IN 4 SEGMENTS OF THE LUNGS IN A 1.5KG INFANT ON CPAP 53 FIGURE 32 TIDAL IMPEDANCE OVER A ONE MINUTE PERIOD OF THE UPPER LEFT SEGMENT OF THE LUNGS IN A TERM INFANT WITH SIMV ...................................................................... 54 FIGURE 33 APNEA IN A 1.5KG INFANT IN ALL FOUR SEGMENTS OF THE LUNGS ......................... 55 FIGURE 34 TACHYPNEA MONITORED BY EIS IN ALL FOUR SEGMENTS OF THE LUNGS IN A 1.5 KG INFANT ................................................................................................................... 55 FIGURE 35 CARDIOVASCULAR IMPEDANCE CHANGES MOSTLY IN THE UPPER LEFT AND LOWER RIGHT SEGMENT OF THE LUNGS IN A 3.2KG NEWBORN WITH SIMV ........................ 56 FIGURE 36 SCREENSHOT OF DATA TRANSFERRED TO MS EXCEL .............................................. 57 FIGURE 37 AND FIGURE 38 ................................................................................................ 59 FIGURE 39 AND FIGURE 40 ................................................................................................ 59 FIGURE 41 AND FIGURE 42 ................................................................................................ 59

179
FIGURE 43 AND FIGURE 44 ................................................................................................ 60 FIGURE 45 AND FIGURE 46 ................................................................................................ 60 FIGURE 47 AND FIGURE 48 ................................................................................................ 60 FIGURE 49 AND FIGURE 50 TIDAL IMPEDANCE CHANGES THROUGHOUT A WHOLE EXAMINATION PERIOD ....................................................................................... 61 FIGURE 51 MIRRORED IMPEDANCE SIGNALS IN THE UPPER RIGHT AND LOWER LEFT SEGMENT OF THE LUNGS IN A 3.2 KG INFANT WITH SIMV. .......................................................... 64 FIGURE 52 TIDAL IMPEDANCE CHANGES IN SPONTANEOUSLY BREATHING INFANTS WITH A MEAN BODY WEIGHT OF 1690G. (N=3) .............................................................................. 67 FIGURE 53 TIDAL IMPEDANCE CHANGES WITHIN ALL 4 THE SEGMENTS DURING ALL EXAMINATION PERIODS. .......................................................................................... 68 FIGURE 54 RESIDUAL IMPEDANCE DISTRIBUTION WITHIN ALL SEGMENTS OF THE THORAX IN SPONTANEOUSLY BREATHING INFANTS WITH A MEAN BODY WEIGHT OF 1690G. (N=3)....................................................................................................................... 69 FIGURE 55 RESIDUAL IMPEDANCE CHANGES WITHIN ALL 4 THE SEGMENTS DURING ALL EXAMINATION PERIODS. .......................................................................................... 71 FIGURE 56 TIDAL IMPEDANCE DISTRIBUTION OF ALL 4 SEGMENTS OF THE THORAX IN SPONTANEOUSLY BREATHING INFANTS WITH A MEAN BODY WEIGHT OF 2200G (N=3)....................................................................................................................... 72 FIGURE 57 TIDAL IMPEDANCE CHANGES WITHIN ALL 4 THE SEGMENTS DURING ALL EXAMINATION PERIODS. .......................................................................................... 74 FIGURE 58 RESIDUAL IMPEDANCE IN ALL FOUR SEGMENTS OF THE THORAX IN SPONTANEOUSLY BREATHING INFANTS WITH A MEAN BODY WEIGHT OF 2200G. (N=3) ...................... 75 FIGURE 59 RESIDUAL IMPEDANCE CHANGES WITHIN ALL 4 THE SEGMENTS DURING ALL EXAMINATION PERIODS. .......................................................................................... 76 FIGURE 60 TIDAL IMPEDANCE IN 4 SEGMENTS OF THE THORAX IN SPONTANEOUSLY BREATHING INFANTS WITH A MEAN BODY WEIGHT OF 3516G (N=5) .......................................... 78 FIGURE 61 TIDAL IMPEDANCE CHANGES WITHIN ALL 4 THE SEGMENTS DURING ALL EXAMINATION PERIODS. .......................................................................................... 79 FIGURE 62 RESIDUAL IMPEDANCE IN 4 SEGMENTS OF THE THORAX IN SPONTANEOUSLY BREATHING INFANTS WITH A MEAN BODY WEIGHT OF 3516G (N=5) ........................ 80 FIGURE 63 RESIDUAL IMPEDANCE CHANGES WITHIN ALL 4 THE SEGMENTS DURING ALL EXAMINATION PERIODS. .......................................................................................... 81 FIGURE 64 TIDAL IMPEDANCE DISTRIBUTION OF ALL 4 SEGMENTS IN SUPINE POSITION IN 11 SPONTANEOUSLY BREATHING INFANTS. DISPLAYED ARE THE MEDIAN VALUES OF OUR FOUR SEGMENTS. ..................................................................................................... 86 FIGURE 65 TIDAL IMPEDANCE CHANGES IN ALL 4 QUADRANTS DURING ALL EXAMINATION PERIODS................................................................................................................... 87 FIGURE 66 RESIDUAL IMPEDANCE IN ALL SEGMENTS OF THE THORAX IN SUPINE POSITION IN SPONTANEOUSLY BREATHING INFANTS (N=11) ....................................................... 89 FIGURE 67 RESIDUAL IMPEDANCE CHANGES IN ALL 4 QUADRANTS DURING ALL EXAMINATION PERIODS................................................................................................................... 90 FIGURE 68 TIDAL IMPEDANCE IN FOUR SEGMENTS OF THE THORAX IN INFANTS WITH ASSISTED VENTILATION AT A PEEP OF 4.5CM H2O IN SUPINE POSITION. (N=4) ....................... 92 FIGURE 69 TIDAL IMPEDANCE DISTRIBUTION IN FOUR SEGMENTS OF THE THORAX IN INFANTS WITH ASSISTED VENTILATION DURING EXAMINATION PERIODS. (N=3) .................... 93 FIGURE 70 RESIDUAL IMPEDANCE DISTRIBUTION IN 4 INFANTS REQUIRING ASSISTED VENTILATION AND A MEAN BODY WEIGHT OF 2430G. .............................................. 94 FIGURE 71 RESIDUAL IMPEDANCE DISTRIBUTION IN ALL FOUR SEGMENTS OF THE THORAX DURING EXAMINATION PERIODS. .............................................................................. 96 FIGURE 72 RESIDUAL IMPEDANCE DISTRIBUTION IN 4 SEGMENTS OF THE THORAX IN INFANTS

180
WITH ASSISTED VENTILATION BASED ON BODY WEIGHT (N=4) ................................ 97 FIGURE 73 TIDAL IMPEDANCE CHANGES IN ABOLUTE NUMBERS DURING ALL EXAMINATION PERIODS IN FOUR SEGMENTS OF THE THORAX. ...................................................... 100 FIGURE 74 RESIDUAL IMPEDANCE CHANGES IN ABSOLUTE NUMBERS DURING ALL EXAMINATION PERIODS IN FOUR SEGMENTS OF THE THORAX. ...................................................... 101 FIGURE 75 TIDAL IMPEDANCE CHANGES IN ABSOLUTE (MEASURED) NUMBERS DURING ALL EXAMINATION PERIODS IN FOUR SEGMENTS OF THE THORAX. ................................ 104 FIGURE 76 RESIDUAL IMPEDANCE CHANGES IN ABSOLUTE (MEASURED) NUMBERS DURING ALL EXAMINATION PERIODS IN FOUR SEGMENTS OF THE THORAX. ................................ 105 FIGURE 77 TIDAL IMPEDANCE CHANGES IN ABSOLUTE (MEASURED) NUMBERS DURING ALL EXAMINATION PERIODS IN FOUR SEGMENTS OF THE THORAX. ................................ 107 FIGURE 78 RESIDUAL IMPEDANCE CHANGES IN ABSOLUTE (MEASURED) NUMBERS DURING ALL EXAMINATION PERIODS IN FOUR SEGMENTS OF THE THORAX ................................. 108 FIGURE 79 DECREASE OF RESI IN ALL 4 SEGMENTS OF THE THORAX DURING DISCONNECTION OF CPAP FOLLOWED BY A PERIOD OF SPONTANEOUS BREATHS IN A 1.5KG INFANT ... 109 FIGURE 80 EXAMINATION COURSE OF ALL 4 SEGMENTS OF THE THORAX DURING OUR INVESTIGATION. .................................................................................................... 111 FIGURE 81 EXAMINATION COURSE IN ALL 4 SEGMENTS OF THE THORAX DURING OUR INVESTIGATION. .................................................................................................... 111 FIGURE 82 EXAMINATION COURSE OF ALL 4 SEGMENTS OF THE THORAX DURING OUR INVESTIGATION. .................................................................................................... 114 FIGURE 83 EXAMINATION COURSE IN ALL 4 SEGMENTS OF THE THORAX DURING OUR INVESTIGATION. .................................................................................................... 114 FIGURE 84 ILLUSTRATES THE RELATIONSHIP BETWEEN RESIDUAL IMPEDANCE AND TIDAL IMPEDANCE ......................................................................................... 116 FIGURE 85 RESIDUAL IMPEDANCE IN THE 4 SEGMENTS OF THE THORAX. ................................ 117 FIGURE 86 RESI DISTRIBUTION WITHIN THE 4 SEGMENTS DURING CPAP AND FIGURE 87 RESI DISTRIBUTION WITHIN THE 4 SEGMENTS BREATHING SPONTANEOUSLY IN A 1.5KG INFANT ....................................... 118 FIGURE 88 TIDI DISTRIBUTION WITHIN THE 4 SEGMENTS DURING CPAP AND FIGURE 89 TIDI DISTRIBUTION WITHIN THE 4 SEGMENTS IN A SPONTANEOUSLY BREATHING 1.5 KG INFANT ..................................................... 118 FIGURE 90 TIDAL IMPEDANCE AND RESIDUAL IMPEDANCE IN 2 INFANTS DURING EXTUBATION/WEANING MANOEUVRE. .................................................................. 120 FIGURE 91 TIDAL IMPEDANCE CHANGES WITHIN 4 SEGMENTS OF THE THORAX IN SUPINE POSITION IN SPONTANEOUSLY BREATHING INFANTS. (N=11) ................................ 121 FIGURE 92 DISTRIBUTION OF RESIDUAL IMPEDANCE CHANGES WITHIN THE THORAX BASED ON BODY WEIGHT OF SPONTANEOUSLY BREATHING INFANTS (N=11) FIGURE 93 ELECTRODE MISPLACEMENT ................................................................................. 122 FIGURE 94 TIDAL IMPEDANCE CHANGES IN 4 SEGMENTS OF THE THORAX DURING ELECTRODE REPLACEMENT AND CONSECUTIVE EXAMINATION PERIODS. ................................. 124 FIGURE 95 RESIDUAL IMPEDANCE CHANGES IN 4 SEGMENTS OF THE THORAX DURING ELECTRODE REPLACEMENT AND CONSECUTIVE EXAMINATION PERIODS. .............. 124 FIGURE 96 CORRELATION BETWEEN TOTAL TIDAL IMPEDANCE IN 11 SPONTANEOUSLY BREATHING INFANTS AND THEIR BODY WEIGHT .................................................... 126 FIGURE 97 CORRELATION BETWEEN TOTAL RESIDUAL IMPEDANCE AND BODY WEIGHT IN 11 SPONTANEOUSLY BREATHING INFANTS ................................................................. 127 FIGURE 98 SIGNIFICANT CORRELATION BETWEEN RESIDUAL IMPEDANCE IN THE LOWER LEFT SEGMENT OF THE THORAX AND BODY WEIGHT OF INFANTS .................................. 128 FIGURE 99 SPONTANEOUSLY BREATHING INFANT OVER ONE MINUTE ..................................... 129 FIGURE 100 INFANT (1.5KG) BREATHING SPONTANEOUSLY IN PRONE POSITION, HEAD TURNED
181
TO THE RIGHT SIDE OF THE INFANT. ..................................................................... 130 FIGURE 101 INFANT (1.5KG) BREATHING SPONTANEOUSLY IN PRONE POSITION, HEAD TURNED TO THE LEFT SIDE OF THE INFANT. ....................................................................... 130 FIGURE 102 TIDAL IMPEDANCE OF THE UPPER LEFT SEGMENT AND THE LOWER RIGHT SEGMENT SHOW HIGHER TIDAL IMPEDANCE CHANGES THAN THE UPPER RIGHT SEGMENT AND THE LOWER LEFT SEGMENT OF THE LUNGS. ......................................................... 131 FIGURE 103 PERIODIC BREATHING IN A 1.5KG PREMATURE INFANT WITHOUT ANY RESPIRATORY OR NEUROLOGICAL DISEASE. .............................................................................. 132 FIGURE 104 PERIODIC BREATHING IN A 3.8KG INFANT AND FIGURE 105 PERIODIC BREATHING IN THE SAME INFANT DURING BREASTFEEDING ................................................... 132 FIGURE 106 PERIODIC BREATHING WITHOUT APNEA BUT CRESCENDO- DECRESCENDO CHARACTER OF TIDAL BREATHS IN A PRETERM 2KG INFANT. .............................. 133 FIGURE 107 PERIODIC BREATHING IN A 3.2KG INFANT IN SUPINE POSITION AND FIGURE 108 BREATHING PATTERN IN THE SAME INFANT DURING AUTOTRANSFUSION ............ 133 FIGURE 109 RECURRENCE OF PERIODIC BREATHING DURING LEFT SIDE POSITION AND FIGURE 110 PERSISTENCE OF PERIODIC BREATHING IN PRONE POSITION ................................. 133 FIGURE 111 1.5KG PREMATURE INFANT ON CPAP OVER ONE MINUTE. ................................... 134 FIGURE 112 TIDAL IMPEDANCE CHANGES IN A 3.2KG INFANT ON SIMV WITH BIRTH ASPHYXIA. ................................................................................................ 135 FIGURE 113 TIDAL IMPEDANCE CHANGES IN A 2KG INFANT ON SIMV AFTER SHUNT OPERATION. ............................................................................................. 135 FIGURE 114 TIDAL IMPEDANCE CHANGES IN A 2.9KG INFANT ON SIMV AND PEEP 4.5CM H2O DUE TO A PNEUMOTHORAX. ................................................................................ 136 FIGURE 115 TIDAL IMPEDANCE CHANGES IN A 2.9KG INFANT AND FIGURE 116 TIDAL IMPEDANCE CHANGES IN A 2.9KG INFANT PEEP 5.5CM H2O .............................. 136 FIGURE 117 TIDAL IMPEDANCE IN A SPONTANEOUSLY BREATHING INFANT WITH A BODY WEIGHT OF 1905G DURING EXAMINATION PERIODS WHEN FEEDING WAS PERFORMED IN LEFT SIDE POSITION. .................................................................... 138 FIGURE 118 RESIDUAL IMPEDANCE IN A SPONTANEOUSLY BREATHING INFANT WITH A BODY WEIGHT OF 1905G DURING EXAMINATION PERIODS WHEN FEEDING WAS PERFORMED IN LEFT SIDE POSITION. .................................................................... 139 FIGURE 119 TIDAL IMPEDANCE CHANGES IN A SPONTANEOUSLY BREATHING, HEALTHY 3.8KG INFANT DURING PLACEMENT IN LEFT SIDE POSITION AND PRONE POSITION. ........ 141 FIGURE 120 RESIDUAL IMPEDANCE CHANGES IN A SPONTANEOUSLY BREATHING, HEALTHY 3.8KG INFANT DURING PLACEMENT IN LEFT SIDE POSITION AND PRONE POSITION. 143 FIGURE 121 THIS FIGURE ILLUSTRATES THE 4D CT VENTILATION IMAGE SET OF A GROWN-UP PATIENT. ............................................................................................................. 147 FIGURE 122 4D-CT FINDINGS OF TIDAL VENTILATION COMPARED TO OUR FOUR SEGMENTS OF THE LUNGS AT THE PEAK OF INSPIRATION. .......................................................... 147

182
References 1 Loeb V, Domby M, Bauer H, Wemhoener A, Simbruner G, Ruediger M, Burkhardt W (2007). Online-Monitoring der thorakalen Belüftung mittels Quadranten-Impedanz-Messung. To be published 2 Burkhardt W, Domby M, Bauer H, Wemhoener A, Loeb V, Simbruner G, Ruediger M (2007). Quadranten-Impedanz-Messung: Uni- versus bipolare Ableitung. To be published 3 Simbruner G, Loeb V, Huang Q, Ruediger M (2006) Regionale Ventilation vermessen mittels Elektrischer Impedanz Tomographie (EIT) in Abhängigkeit von variierten Beatmungsfrequenzen und PEEP Einstellungen. Z Geburtshilfe Neonatol 2006, 210. 4 Papadakos P, Lachmann B (2002) The open lung concept of alveolar recruitment can improve outcome in respiratory failure and ARDS. The Mount Sinai Journal of Medicine, Jan- March 2002. 5 Gersing E (1999) Monitoring temperature-induced changes in tissue during hyperthermia by impedance methods. Ann N Y Acad Sci, 875 (1999), 13-20.
6 Brown BH (2003) Electrical Impedance Tomography (EIT): a review. Journal of Med Eng& Technol, 27-3 (2003), 97-108. 7 Dunlop S, Hough J, Riedel T, Fraser JF, Dunster K, Schibler A (2006) Electrical impedance tomography in extremely prematurely born infants and during high freguency oscillatory ventilation analyzed in the frequency domain. Physiol. Meas., 27 (2006), 1151-1165. 8 Heinrich S, Schiffmann H, Frerichs A, Klockgether- Radke A, Frerichs I (2006) Body and head position effects on regional lung ventilation in infants: an electrical impedance tomography study. Intensive Care Med, 32(9) (2006), 1290-1292 . 9 Frerichs I, Schmitz G, Pulletz S, Schaendler D, Zick G, Scholz J, Weiler N (2007) Reproducibility of regional lung ventilation distribution determined by electrical impedance tomography during mechanical ventilation. Physiol. Meas., 28 (2007), 261-267. 10 Leathard AD, Brown BH, Campell J, Zhang F, Morice AH, Tayler D (1994) A comparison of ventilatory and cardiac related changes in EIT images of normal human lungs and of lungs with pulmonary emboli. Physiol. Meas., 15 (1994), A137- A146. 11 Frerichs I, Dargaville PA, Dudykevych T, Rimensberger PC (2003) Electrical impedance tomography: a method for monitoring regional lung aeration and tidal volume distribution? Intensive Care Med., 29(12) (2003), 2312-2316 . 12 Luepschen H, Meier T, Grossherr M, Leibecke T, Karsten J, Leonhardt S (2007) Protective ventilation using electrical impedance tomography. Physiol. Meas., 28(7) (2007), S247-S260.
183
13 Pillow JJ, Frerichs I, Stocks J (2006) Lung function tests in neonates and infants with chronic lung disease: Global and regional ventilation inhomogeneity. Pediatr. Pulmonol., 41,105-121. 14 Frerichs I, Schiffmann H, Oehler R, Dudykevych T, Hahn G, Hinz J, Hellige G (2003) Distribution of lung ventilation in spontaneously breathing neonates lying in different body positions. Intensive Care Med., 29 (2003), 787-794. 15 Mishra S, Agarwal R, Jeevasankar M, Aggarwal R, Deorari AK, Paul VK (2008) Apnea in the newborn. Indian J Pediatr., 75(1) (2008),57-61. 16 Linder N, Haskin O, Levit O, Klinger G, Prince T, Naor N, Turner P, Karmazyn B, Sirota L.(2003) Risk factors for intraventricular hemorrhage in very low birth weight premature infants: a retrospective case-control study. Pediatrics, 111 (5 Pt1) (2003):e590-5.
17 van Genderingen HR, van Vught AJ, Jansen JR (2004) Regional lung volume during high-frequency oscillatory ventilation by electrical impedance tomography. Crit Care Med., 32(3) (2004), 787-94. 18 Li J (2000) Multifrequente Impedanztomographie zur Darstellung der elektrischen Impedanzverteilung im menschlichen Thorax. (Dissertation) 19 Kavvadia V, Greenough A, Itakura Y, Dimitriou G (1999) Neonatal lung function in very immature infants with and without RDS. J. Perinat. Med., 27 (1999), 382-387. 20 Dinger J, Töpfer A, Schaller P, Schwarze R (2001) Effect of positive end expiratory pressure on functional residual capacity and compliance in surfactant-treated preterm infants. J. Perinat. Med., 29 (2001) 137-143. 21 Hülskamp G, Pillow JJ, Dinger J, Stocks J (2006) Lung function tests in neonates and infants with chronic lung disease of infancy: Functional Residual Capacity. Ped. Pulmonol., 41 (2006), 1-22. 23 Bhat RY, Leipälä JA, Singh NR, Rafferty GF, Hannam S, Greenough A (2003) Effect of posture on oxygenation, lung volume, and respiratory mechanics in premature infants studied before discharge. Pediatrics 112 (2001) 29-32. 26 McEvoy C, Bowling S, Williamson K, Steward M, Durand M (2001) Functional residual capacity and passive compliance measurements after antenatal steroid therapy in preterm infants. Pediatr. Pulmonol. 31 (2001) 425-430. 27 Greenough A, Dimitriou G, Bhat RY, Broughton S, Hannam S, Rafferty GF, Leipälä JA (2005) Lung volumes in infants who had mild to moderate bronchopulmonary dysplasia. Eur J Pediatr. 164 (2005) 583–586. 28 Heinze H, Sedemund-Adib B, Heringlake M, Meier T, Eichler W (2009) Changes in functional residual capacity during weaning from mechanical ventilation: A Pilot Study. Crit. Care Med. 108, (2009) 911-915.

184
29 Siew ML, te Pas AB, Wallace MJ, Kitchen MJ, Lewis RA, Fouras A, Morley CJ, Davis PG, Yagi N, Uesugi K, Hooper SB (2009) Positive end-expiratory pressure enhances development of a functional residual capacity in preterm rabbits ventilated from birth. J Appl Physiol., 106 (2009) 1487-1493. 30 Cox RG, Ewen A, Bart BB (2001) The prone position is associated with a decrease in respiratory system compliance in healthy anaesthetized infants. Paediatric Anaesthesia 11 (2001) 291-296. 31 Stocks J, Godfrey S, Beardmore C, Bar-Yishay E, Castile R. (2001) Plethysmographic measurements of lung volume and airway resistance Eur Respir J 17 (2001) 302-312. 32 Kumar P, Leonidas JC, Ashtari M, Napolitano B, Steele AM (2005) Comparison of lung area by chest radiograph, with estimation of lung volume by helium dilution during prone and supine positioning in mechanically ventilated preterm infants: A pilot study. Pediatr. Pulmonol., 40 (2005) 219-222. 33 Guerrero T, Sanders K, Castillo E, Zhang Y, Bidaut L, Pan T, Komaki R (2006) Dynamic ventilation imaging from four-dimensional computed tomography. Phys. Med. Biol. 51 (2006) 777-791. 34 Petrofsky J (2008) The effect of the subcutaneous fat on the transfer of current through the skin and into muscle. Med Eng Phys 30 (2008) 1168-76. 35 Hülskamp G, Hoo AF, Ljungberg H, Lum S, Pillow JJ, Stocks J (2003) Progressive decline in plethysmographic lung volumes in infants: physiology or technology? Am J Respir Crit Care Med 168 (2003) 1003-9.
36 Blondheim O, Abbasi S, Fox WW, Bhutani VK (1993) Effect of enteral gavage feeding rate on pulmonary functions of very low birth weight infants. J Pediatr 122 (1993) 751-5. 37 Mizuno K, Itabashi K, Okuyama K (1995) Effect of body position on the blood gases and ventilation volume of infants with chronic lung disease before and after feeding. Am J Perinatol. 12 (1995) 275-7. 38 Javorka K, Tomori Z, Zavarská L (1982) Mechanics of breathing during sneezing and crying in premature newborns. Eur J Respir Dis, 63 (1982) 442-8. 39 Maynard V, Bignall S, Kitchen S (2000) Effect of positioning on respiratory synchrony in non-ventilated pre-term infants. Physiother Res Int., 5 (2000) 96-110. 40 Mure M, Lindahl SGE (2001) Prone position improves gas exchange – but how? Acta Anaesthesiol Scand., 45 (2001) 150-159. 41 Kelly DH, Shannon DC (1981) Treatment of apnea and excessive periodic breathing in the full-term infant. Pediatrics, 68 (1981) 183-186. 42 Sanchack KE (2004) Hiccups: When the diaphragm attacks. Journal of Palliative Med., 7 (2004) 870-873.

185
45 Löb V (2005) Regional lung ventilation assessed by electrical impedance measurements at various ventilator frequencies and PEEP levels. Doctoral Thesis (2005) 47 von Ungern-Sternberg BS, Frei FJ, Hammer J, Schibler A, Doering R, Erb TO (2007) Impact of depth of propofol anaesthesia on functional residual capacity and ventilation distribution in healthy preschool children. Br J Anaesth 98, (2007) 503-508. 48 Chawla G, Drummond GB (2008) Fentanyl decreases end-expiratory lung volume in patients anaesthetized with sevoflurane. Br J Anaesth 100, (2008) 411-414.
49 von Ungern-Sternberg BS, Erb TO, Habre W, Sly PD, Hantos Z (2009) The impact of oral premedication with midazolam on respiratory function in children. Anesth. Analg 108, (2009) 1771-1776. 51 Greenough A, Dimitriou G, Prendergast M, Milner AD (2004) Synchronized mechanical ventilation for respiratory support in newborn infants. Cochrane Database Syst Rev. 4, (2004): CD000456, retrieved June 26, 2009. 52 Morrow BM, Argent AC (2008) A comprehensive review of pediatric endotracheal suctioning: Effects, indications, and clinical practice. Pediatr Crit Care Med. 9, (2008) 539-540. 53 Simbruner G, Coradello H, Lubec G, Pollak A, Salzer H (1982) Respiratory compliance of newborns after birth and its prognostic value for the course and outcome of respiratory disease. Respiration 43, (1982) 414- 423. 54 Moss TJ (2006) Respiratory consequences of preterm birth. Clin Exp Pharmacol Physiol 33, (2006) 280- 284. 57 Frerichs I, Dudykevych T, Hinz J, Bodenstein M, Hahn G, Hellige G (2001) Gravity effects on regional lung ventilation determined by functional EIT during parabolic flights. J Appl Physiol. 91, (2001) 39-50. 58 Boutroy MJ (1994) Drug induced apnea. Biol Neonate 65, (1994) 252-257.
59 Welzig L, Kribs A, Huenseler C, Eifinger F, Mehler K, Roth B (2009) Remifentanil for INSURE in preterm infants: a pilot study for evaluation of efficiancy and safety aspects. Acta Paediatr. Epub May 25, 2009
186
Books 22 Schneider D (2006) The cardiovascular system. In RM Kliegman, KJ Marcdante, HB Jenson, and RE Behrman (Eds.) Nelson Essentials of Pediatrics (p. 657, 5th ed.) Philadelphia: Saunders Elsevier 24 Carlo WA, Di Fiore JM (2005) Assessment of pulmonary function. In RJ Martin, AA Fanaroff, and MC Walsh (Eds.) Fanaroff and Martin’s Neonatal Perinatal Medicine, Diseases of the Fetus and Infant (pp.1087- 1097, 8 th ed.) Philadelphia: Mosby Elsevier 25 Oczenski W, Werba A, Andel H (1996) Statische Lungenvolumina. In W.Oczenski, A. Werba, and H. Andel (Eds.) Atmen-, Atemhilfen – Atemphysiologie und Beatmungsmechanik (pp. 59-65, 3rd ed.) Berlin, Wien: Blackwell Wissenschaftsverlag 43 Carlo WA, Martin RJ, Fanaroff AA (2005) Assisted ventilation and complications of respiratory distress. In RJ Martin, AA Fanaroff, and MC Walsh (Eds.) Fanaroff and Martin’s Neonatal Perinatal Medicine, Diseases of the Fetus and Infant (pp.1114-1115, 8 th ed.) Philadelphia: Mosby Elsevier 44 Wung JT (2006) Mechanical ventilation of the newborn – Using conventional infant ventilators. In 18th Annual Course – Respiratory Care of the Newborn, a Practical Approach . (p 85). 50 Oczenski W, Werba A, Andel H (1996) Physiologie des Gasaustausches. In W.Oczenski, A. Werba, and H. Andel (Eds.) Atmen-, Atemhilfen – Atemphysiologie und Beatmungsmechanik (pp. 33-52, 3rd ed.) Berlin, Wien: Blackwell Wissenschaftsverlag 55 Rodriguez RJ, Martin RJ, Fanaroff AA (2005) Respiratory distress syndrome and its management. In RJ Martin, AA Fanaroff, and MC Walsh (Eds.) Fanaroff and Martin’s Neonatal Perinatal Medicine, Diseases of the Fetus and Infant (pp.1097-1107, 8 th ed.) Philadelphia: Mosby Elsevier 56 Wung JT (2006) CPAP Therapy In 18th Annual Course – Respiratory Care of the Newborn, a Practical Approach . (p 6).
Internet 46 Orlischer M. Perinatale Asphyxie, retrieved from https://www.meduniwien.ac.at/sg/files/16/312/asphyxie_(olischar).pdf June 25, 2009