Neue Antikoagulantien in der Therapie des … · Folie 2 Vorhofflimmern - häufigste kardiale...
80
Neue Antikoagulantien in der Therapie des Vorhofflimmerns Halle, April 2013
Transcript of Neue Antikoagulantien in der Therapie des … · Folie 2 Vorhofflimmern - häufigste kardiale...

Neue Antikoagulantien in der Therapie des Vorhofflimmerns
Halle, April 2013
Folie 2
Vorhofflimmern
- häufigste kardiale Rhythmusstörung 1-2% in der Gesamtbevölkerung 5-15% > 80 Jahre
- etwa 5-fach erhöhtes Hirninfarktrisiko - 15% aller Hirninfarkte1
30% der Hirninfarkte > 80 Jahre1
1Wolf PA et al., Stroke 1991; 22: 983-988

Folie 3
VHF: TE-Risiko
Vorhofflimmern
lokale Hyperkoagulabilität
intraartriale Thromben
embolischer Hirninfarkt

Folie 4
VHF: TE-Prophylaxe
Vorhofflimmern
lokale Hyperkoagulabilität
intraartriale Thromben
embolischer Hirninfarkt
antikoagulatorische Therapie

Folie 5
- Reduktion der Schlaganfallhäufigkeit durch Therapie mit Vitamin-K-Antago- nisten (INR: 2-3).2
- Primärprophylaxe: 60-75%ige Reduktion2 - Sekundärprophylaxe: 70%ige Reduktion
VHF und Antikoagulation
2Hart RG et al. Ann Intern Med 2007; 146: 857-867
Folie 6
- antikoagulatorische Wirkung durch Hemmung der γ-Carboxylierung
- hohe inter- und intraindividuelle Variabilität
erfordert regelmäßige Therapiekontrollen - relativ lange Halbwertszeiten
Acenocoumarol 3-11h Warfarin 30-50 h, Phenprocoumon 90-140h
VKA: Profil (1)

Folie 7
- Blutungen: 7,6%/100 Behandlungsjahre davon 1,1% schwer, 0,25% tödlich3
- wirksame Antagonisationsstrategien
verfügbar (Vit.-K/PPSB)
VKA: Profil (2)
3Palareti G et al. Lancet 1996; 348: 432-438
Folie 8
- effektive antikoagulatorische Wirkung - jahrzehntelanges Erfahrungspotenzial - Überwachung der Therapieeffizienz
möglich - Antidot und Antagonisierungsstrategie
verfügbar
VKA: Vorteile

Folie 9
- in der Einstellungsphase begleitende anti- koagulatorische Therapie erforderlich
- regelmäßiges Monitoring erforderlich - periinterventioneller Antikoagulanzien-
wechsel erforderlich - relativ hohe Rate an schweren Blutungs-
komplikationen
VKA: Nachteile

Folie 10
- Vitamin-K-Antagonisten Phenprocoumon/Warfarin
- Direkte FXa-Inhibitoren
Rivaroxaban (Xarelto®) Apixaban (Eliquis®)
- Direkte FIIa-Inhibitoren
Dabigatran (Pradaxa®)
Orale Antikoagulanzien
Folie 11
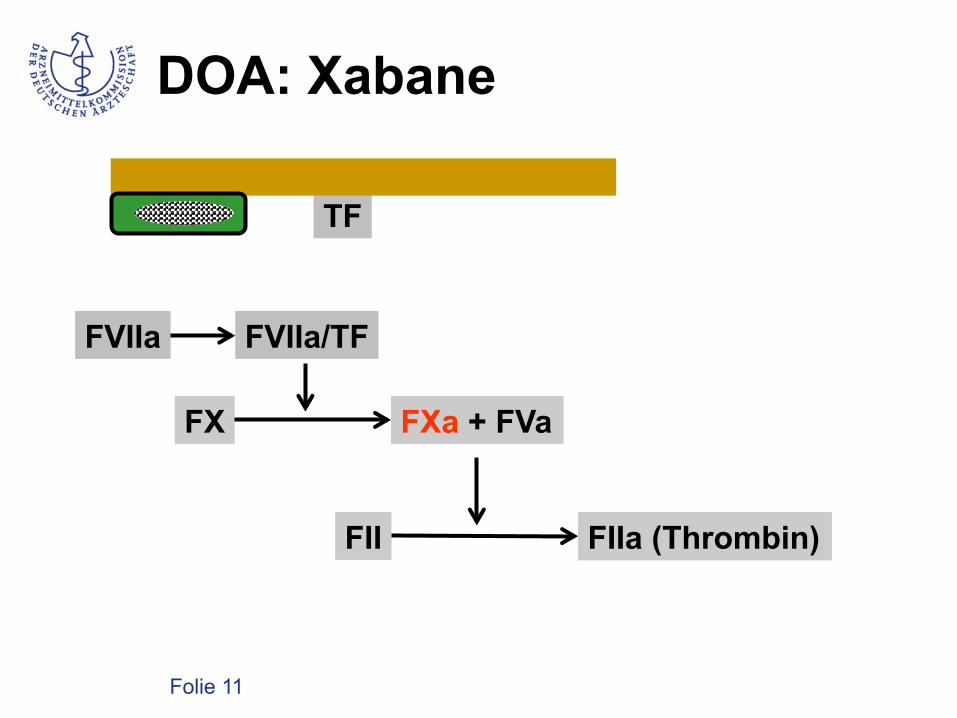
DOA: Xabane
FX
FII
FXa + FVa
FIIa (Thrombin)
FVIIa FVIIa/TF
TF EC Gewebsverletzung
EC Gerinnsel

Folie 12
- Vitamin-K-Antagonisten Phenprocoumon/Warfarin
- Direkte FXa-Inhibitoren
Rivaroxaban (Xarelto®) Apixaban (Eliquis®)
- Direkte FIIa-Inhibitoren
Dabigatran (Pradaxa®)
Orale Antikoagulanzien

Folie 13
DOA: Dabigatran
FX
FII
FXa + FVa
FIIa (Thrombin)
FVIIa FVIIa/TF
TF EC Gewebsverletzung
EC Gerinnsel

Folie 14 Kubitza et al., J Clin Pharmacol 2007; 47: 218 - 226
Rivaroxaban: Kinetik
222 • J Clin Pharmacol 2007;47:218-226
KUBITZA ET AL
0.80-1.03) between the >120 kg group and the 70 to80 kg group. All of the CIs were within the interval0.8 to 1.25, indicating bioequivalence.15 The timecourse of inhibition of FXa activity followed a simi-lar pattern in all 3 groups, although the return of FXaactivity to baseline was slightly slower with increas-ing weight. This resulted in the AUC0-tn of the inhibi-tion of FXa activity versus time curve increasing withincreasing body weight; however, differences betweenthe groups were not significant (P = .07).
Rivaroxaban prolonged PT, and placebo had noeffect (Figure 2B). The Emax for prolongation of PTdecreased significantly (P < .001) with increasingbody weight, with LS-means ratios of 1.15 (90% CI,1.01-1.32) between the !50 kg group and the 70 to80 kg group and 0.82 (90% CI, 0.72-0.94) between the70 to 80 kg group and the >120 kg group. Maximumprolongation was observed 2 to 3 hours after admin-istration of rivaroxaban, and PT almost completelyreturned to baseline after 15 hours. The return to
Table II Pharmacokinetics of Rivaroxaban 10 mg After Administration to Female Subjects of !50 kgand Male and Female Subjects of 70 to 80 kg and >120 kg Body Weight
Parameter !!50 kg (n = 12) 70-80 kg (n = 12) >120 kg (n = 12)
AUC, µg • h/La 1172 (22.00) 1029 (20.10) 1155 (15.60)LS-means ratio body weightb 1.14 (0.98-1.30) — 1.12 (0.98-1.28)LS-means ratio genderc — 0.97 (0.81-1.15) 0.85 (0.72-1.02)
AUCnorm, g • h/La 5665 (22.70) 7611 (19.20) 15 230 (18.50)Cmax, µg/La 178.1 (16.60) 143.4 (26.50) 149.0 (20.40)
LS-means ratio body weightb 1.24* (1.07-1.44) — 1.04 (0.90-1.20)LS-means ratio genderc — 0.98 (0.78-1.24) 0.81 (0.64-1.02)
Cmax,norm, g/La 860.7 (16.60) 1061.0 (25.90) 1964.0 (23.10)tmax, h
d 4.00 (1.00-4.00) 3.50 (1.00-4.00) 4.00 (2.00-4.00)t!, ha 9.60 (36.70) 7.20 (42.10) 7.30 (25.40)Vz/F, L/kga 2.44 (53.30) 1.36 (37.40) 0.69 (35.80)Total unchanged rivaroxaban excreted in urine, %a 25 (58) 35 (18) 29 (25)
AUC = area under the plasma-concentration time curve from time 0 to infinity; AUCnorm = AUC normalized to dose and body weight; Cmax = maximumplasma concentration; Cmax,norm = Cmax normalized to dose and body weight; tmax = time of Cmax; t! = half-life associated with the terminal slope; Vz/F =apparent volume of distribution during the terminal phase after oral administration.a. Geometric means (percentage coefficient of variation).b. Least squares (LS)–means ratios versus the 70 to 80 kg group (90% confidence interval).c. LS-means ratios of men versus women (90% confidence interval).d. Median (range).*Significantly different from the 70 to 80 kg group (P = .04).
Figure 1. Mean plasma concentrations of rivaroxaban after administration of 10 mg to healthy, male and female subjects (A) in 3 weightgroups (n = 12 per group) and (B) by gender for the 70 to 80 kg and >120 kg weight groups (n = 6 per category).
Folie 15
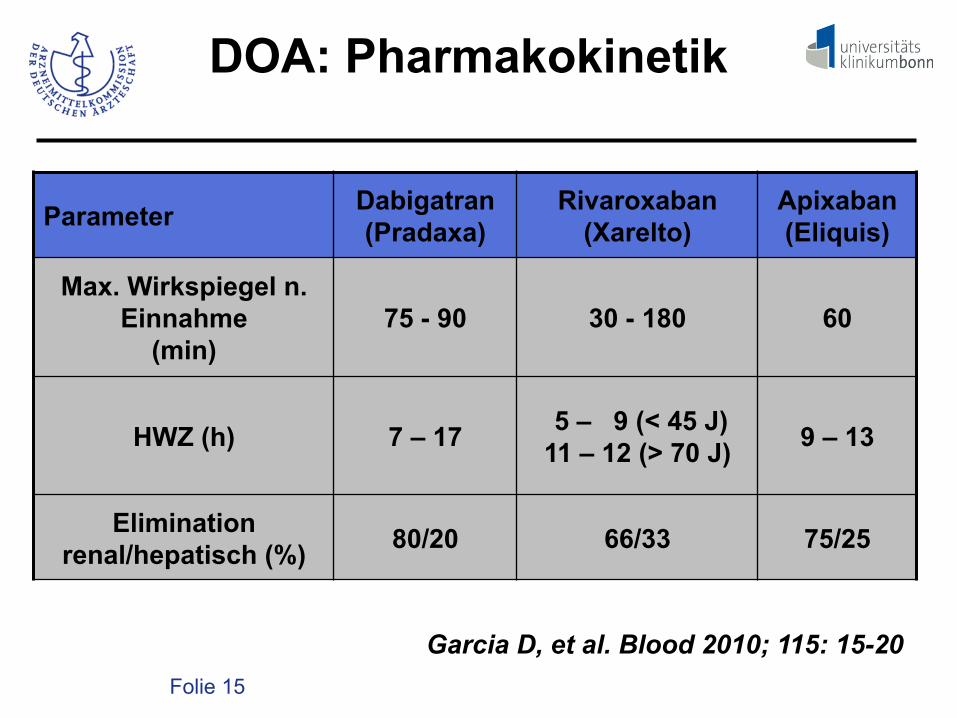
Parameter Dabigatran (Pradaxa)
Rivaroxaban (Xarelto)
Apixaban (Eliquis)
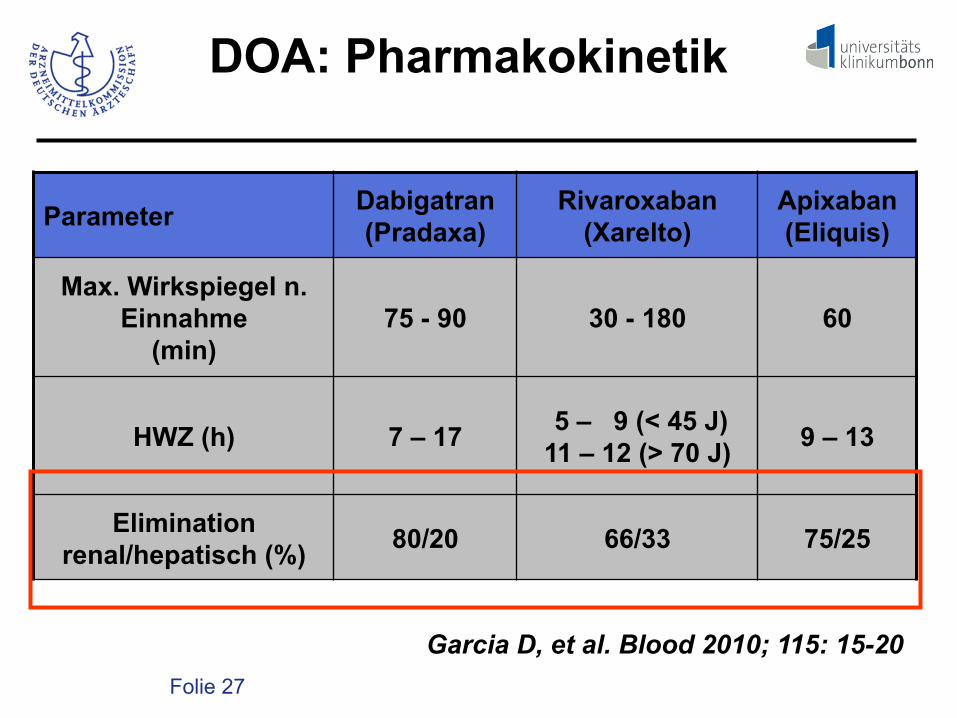
Max. Wirkspiegel n. Einnahme
(min) 75 - 90 30 - 180 60
HWZ (h)
7 – 17 5 – 9 (< 45 J)
11 – 12 (> 70 J) 9 – 13
Elimination renal/hepatisch (%) 80/20 66/33 75/25
DOA: Pharmakokinetik
Garcia D, et al. Blood 2010; 115: 15-20

Folie 16
- antikoagulatorische Wirkung durch Hemmung von FXa oder Thrombin
- geringe Variabilität in Plasmaspiegeln è pauschalierte Gabe möglich
DOA: Profile

Folie 17
Zur Prophylaxe von kardialen thrombo- embolischen Komplikationen: - Apixaban: 2 x 5 mg - Dabigatran: 2 x 110/150 mg - Rivaroxaban: 1 x 20 mg
DOA: Dosierungen

Folie 18
RE-LY: Indikation VHF
Connolly SJ et al. N Engl J Med 2009; 36: 1139 - 1151
Event
Dabigatran
2 x 110 mg
N = 6015
Dabigatran
2 x 150 mg
N = 6076
Warfarin
INR 2-3
N = 6076
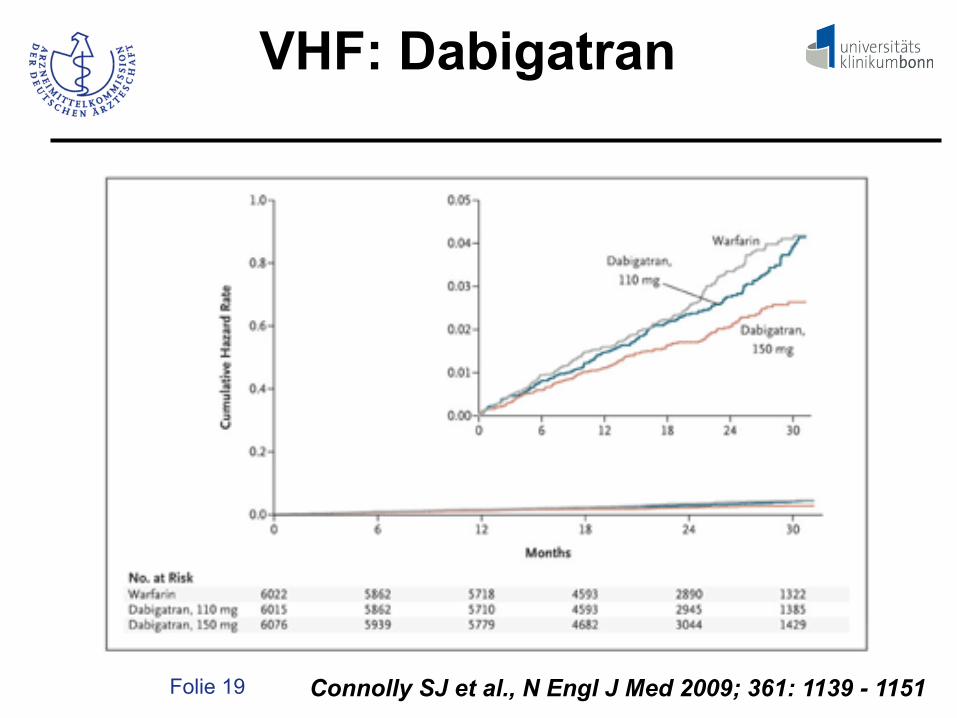
Stroke/TE 183 (1.5%) 134 (1.1%) 202 (1.7%)
Ischemic stroke 152 (1.3%) 103 (0.9%) 134 (1.1%)
Folie 19
VHF: Dabigatran
Connolly SJ et al., N Engl J Med 2009; 361: 1139 - 1151

Folie 20
Rivaroxaban: VHF
Garcia D et al., Blood 2010; 115: 15-20
Indika'on Pa'entenzahl Akronym
Periop.Thrombose-‐ prophylaxe 8.500 RECORD 1-‐4
Vorhofflimmern 14.000 ROCKET-‐AF
Thrombosetherapie 6.200 EINSTEIN DVT/PE
Sek. Thrombose-‐prophylaxe 1.300 EINSTEIN
extension study
Folie 21
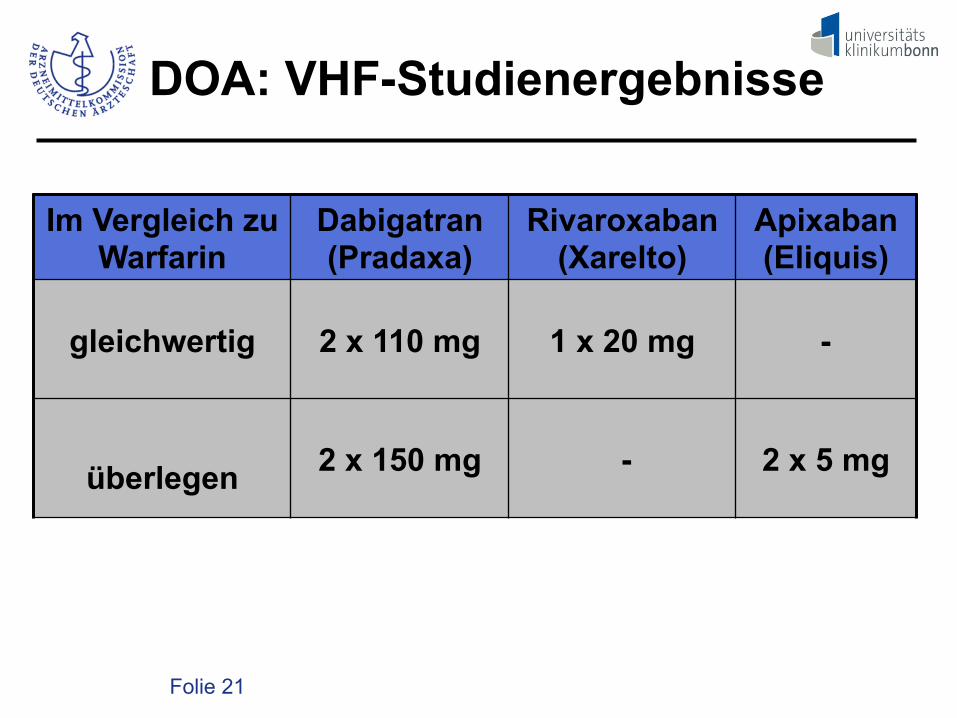
Im Vergleich zu Warfarin
Dabigatran (Pradaxa)
Rivaroxaban (Xarelto)
Apixaban (Eliquis)
gleichwertig 2 x 110 mg 1 x 20 mg -
überlegen 2 x 150 mg - 2 x 5 mg
DOA: VHF-Studienergebnisse

Folie 22
Major bleedings %/year
DOA vs. VKA DOA Warfarin
Dabigatran1 2 x 110 mg 2,71 3,36 Dabigatran1 2 x 150 mg 3,11 3,36 Rivaroxaban2 1 x 20/15 mg 3,60 3,40 Apixaban3 2 x 5 mg 2,13 3,09
1 ConnollySJ et al., N Engl J Med 2009;361:1139-51 2 Patel MR et al., N Engl J Med 2011;365:883-91 3 Granger CB et al., N Engl J Med 2011;365:981-92

Folie 23
Intracranial bleeding %/y.
DOA vs. VKA DOA Warfarin
Dabigatran1 2 x 110 mg 0,23 0,7 Dabigatran1 2 x 150 mg 0,3 0,7 Rivaroxaban2 1 x 20/15 mg 0,5 0,7 Apixaban3 2 x 5 mg 0,33 0,8
1 ConnollySJ et al., N Engl J Med 2009;361:1139-51 2 Patel MR et al., N Engl J Med 2011;365:883-91 3 Granger CB et al., N Engl J Med 2011;365:981-92

Folie 24
VKA-Blutung: Outcome
Blutungslokalisation In-hospital mortality (%)
Parenchymblutung 42 Subdurale Blutung 34 Epidurale Blutung 0 Subarachnoidale Blutung 13
Dowlatshahi D, et al. Stroke 2012; 43: 1812 - 1817

Folie 25
- Welcher Patient mit VHF profitiert von den DOA, welcher profitiert nicht?
- Welcher Patient sollte mit DOA
behandelt werden?
DOA: Fragen

Folie 26
- Ist ein Therapiemonitoring möglich? - Was tun bei Überdosierungen? - Was tun bei Interventionen? - Welche Kosten entstehen?
DOA: Fragen
Folie 27
Parameter Dabigatran (Pradaxa)
Rivaroxaban (Xarelto)
Apixaban (Eliquis)
Max. Wirkspiegel n. Einnahme
(min) 75 - 90 30 - 180 60
HWZ (h)
7 – 17 5 – 9 (< 45 J)
11 – 12 (> 70 J) 9 – 13
Elimination renal/hepatisch (%) 80/20 66/33 75/25
DOA: Pharmakokinetik
Garcia D, et al. Blood 2010; 115: 15-20

Folie 28
Dabigatran: Interaktionen6
- Cytochrom-P-450-Substrat: nein - P-Glykoprotein-Substrat: ja → Bioverfügbarkeit wird durch Amiodaron
gesteigert.
6Ufer M, Thromb Haemost 2010; 103: 572 - 585
Folie 29
Rivaroxaban: Interaktionen6
- Cytochrom-P-450-Substrat: nein - P-Glykoprotein-Substrat: ja → Bioverfügbarkeit wird durch Amiodaron
gesteigert.
6Ufer M, Thromb Haemost 2010; 103: 572 - 585

Folie 30
- antikoagulatorische Wirkung durch Hemmung von FXa oder Thrombin
- geringe Variabilität in Plasmaspiegeln è pauschalierte Gabe möglich è im Einzelfall Dosisadjustierungen
erforderlich
DOA: Profile

Folie 31
DOA: Gerinnungsteste
- Grundsätzlich können alle FXa- oder FIIa- abhängigen Gerinnungsteste durch FXa- oder FIIa-Inhibitoren beeinflusst werden.
- Unterschiede existieren in der Sensitivität
und in der Linearität.
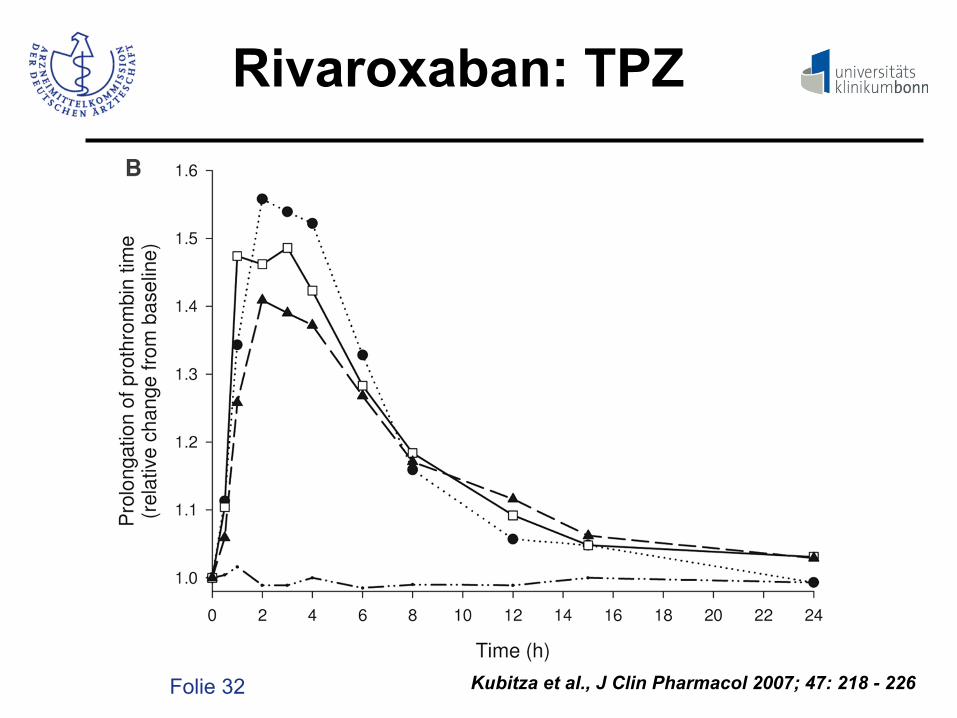
Folie 32 Kubitza et al., J Clin Pharmacol 2007; 47: 218 - 226
Rivaroxaban: TPZ

Folie 33
Dabigatran: APTT7
Thrombin time (TT)
TT was too sensitive leading to high variability for concentrations higher than 25 ng/ml in the initial blood sample (data not shown).
Hemoclot Thrombin Inhibitor! (HTI)
HTI showed a concentration dependent prolongation of clotting time (!Fig. 3). The variability was 0.9% and 2.5% in intra- and inter-assay, respectively.
Ecarin clotting time (ECT)
ECT showed a concentration-dependent prolongation of clotting time. For the two concentrations of ecarin tested, 2 x CT was 15 ng/ml and 21 ng/ml for ECT 5 IU/ml and 1.67 IU/ml in final mixture, respectively (!Fig. 4). Reproducibility [mean CV (%)] was 0.7% for ECT 1.67 IU/ml and 0.9% for ECT 5 IU/ml, respectively. Inter-lot reproducibility showed a similar response until 470 ng/ml in the initial sample with a CV = 3.1% (2 x CT was 17 ng/ml; 23 ng/ml and 21 ng/ml, respectively) (!Fig. 4). Nevertheless, with con-centration higher than 470 ng/ml, some samples showed a coagu-lation time exceeding the limit of measurement. Thus, CV in-creased with a value of 5.1% and sensitivity decreased sharply (38 ng/ml, 41.5 ng/ml and 39 ng/ml, respectively, for the three different lots tested) (data not shown).
© Schattauer 2012 Thrombosis and Haemostasis 107.5/2012
989 Douxfils, Mullier et al. Laboratory recommendations for monitoring dabigatran
Figure 2: Influence of dabigatran on acti-vated the partial thromboplastin time (aPTT). aPTT showed a concentration-dependent prolongation of clotting time with a loss of sensi-tivity for higher concen-trations in dabigatran. Actin FS! was the most sensitive test with a 2 x CT of 83 ng/ml but suf-fered from a lower repro-ducibility. The box in blue and red represents the therapeutic range in the orthopaedic indication and in AF patients, re-spectively. Cut-offs at Ctrough of 67 ng/ml and 200 ng/ml are defined for the orthopaedic indi-cation (220 mg qd) and for the AF patients (150 mg bid), respectively (15).
For personal or educational use only. No other uses without permission. All rights reserved.Downloaded from www.thrombosis-online.com on 2012-05-02 | ID: 1000502741 | IP: 131.220.35.99
7Douxfils J et al. Thromb Haemost 2012; 107: 985-997

Folie 34
Dabigatran: Thrombin inhibition7
7Douxfils J et al. Thromb Haemost 2012; 107: 985-997 Ecarin chromogenic assay (ECA)
ECA showed a concentration-dependent decrease of OD/min. 2 x OD/min was 4 ng/ml, but the sensitivity decreased with the high-est concentrations of dabigatran making the relation non-linear (see !Fig. 9 in the Suppl. materials, available online at www.thrombosis-online.com). By measuring the time necessary to obtain an
OD = 1, results showed a concentration needed to double the time necessary to reach the value of 1 in absorbance of 7 ng/ml, but re-sults were not linear for concentrations lower than 50 ng/ml (!Fig. 5). For all the concentrations above and until 940 ng/ml, the relation was linear as shown in a previous study performed on argatroban (25).
990 Douxfils, Mullier et al. Laboratory recommendations for monitoring dabigatran
Thrombosis and Haemostasis 107.5/2012 © Schattauer 2012
Figure 3: Influence of dabigatran on Hemo-clot Thrombin In-hibitor! (HTI). HTI showed a concentration-dependent prolongation of clotting time with a lin-ear relation and a good reproducibility. HTI is the most sensitive assay with a 2 x CT of 8 ng/ml. The box in blue and red repre-sents the therapeutic range in the orthopaedic indication and in AF pa-tients, respectively. Cut-offs at Ctrough of 67 ng/ml and 200 ng/ml are de-fined for the orthopaedic indication (220 mg qd) and for AF patients (150 mg bid), respectively (15).
Figure 4: Influence of dabigatran on ecarin clotting time (ECT) 5 IU/ml and 1.66 IU/ml in final concentration. Mean 2 x CT was 21 ng/ml for ECT 1.66 IU/ml versus 15 ng/ml for ECT 5 IU/ml. ECT 1.66 IU/ml showed a better cor-relation coefficient than ECT 5 IU/ml (R2>0.99 vs. 0.98). Results obtained inter-
lots were very reproducible up to 470 ng/ml. The box in blue and red represents the therapeutic range in the orthopaedic indication and in AF patients, respect-ively. Cut-offs at Ctrough of 67 ng/ml and 200 ng/ml are defined for the orthopaedic indication (220 mg qd) and for AF patients (150 mg bid), respectively (15).
For personal or educational use only. No other uses without permission. All rights reserved.Downloaded from www.thrombosis-online.com on 2012-05-02 | ID: 1000502741 | IP: 131.220.35.99

Folie 35
AT FXa AT-FXa
chromogenes Substrat Δ OD
FXa
+
Anti-FXa-Bestimmung

Folie 36
AT FXa Ri-FXa
chromogenes Substrat Δ OD
FXa
+
Anti-FXa-Bestimmung
Ri
Ri = Rivaroxaban

Folie 37
DOA-Monitoring: Fazit
- In der Regel ist eine pauschalierte Gabe ohne Drug-Monitoring möglich.
- Ein Monitoring wird bei Patienten mit
eingeschränkter Nierenfunktion (CrCl < 30 ml/min) oder relevanter Begleit- medikation/Medikamentenwechsel empfohlen.
- Meist ist ein kurzfristiges Monitoring aus-
reichend.

Folie 38
DOA-Monitoring: Fazit
- Die APTT ist geeignet eine Überdosierung zu erkennen.
- Dabigatran: Die Bestimmung der anti-Throm-
bin-Aktivität ermöglicht eine quantitative Bestimmung.
- Rivaroxaban/Epixaban: Die Bestimmung der
Anti-FXa-Aktivität ermöglicht eine quantita- tive Bestimmung.

Folie 39
- Ist ein Therapiemonitoring möglich? - Was tun bei Überdosierungen? - Was tun bei Interventionen? - Welche Kosten entstehen?
DOA: Fragen

Folie 40
Intracranial bleeding %/y.
DOA vs. VKA DOA Warfarin
Dabigatran1 2 x 110 mg 0,23 0,7 Dabigatran1 2 x 150 mg 0,3 0,7 Rivaroxaban2 1 x 20/15 mg 0,5 0,7 Apixaban3 2 x 5 mg 0,33 0,8
1 ConnollySJ et al., N Engl J Med 2009;361:1139-51 2 Patel MR et al., N Engl J Med 2011;365:883-91 3 Granger CB et al., N Engl J Med 2011;365:981-92

Folie 41
Antagonisationsstrategien
Kurzfristige Unterbrechung der antikoa- gulatorischen Wirkung durch: - ein Antidot - Elimination - unspezifische Hämostyptika
Folie 42
Spezifische Inhibitoren
Unfraktioniertes Heparin – Protamin Vitamin-K-Antagonisten – Vitamin K/PPSB Apixaban/Rivaroxaban – Dabigatran –

Folie 43
Spezifische Inhibitoren
Unfraktioniertes Heparin – Protamin Vitamin-K-Antagonisten – Vitamin K/PPSB Apixaban/Rivaroxaban – rFXai
1
Dabigatran –
1Lu G et al. Nature Med 2013; 19: 446- 453

Folie 44
Inaktiver Faktor Xa (FXai)
A R T I C L E S
NATURE MEDICINE VOLUME 19 | NUMBER 4 | APRIL 2013 447
weight for the r-Antidote light chain compared to plasma-derived fXa. The double bands observed for the heavy chain of both plasma-derived fXa and r-Antidote correspond to the - and -isoforms of the protein. The -isoform results from additional proteolytic cleav-age at the C terminus of the heavy chain11,12. We verified the identity of the heavy and light chains of the purified proteins by western blot-ting with human fX- and Xa-specific monoclonal antibodies (data not shown). N-terminal sequencing of both the light and heavy chains of purified r-Antidote yielded the expected amino acid sequences, indi-cating proper processing of the PrePro sequence at the N-terminus of the light chain and the RKRRKR linker at the N-terminus of the heavy chain (data not shown). To produce functional protein, proper processing requires that the N terminus of the heavy chain start at Ile235 and the RKRRKR linker be completely removed.
Reversal of direct fXa inhibitors by r-AntidoteWe determined the potency (Kd) of r-Antidote binding to three direct fXa inhibitors (betrixaban, rivaroxaban and apixaban) and compared
them to inhibition of purified human fXa using a peptidyl substrate (Fig. 2a). r-Antidote dose-dependently reversed the inhibitory activity of the small-molecule fXa inhibitors but did not produce any change in the rate of peptidyl substrate cleavage by fXa in the absence of inhibitor. This observation is consistent with the expected lack of catalytic activity of r-Antidote. Analysis of these kinetic data indi-cated that r-Antidote has subnanomolar affinities for these direct fXa inhibitors (Table 1). The relative potency of binding was in the same order of magnitude as the inhibition constants (Ki) reported in the literature for these inhibitors against plasma-derived fXa13–15.
After testing in a purified enzyme system, we evaluated the ability of r-Antidote to reverse the effects of anticoagulation in plasma. We determined the residual inhibitory activity of rivaroxaban, as mea-sured by anti-fXa activity, after incubation with varying amounts of r-Antidote. Inhibitory activity was dose-dependently and com-pletely reversed by r-Antidote in both human and rat plasma (data not shown). We next used rivaroxaban as a prototype inhibitor to test the effects of r-Antidote on markers of anticoagulation as measured
a 1
1
41
41 46 78 79 179 235 488
ANSFL RKRRKR
PrePro
PrePro
LC
Deletion
179 183 235
HC
HC
(Ser419)
(S419A)
488
fX
r-Antidote
RKR AP
pd-fXa r-AntidoteMW
(kDa)
188
MKb
98624938281714
HC ( , )
LC
LC
6
4
Figure 1 Design of r-Antidote and protein expression in CHO cells. (a) Schematic illustration of the domain structure of full-length human fX and r-Antidote (PRT064445) precursors. Using fX as a template, modifications were made in three regions to generate r-Antidote: deletion of a 34-residue fragment (residues 46–78) that contains the 11 GLA residues; replacement of the activation peptide (AP) with ArgLysArg (RKR) to form the RKRRKR linker that connects the light chain (LC) to the heavy chain (HC); and mutation of the active-site serine to alanine (S419A). Arrows indicate potential cleavage sites. (b) Reduced SDS-PAGE of purified r-Antidote showing bands of expected molecular weight (MW) for the light (~11 kDa) and heavy (~28 kDa) chains. The double bands of the heavy chain of plasma-derived fXa (pd-fXa) and r-Antidote correspond to the - and -isoforms. MK, molecular weight marker.
500,000c
400,000
300,000
200,000
100,000
0
0 1,000EGR-Xa or r-Antidote (nM)
lla fo
rmat
ion
(RF
U)
2,000 3,000
b25
1.5
1.0
0.5
0
20
15
5
10PT
(s)
Ratio
0
PPP 038
076
01,1
401,5
201,9
001,9
00
r-Antidote (nM)
100
75
50
Rat
e (m
OD
min
–1)
25
0
a
0 50 100 150 200r-Antidote (nM)
Betrixaban
[I] = 0 nM[I] = 2.5 nM[I] = 5.0 nM[I] = 7.5 nM
250 300
Rat
e (m
OD
min
–1)
100
75
50
25
0
Rivaroxaban
0 50 100 150 200r-Antidote (nM)
250 300
[I] = 0 nM[I] = 2.5 nM[I] = 5.0 nM[I] = 7.5 nM
Rat
e (m
OD
min
–1)
100
75
50
25
0
Apixaban
0 50 100 150 200r-Antidote (nM)
250 300
[I] = 0 nM[I] = 2.5 nM[I] = 5.0 nM[I] = 7.5 nM
Figure 2 r-Antidote reverses the inhibitory activity of three direct fXa inhibitors. (a) Dose-dependent reversal of betrixaban, rivaroxaban and apixaban inhibition in fXa enzyme assays. fXa activity was determined by the rate of peptide substrate cleavage after incubation of r-Antidote (0–250 nM) at room temperature for 30 min with the indicated concentrations of inhibitors ([I]). The curves drawn represent the best fits with the Kd and Ki values listed in Table 1. mOD, milli optical density. (b) Reversal of the prolongation of prothrombin time (PT) produced by rivaroxaban in human plasma after incubation of rivaroxaban (1 M) with different concentrations of r-Antidote at room temperature for 30 min before initiation of the assay. Gray bar, control plasma alone (PPP); filled bars, rivaroxaban or rivaroxaban plus r-Antidote; open bar, control plasma plus r-Antidote. n = 2–10. Error bars, s.d. (c) Effects of EGR-Xa and r-Antidote on prothrombinase activity. Human plasma was incubated with increasing concentrations of r-Antidote (squares) or EGR-Xa (circles) for 30 min at room temperature. Thrombin generation (IIa formation) was then initiated by the addition of Ca2+ and tissue factor, and cleavage of the thrombin-specific substrate Z-GlyGlyArg-aminomethylcoumarin (Z-GGR-AMC; relative fluorescence units, RFU) was measured at 37 °C for 10 min.
Lu G et al. Nature Med 2013; 19: 446- 453

Folie 45
Apixaban reversal
A R T I C L E S
448 VOLUME 19 | NUMBER 4 | APRIL 2013 NATURE MEDICINE
by ex vivo clotting assays. r-Antidote reversed the anticoagulant effect of rivaroxaban in human plasma (Fig. 2b). At a near-peak therapeu-tic concentration, rivaroxaban (1 M) caused a prolongation of pro-thrombin time. This prolongation was corrected to baseline by an approximately equal molar concentration of r-Antidote. Although r-Antidote bound and neutralized the anticoagulant effect of rivaroxa-ban in a dose-dependent manner, r-Antidote by itself did not change prothrombin time at the highest concentration tested (Fig. 2b). Thus, r-Antidote alone did not produce detectable amounts of procoagulant or anticoagulant activity as measured by this clotting assay.
As an additional test of the procoagulant or anticoagulant activity of r-Antidote, we used a thrombin generation assay, which tests fXa activity in the presence of cofactor factor Va and phospholipids in the prothrombinase complex. r-Antidote lacks the GLA domain and should have a substantially reduced capacity to incorporate into the prothrombinase complex. In contrast, active site–inhibited fXa with an intact GLA domain is expected to be a potent anticoagu-lant, as it can compete with endogenous fXa for assembly into the prothrombinase complex. We compared the effect of r-Antidote on prothrombinase activity with that of EGR-Xa, an active site–inhibited full-length human fXa. We measured prothrombinase activity by thrombin generation in human plasma with increasing concentra-tions of r-Antidote (0–3.3 M) or EGR-Xa (0–0.5 M). Formation of thrombin (as measured by relative fluorescence units) in the presence of r-Antidote remained essentially unchanged up to a concentration of 3.3 M, whereas EGR-Xa showed potent inhibition in the same assay (half-maximal inhibitory concentration of 26 nM) (Fig. 2c). These results are consistent with an earlier report documenting inhibition of prothrombinase activity by active site–inhibited native fXa16.
We next tested the ability of r-Antidote to reverse the anticoagulant effect of three direct fXa inhibitors in vivo in a rat model. Infusion of rivaroxaban (0.25 mg per kg body weight h!1) over a 30-min period produced a twofold increase in the level of anticoagulation as mea-sured by whole-blood INR (international normalized ratio) (Fig. 3a). After rivaroxaban infusion was stopped, rats were treated with vehicle
or were given an intravenous (i.v.) bolus injection of r-Antidote (4 mg per rat) followed by sustained r-Antidote infusion (4 mg h!1). In the vehicle-treated group, INR values decreased gradually as a result of clearance of the circulating inhibitor. In contrast, in the r-Antidote-treated group, the raised INR was rapidly and completely reversed to baseline values, and this reversal was sustained.
We also evaluated the effect of r-Antidote administration on the pharmacokinetics of rivaroxaban (Supplementary Fig. 1). After i.v. administration of r-Antidote, the total rivaroxaban plasma concentra-tion increased immediately as a result of the redistribution of rivaroxa-ban from extravascular compartments. Despite the increase in total rivaroxaban concentration, the amount of free, non–protein bound rivaroxaban (the fraction responsible for anticoagulant activity) decreased to very low levels. Thus, a decrease in the free fraction of rivaroxaban correlated with the correction of whole-blood INR values. The plasma molar ratios of r-Antidote to rivaroxaban (total) during the experimental time course were 2.1 (35 min), 1.7 (60 min) and 1.3 (90 min). As the plasma molar ratio of r-Antidote to fXa inhibitor decreased during the time course, some reestablishment of anticoagulation was observed in the rats.
We next performed similar experiments testing the effects of r-Antidote after betrixaban and apixaban infusion into rats (Fig. 3b,c). As above, we collected serial blood samples to measure whole-blood INR values, plasma concentrations of r-Antidote and the total and free plasma fractions of the inhibitors. Both betrixaban and apixa-ban–mediated whole-blood INR increases were similarly reversed by r-Antidote. After i.v. infusion of the three fXa inhibitors (each admin-istered individually) for 30 min, the total plasma concentrations of rivaroxaban, betrixaban and apixaban were 1.4 0.4 M (mean s.d.), 0.2 0.01 M and 1.4 0.3 M, respectively, and the percentages of unbound inhibitor were 2.2% 0.8% (mean s.d.), 40% 7.2% and 1.5% 0.3%, respectively. After administration of r-Antidote, the total plasma concentrations of the inhibitors increased to 1.9 0.09 M, 2.0 0.4 M and 4.2 0.7 M, respectively, and the percentage of unbound inhibitor declined to 0%, 0.3% 0.1% and 0.05% 0.02%, respectively. Thus, for each of the three inhibitors, correction of prothrombin time by r-Antidote to near-normal values was associated with a reduction in the free fraction of the inhibitor.
r-Antidote restores hemostasis in animal models of blood lossTo evaluate whether effects of r-Antidote in reversing coagulation as measured by INR translates into a cessation of bleeding, we first tested the ability of r-Antidote to restore normal hemostasis in a mouse
Table 1 Affinity of r-Antidote for direct fXa inhibitorsInhibitor r-Antidote Kd (nM) fXa Ki (nM) Ref.
Betrixaban 0.53 0.01 0.117 13Rivaroxaban 1.53 0.22 0.400 14Apixaban 0.58 0.02 0.100 15
Kd (mean s.d.) values were calculated by nonlinear fitting of the kinetic data in Figure 2a with the reported Ki value for each inhibitor.
Figure 3 Sustained reversal of whole-blood INR by r-Antidote in rats treated with direct fXa inhibitors. (a) Whole-blood INR values (mean s.d.) in rats infused with rivaroxaban (0.25 mg per kg body weight h!1) or vehicle for 30 min and then treated with either vehicle or r-Antidote by i.v. bolus (4 mg) over 5 min plus infusion (4 mg h!1) for up to 90 min. Circles, vehicle + vehicle; squares, rivaroxaban + vehicle; triangles, rivaroxaban + r-Antidote. **P 0.01 compared to the r-Antidote treatment group determined by unpaired two-tailed t test. (b) Whole-blood INR values (mean s.d.) in rats infused with betrixaban (1 mg per kg body weight h!1) or vehicle and then treated with either vehicle or r-Antidote by i.v. bolus (6 mg) over 5 min plus infusion (9 mg h!1) for up to 90 min. Circles, vehicle + vehicle; squares, betrixaban + vehicle; triangles, betrixaban + r-Antidote. *P 0.02 compared to the r-Antidote treatment group determined by unpaired two-tailed t test. (c) Whole-blood INR values (mean s.d.) in rats infused with apixaban (0.5 mg per kg body weight h!1) or vehicle and then treated with either vehicle or r-Antidote by i.v. bolus (6 mg) over 5 min plus infusion (6 mg h!1) for up to 90 min. Circles, vehicle + vehicle; squares, apixaban + vehicle; triangles, apixaban + r-Antidote. *P 0.01 compared to the r-Antidote treatment group determined by unpaired two-tailed t test.
a5.5 4.0
Infusion ofrivaroxaban
Infusion ofbetrixaban
Infusion ofapixaban
Bolus plusinfusion of r-Antidote
Bolus plusinfusion of r-Antidote
Bolus plusinfusion of r-Antidote
Time (min) Time (min)0 030 35 60 90 3035 60 90
Time (min)0 30 35 60 90
b c
4.5
Who
le-b
lood
INR
Who
le-b
lood
INR
Who
le-b
lood
INR
3.5
2.5
1.5
3.5
3.0
2.5
2.0
1.5
4.5
4.0
3.5
3.0
2.5
2.0
1.5
** ** * * ** *
apixaban + r-Antidote
apixaban + vehicle
Lu G et al. Nature Med 2013; 19: 446- 453

Folie 46
Spezifische Inhibitoren
Unfraktioniertes Heparin – Protamin Vitamin-K-Antagonisten – Vitamin K/PPSB Apixaban/Rivaroxaban – rFXai
1
Dabigatran – α-dab2
1Lu G et al. Nature Med 2013; 19: 446- 453 2Schiele F et al. Blood prepublished online March 8, 2013; doi:10.1182/ blood-2012-11-468207

Folie 47
Dabigatran reversal
Schiele F et al. Blood prepublished online March 8, 2013; doi:10.1182/ blood-2012-11-468207
21
Figure 4
-20
0
25
50
75
100
125
0 5 10 15 20 25 30
Dabigatran infusion + aDabi-Fab 0.3 µmol/kg bolus
Vehicle + Vehicle
Dabigatran infusion, no aDabi-Fab
Vehicle + aDabi-Fab 0.3 µmol/kg bolus
Time (min)
Thro
mbi
n tim
e (s
econ
ds)
-20
10
15
20
25
30
35
0 10 20 30
Dabigatran infusion + aDabi-Fab 0.3 µmol/kg bolus
Vehicle + Vehicle
Dabigatran infusion, no aDabi-Fab
Vehicle + aDabi-Fab 0.3 µmol/kg bolus
Time (min)
aPTT
(sec
onds
)A B
For personal use only. at ULB BONN/ABT MNL on April 22, 2013. bloodjournal.hematologylibrary.orgFrom
Dabigatran infusion,
no aDabi-Fab Dabigatran infusion +
aDabi-Fab 0.3 µmol/kg
bolus
Folie 48
Direkte orale Antikoagulanzien
- Spezifische Antidots sind entwickelt. - Für den klinischen Einsatz noch nicht
verfügbar. è Alternativen sind erforderlich

Folie 49
Antagonisationsstrategien Kurzfristige Unterbrechung der antikoa- gulatorischen Wirkung durch: - ein Antidot - Elimination
forcierte Diurese - Dialyse - unspezifische Hämostyptika

Folie 50
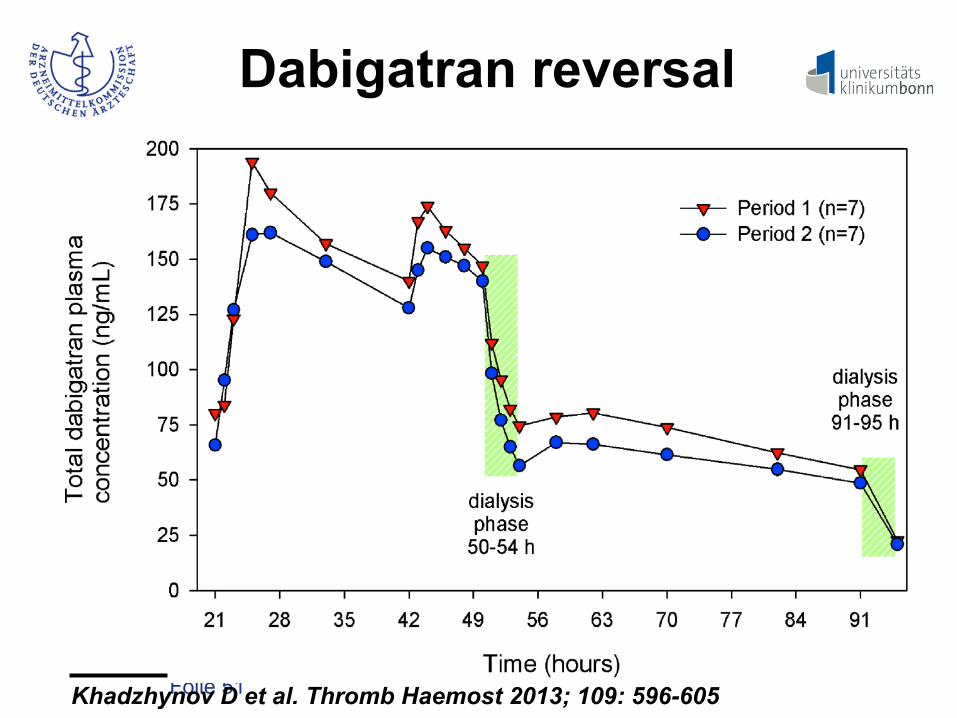
Dabigatran reversal
Khadzhynov D et al. Thromb Haemost 2013; 109: 596-605
© Schattauer 2013 Thrombosis and Haemostasis 109.4/2013
598
On Day 3, after the third DE was administered, a HD setting was employed that maximised elimination by selecting the largest and most adequate membrane available (based on dabigatran’s physic-chemical properties) and choosing the largest dialysate flow rate possible. This included a maximal dialysate flow rate of 700 ml/min and high flux filters with an extra-large surface of 2.1 m2 (PF-210H, Gambro). In the first dabigatran dosing and elimin-ation period, a blood flow rate of 200 ml/min was targeted. This flow rate reflects the clinical situation when a central venous ca-theter would be in place for potential use as an access port for HD and when blood flow rates up to 200 ml/min could reasonably be expected (“catheter setting”). During the second dosing and elim-ination period period, blood flow rates of 400 ml/min were tar-geted. This setting resembles the clinical situation in an ESRD pa-tient with an available dialysis shunt (“shunt setting”). If a blood flow of 400 ml/min could not be achieved, the maximal tolerable
blood flow was attained. In both catheter and shunt dialysis set-tings, a low-dose heparin anticoagulation scheme was used to en-sure effective HD while keeping the patients bleeding risk low (1,000 IU heparin bolus followed by 500 IU per hour; ! Figure 1).
On Day 5 of each dosing and elimination period, an “adapted” regular HD was performed. The adaptations compared to the regular HD on Day 1 comprised a dialysate flow of 700 ml/min, PF-210H dialyser and standard anticoagulation with heparin (2,000 IU bolus followed by 1,000 IU per h). Only the blood flow of 300 ml/min remained unchanged (! Figure 1).
Sample collection and analytical method
Twenty-six venous blood samples for PK and/or PD evaluations were taken through an indwelling catheter at baseline [pre-dose (0 h) on Day 1] and through 95 h post-dosing on Day 5. During the
Khadzhynov et al. Elimination of dabigatran during intermittent haemodialysis
Figure 1: Overview of study flow and summary of haemodialysis modalities.
For personal or educational use only. No other uses without permission. All rights reserved.Note: Uncorrected proof, prepublished online
Downloaded from www.thrombosis-online.com on 2013-04-19 | ID: 1000502741 | IP: 131.220.35.68
Folie 51
Dabigatran reversal
© Schattauer 2013 Thrombosis and Haemostasis 109.4/2013
600
ResultsPatient´s characteristicsSeven ESRD patients without atrial fibrillation were enrolled. All patients completed the study and all were included in all the phar-macokinetic, pharmacodynamic and safety evaluations. Study par-ticipants were male Caucasians with a mean age of 38.3 ± 10.9 years and mean BMI of 23.3 ± 2.3 kg/m2. Underlying renal dis-eases were chronic glomerulonephritis (five patients), polycystic kidney disease and Fabry’s Disease with renal involvement (one patient each). Medical histories of comorbidities were consistent with the diagnosis of ESRD and its secondary diseases (concomi-tant morbidities such as renal anaemia, secondary hyperparathy-reoidism etc.). The concomitant medication is listed in ! Table 1.
In Period 1, the target blood flow rate of 200 ml/min during the Day 3 HD session was achieved for all seven subjects. In Period 2, the maximal technically achieved blood flow rates during the Day 3 HD were in the range 350 to 395 ml/min (379 ± 10 ml/min), slightly lower than the targeted flow rate of 400 ml/min.
Pharmacokinetics of dabigatran before dialysis
Pharmacokinetic parameters for total dabigatran for Period 1 and 2 are summarised in ! Table 2. Plasma concentration - time pro-files were comparable between both Day 2 and 3 of each period and the first and second dosing period (! Figure 2). The fraction of glucuronide conjugated dabigatran was on average 31% of total dabigatran. Renal clearance of total dabigatran was less than 1 ml/min (CLR 0.60 and 0.58 ml/min in Period 1 and 2, respectively) as calculated in those ESRD patients with residual urine production.
Pharmacokinetics of dabigatran during haemodialysis
The effect of HD on the pharmacokinetic profile of total dabi-gatran is summarised in ! Table 3. HD of 4 h duration resulted in marked decreases in the dabigatran plasma concentrations from the start to the end of the dialysis session in both study periods (! Figure 2). The plasma fraction cleared from dabigatran reached a geometric mean (gMean) of 48.8% with a targeted blood flow of
Khadzhynov et al. Elimination of dabigatran during intermittent haemodialysis
Table 2: Pharmacokinetic parameters of total dabigatran after oral doses of dabi-gatran etexilate on Day 1 (150 mg), Day 2 (110 mg) and Day 3 (75 mg) (prior to hae-modialysis) in treatment periods 1 and 2. Full plasma concentration-time profiles were assessed on Day 2 and Day 3. *For tmax, median but no gCVs are shown. gCV, geo-metric coefficient of variation, range, min-max.
Treatment period 1 (n = 7)
Cmax, ng/ml
tmax*, h
AUC0–8 , ng*h/ml
Treatment period 2 (n = 7)
Cmax, ng/ml
tmax*, h
AUC0–8, ng*h/ml
Day 2
gMean
194
4.00
1230
171
6.00
1140
gCV [%]
53.1
57.1
36.2
39.4
range
103–439
4.00–12.0
578–2760
106–287
2.00–12.0
697–1980
Day 3
gMean
176
2.00
1280
159
2.00
1180
gCV [%]
54.1
54.4
50.2
50.2
range
99.6–398
1.00–2.00
764–3020
81.5–254
1.00–6.00
587–1940
Figure 2: Geometrical mean plasma concentration-time profiles of total dabi-gatran in both treatment periods. Dabi-gatran was administered at 0, 21 and 42 h after the first dose; dialysis was performed from 50 to 54 and 91 to 95 h.
For personal or educational use only. No other uses without permission. All rights reserved.Note: Uncorrected proof, prepublished online
Downloaded from www.thrombosis-online.com on 2013-04-19 | ID: 1000502741 | IP: 131.220.35.68
Khadzhynov D et al. Thromb Haemost 2013; 109: 596-605

Folie 52
DOA: Elimination - Dabigatran ist dialysierbar.
- In der Notfallsituation ist eine Dialyse-
behandlung meist schwierig zu realisieren. - Rivaroxaban/Apixaban sind nicht
dialysierbar.

Folie 53
Antagonisationsstrategien Kurzfristige Unterbrechung der antikoa- gulatorischen Wirkung durch: - ein Antidot - Elimination
forcierte Diurese - Dialyse - unspezifische Hämostyptika

Folie 54
Systemische Hämostyptika
- Prothrombinkomplexkonzentrat (PPSB) - Aktivierter Faktor VII (rFVIIa) - „factor VIII-bypassing activity“ (FEIBA)

Folie 55
DOA: clinical study
Regardless of the relative short half-life of these agents,immediate reversal of the anticoagulant effect may be neededin case of major bleeding or emergency surgery. No studies inhumans have assessed the ability of prohemostatic drugs toantagonize the anticoagulant effect of either rivaroxaban ordabigatran.13 Hypothetically, prothrombin complex concen-trate (PCC) could overcome the anticoagulant effect inducedby thrombin and factor Xa inhibitors because PCC containsthe coagulation factors II, VII, IX, and X in a high concen-tration and in general enhances thrombin generation. Inanimals, infusion with PCC reversed the effect of rivaroxa-ban.14 Unfortunately, results for dabigatran are not as clear-cut. In an animal bleeding model, PCC reversed the effect ofdabigatran on hemostatic parameters but had no effect oncoagulation assays.15 Another possible method of reversal isdialysis, although this is an invasive and burdensome proce-dure, and about one third of dabigatran is bound to plasmaproteins and can therefore not be dialyzed.3 Dialysis is alsonot suitable for rivaroxaban, which is 95% bound to protein.16
This study evaluated the possibility of using PCC toreverse the anticoagulant effect in a randomized, placebo-controlled, crossover trial in healthy volunteers who weretreated with dabigatran and rivaroxaban.
MethodsStudy DesignTwelve healthy male subjects were included in this randomized,double-blind, placebo-controlled, crossover trial. All gave writteninformed consent, and the study was approved by the medical ethicscommittee of the Academic Medical Center of Amsterdam, theNetherlands. The study was registered at the Dutch trial register(http://www.trialregister.nl; identifier, NTR2272). The 12 volunteersin this study first received either dabigatran or rivaroxaban for 21⁄2days. The last dose of the anticoagulant was taken on the third daywith no food consumption. On that third day, subjects were admittedto the hospital for infusion with either PCC or a similar volume ofsaline. Blood was then collected up to 24 hours after the infusion.After a washout period of 11 days, the healthy subjects received theother anticoagulant drug following the same protocol (Figure 1). Allvolunteers received financial compensation for the time spent on thestudy. Subjects were seen at the Clinical Trial Unit, which is anextension of the Cardiac Care Unit of the Academic Medical Centerin Amsterdam. Subjects were unblinded to the anticoagulant butblinded to placebo or Cofact. Technicians in the Department of
Experimental Vascular Medicine performed the laboratory analysesand were blinded to the treatment administered.
SubjectsHealthy volunteers without a relevant medical history were included.All subjects had normal blood count and normal kidney and liverfunction. All were tested and found to be negative for hepatitis B andC and HIV.
Study AgentsDabigatran (Pradaxa, Boehringer Ingelheim, Ingelheim, Germany)and rivaroxaban (Xarelto, Bayer, Leverkusen, Germany) are oralanticoagulants that act rapidly and reach steady-state levels almostimmediately after their initiation. Both drugs lose most of their effectwithin 24 hours; the half-life of dabigatran is 14 to 17 hours and ofrivaroxaban is 5 to 9 hours.17,18 Dabigatran was provided in capsulesof 150 mg twice daily for 21⁄2 days, similar to doses used for thetreatment of VTE or atrial fibrillation.7,19
Rivaroxaban tablets of 20 mg were given twice daily for 21⁄2 days,a regimen that is higher than the initial dose for the treatment of acuteVTE, which is 15 mg twice daily.5 The dose was chosen for practicalreasons: 15-mg and 5-mg tablets are not available yet.
Cofact (Sanquin Blood Supply, Amsterdam, the Netherlands) is anonactivated PCC derived from human plasma. It contains a highconcentration of the procoagulation factors II, VII, IX, and X, as wellas the natural anticoagulants protein C and S and antithrombin. Noheparin is added to Cofact. The specific activity of Cofact is based onthe level of factor IX.20 In this trial, a fixed dose of 50 U PCC/kgbody weight was chosen because the anticoagulant effect of rivar-oxaban and dabigatran on bleeding time in animal experiments wasreversed most effectively by the same amount (50 U/kg) of anotherPCC, Beriplex. Prothrombin complex concentrate is administeredintravenously, and any anticipated effect is seen immediately afterinfusion.21 Cofact 500 IU was reconstituted with 20 mL sterile waterbefore administration.
Blood Collection and ProcessingOn the day of admission, subjects were given 2 venous catheters: 1for the infusion of Cofact or placebo and 1 for the collection of bloodsamples. The catheter for blood samples was flushed with saline, andwhen blood was collected, the first 5 mL blood was discarded.Citrate tubes were used for blood samples and centrifuged at 15°Cfor 20 minutes at 1700g. Platelet-poor plasma was then prepared andcentrifuged at the same temperature for 15 minutes at 2000g andfrozen at !80°C before processing. Blood was drawn at baseline, onthe third day of anticoagulant treatment before infusion, and 15minutes, 30 minutes, and 1, 2, 4, 6, and 24 hours after infusion withCofact or placebo.
Figure 1. Flowchart of the study, a randomized, double-blind, placebo-controlled, crossover trial with healthy male subjects (n"12).
1574 Circulation October 4, 2011
Eerenberg et al, Circulation 2011; 124: 1573-1579

Folie 56
Rivaroxaban: PPSB
Eerenberg et al, Circulation 2011; 124: 1573-1579
information on the proper method to neutralize their antico-agulant activity. Findings from this study, the first conductedin humans, indicate that a nonactivated PCC immediatelyreverses the effect of full-dose rivaroxaban in healthy indi-viduals but not dabigatran at the PCC dose used in this study.
Prothrombin complex concentrate (Cofact) was chosen as amethod of reversal for both rivaroxaban and dabigatran forthe following reasons. It contains 4 coagulation factors,namely factors II (prothrombin), VII, IX, and X, that stimu-late thrombin formation, thereby potentially bypassing theanticoagulant effect of both drugs. The assessment of thereversal of the anticoagulant effects was based on coagulationassays shown to be sensitive in previous studies.16,22
Indeed, rivaroxaban influenced both the PT and ETPsignificantly. On the basis of these tests, the anticoagulanteffect of rivaroxaban was completely reversed immediatelyafter infusion of 50 U/kg PCC in all subjects, an effect that
persisted until the last measurement after 24 hours. Similarresults were previously obtained in a rat model with rivar-oxaban in which mesenteric bleeding times and coagulationassays (PT) were measured after administration of Beriplex, aPCC. The dose of 25 U Beriplex/kg body weight had noeffect on bleeding time, but 50 U Beriplex/kg body weightnormalized the bleeding time.14,21 A dose of 50 U/kg wastherefore chosen, but we cannot rule out that a lower dosemay have been sufficient. Results from the ETP show anincrease over time, suggesting perhaps a surplus of thrombingeneration. Nevertheless, these results are not seen immedi-ately after the infusion of PCC, and further research is neededto confirm the efficacy of a lower dose of PCC for thereversal of rivaroxaban.
The anticoagulant effect of dabigatran was monitored bythe aPTT, lag time of the ETP, TT, and ECT because theseassays seemed most sensitive to the direct thrombin inhibitor.
Figure 2. A, Effect of rivaroxaban followed by pro-thrombin complex concentrate (PCC) or placeboon the prothrombin time (PT; mean!SD). P"0.001for PCC, repeated measures ANOVA. B, Effect ofrivaroxaban followed by PCC or placebo on theendogenous thrombin potential (ETP; mean!SD).P"0.001 for PCC, repeated measures ANOVA.
1576 Circulation October 4, 2011

Folie 57
Dabigatran und PPSB
In particular, TT and ECT show linear dose-response curvesfor dabigatran.23 Dabigatran treatment clearly prolonged theaPTT, ETP lag time, TT, and ECT in all subjects. Subsequentadministration of 50 U/kg PCC had no effect on these assays.In a previous rat-tail bleeding model, Feiba (activated PCC)had no influence on an aPTT prolonged by dabigatran.However, Feiba reversed the bleeding time prolongationcaused by dabigatran.15 Furthermore, in a rabbit kidney injurybleeding model, Beriplex was able to dose-dependentlyreverse the prolonged bleeding time and the amount of bloodloss after dabigatran administration.26 This discrepancy be-tween the PCC effect on plasma coagulation assays andbleeding time raises the question of whether the coagulationtests adequately monitor the potential of PCC for reversal incases of bleeding associated with dabigatran. Coagulationassays are obviously only surrogate markers for a bleedingtendency. On the other hand, animal bleeding models may notbe representative of major hemorrhagic events in humans. On
the basis of the findings in the present study, at the PCC doseused in this study, there is no evidence to support the use ofPCC to neutralize the anticoagulant effect of direct thrombininhibitors. The question of how the effect of dabigatran canbe antagonized remains unanswered. A possible candidatemay be recombinant factor VIIa; this agent reduced the tailbleeding in the previously mentioned rat model with dabiga-tran. Recombinant factor VIIa, however, only partially re-stored the aPTT from 58!8 to 27!2 seconds (baseline aPTT,7!0.5 seconds).15 Additionally, a study using a single bolusof recombinant factor VIIa saw no reversal effect on mela-gatran, another direct thrombin inhibitor, based on aPTT,ETP, and other coagulation markers.27 A potential limitationof our study is that we used only 1 dose of 1 particular PCC.This does not exclude the potential of an alternative strategyfor reversal of dabigatran anticoagulation, eg, by repeatedlyadministering PCC, by administering recombinant factorVIIa, or by using a combination of PCC and recombinant
Figure 3. A, Effect of dabigatran followed by prothrombin complex concentrate (PCC) or placebo on the activated partial thromboplas-tin time (aPTT; mean !SD). P"0.21 for PCC, repeated measures ANOVA. B, Effect of dabigatran followed by PCC or placebo on thethrombin time (TT; mean!SD). P"0.36 for PCC, repeated measures ANOVA. C, Effect of dabigatran followed by PCC or placebo onthe ecarin clotting time (ECT; mean!SD). P"0.08 for PCC, repeated measures ANOVA.
Eerenberg et al PCC for Reversal of Rivaroxaban and Dabigatran 1577
Eerenberg et al, Circulation 2011; 124: 1573-1579

Folie 58
Dabigatran: mouse model
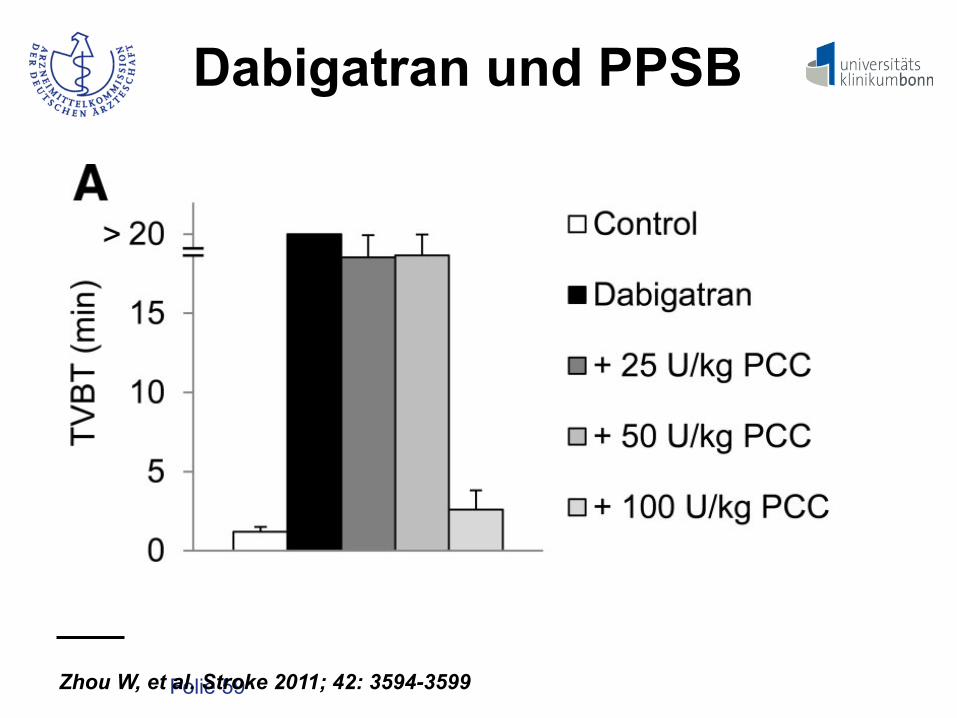
Zhou W, et al. Stroke 2011; 42: 3594-3599 TVBT, tail vein bleeding time
reached 6 hours after inducing ICH (Figure 3B). Interest-ingly, 77% of the maximal volume was already reachedwithin 1 hour and 86.7% within 3 hours. Thus, the majority ofexcess hematoma growth caused by DE in this modeloccurred in the first hour after collagenase injection. Hema-toma volume measured on MR T2* images and brain cryo-sections, respectively, correlated well (r!0.959; P"0.01),which is consistent with our previous report.16
Effect of Different Hemostatic Agents onHematoma Volume and MortalityTwenty-four hours after inducing ICH, mean hematomavolume in controls was 11.9#2.7 mm3 (Figure 4C). Pretreat-ment with DE 9.0 mg/kg increased the hematoma size to17.0#4.1 mm3. Hematoma growth could be effectively pre-vented by administering PCC (11.7#3.0 mm3; P"0.05),
whereas FFP (15.0#3.2 mm3) and FVIIa (17.9#4.7 mm3)failed to reduce hematoma expansion. In the second series ofexperiments (Figure 4D), hematoma size was 9.8#2.0 mm3
in controls. Pretreatment with 4.5 mg/kg DE increased thehematoma volume to 13.6#2.9 mm3 (P"0.01). Injectingeither FFP (9.3#1.8 mm3; P"0.001) or PCC (9.0#1.7 mm3;P"0.001) prevented hematoma growth. In contrast, FVIIadid not reduce hematoma size significantly (12.0#2.9 mm3).
The 24-hour mortality after ICH differed significantlyamong groups (Figure 4E). Approximately 5% of controlmice died within 24 hours. In contrast, the 24-hour mortalitywas 30% (P"0.05) in the anticoagulated mice that had notreceived any hemostatic agent. Only administrating PCCsignificantly reduced the 24-hour mortality (4%) to the levelof controls, whereas neither FFP (14%) nor FVIIa (15%) hadan impact on mortality.
Dose-Dependency of ProthrombinComplex ConcentrateAfter pretreatment with DE (9.0 mg/kg) for 1 hour, TVBTwas measured to assess whether the antagonistic effect ofPCC was dose-dependent. Here, 30 minutes after intravenousinjection of saline, TVBT exceeded 20 minutes. Compared withcontrols (1.2#0.3 minutes), TVBT in anticoagulated animalsreceiving 100 U/kg PCC was slightly prolonged (2.6#1.2minutes; P"0.01). Lower doses of PCC (25 or 50 U/kg) tendedto reduce TVBT, but some values were still beyond 20 minutes(Figure 5A).
Despite their different effects on TVBT, both 100 U/kg(10.2#2.2 mm3; P"0.05) and 50 U/kg (10.7#3.6 mm3;P"0.05) of PCC significantly reduced hematoma growthas compared to anticoagulated mice receiving saline(15.6#4.2 mm3; Figure 5B).
DiscussionDE recently has been approved for stroke prevention in AFand has potential to become a long-term preventive medica-tion for millions of patients with AF worldwide. However,despite its lower risk of hemorrhagic complications comparedto warfarin,4 lack of an antidote or an effective antagonist isa major concern in the event of severe bleeding, including
Figure 1. Effect of dabigatran-etexilate (DE) on systemic antico-agulation. A, Tail vein bleeding time (TVBT) was measured incontrol and anticoagulated mice at 1, 2, 4, 8, and 12 hours aftertreatment with 2.25, 4.5, or 9.0 mg/kg DE. Mean values of TVBT(n!3 per time point and experimental group) are depicted inminutes. TVBT was recorded for a maximum of 20 minutes(higher values were categorized as $20 minutes). B, Ecarin clot-ting time (ECT) was measured in control and anticoagulatedmice at 1, 2, 4, 8, and 12 hours after treatment (n!3 per timepoint and experimental group) with either 4.5 or 9.0 mg/kg DE.ECT is depicted in minutes and was measured for a maximumof 16.5 minutes (1000 seconds; higher values were categorizedas $16.5 minutes). C, Plasma levels of dabigatran were mea-sured in animals receiving either 4.5 or 9.0 mg/kg DE at 1, 2, 4,8, and 12 hours after treatment. Mean values (n!3 per timepoint and experimental group) are depicted as ng per mL.
Figure 2. Effect of different doses of dabigatran-etexilate (DE)on intracerebral hemorrhage (ICH) volume 24 hours after colla-genase injection. High doses of DE (4.5 or 9.0 mg/kg) exacer-bated ICH expansion. Hematoma volume was measured oncryosections at 24 hours after collagenase injection (n!7 pergroup). *P"0.05.
3596 Stroke December 2011
Folie 59
Dabigatran und PPSB
Zhou W, et al. Stroke 2011; 42: 3594-3599
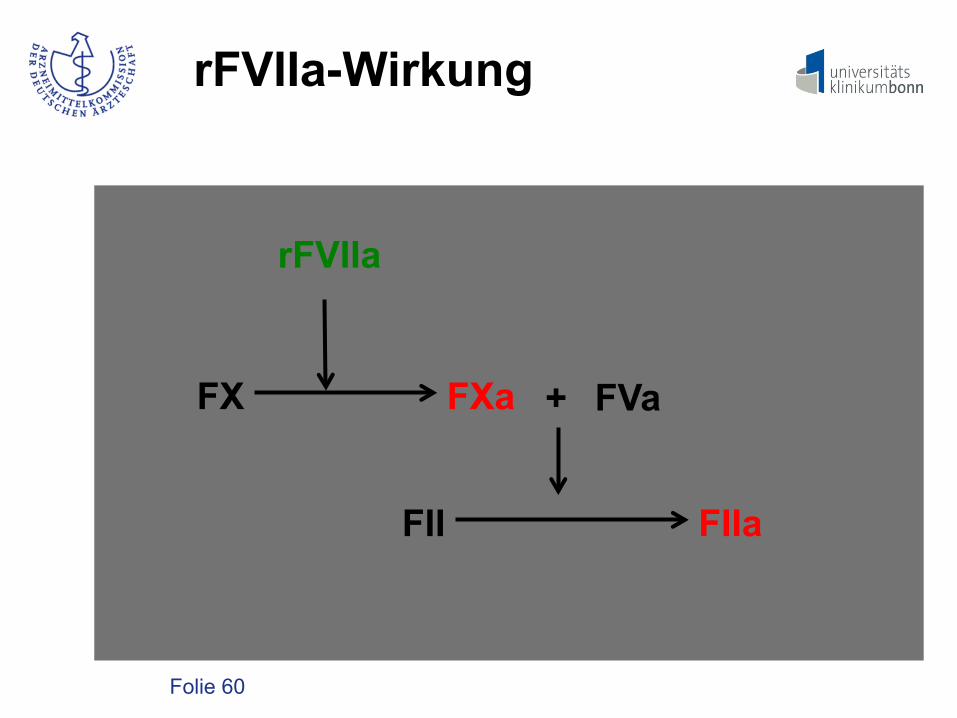
In contrast, FVIIa failed to reduce hematoma expansion inthe present experiments. Similar results were reported for thedirect thrombin inhibitor melagatran in an experimentalsystemic bleeding model.25 The dose of human FVIIa used inthe present study (8.0 mg/kg) was most effective in a murineexperimental study of hemophilia.26 Inefficiency of FVIIa inthe present study may result from its inability to counteractthe inhibitive effect of dabigatran on factor II.
The present study has strengths and limitations. Theefficacy of the different hemostatic agents was tested in 2independent experiments using 2 different doses of DE.Furthermore, the dose-dependent effect of PCC was shown inadditional experiments because PCC appeared most promis-ing in our synopsis of experimental and clinical evidence.Although in these studies 100 U/kg of PCC reversed theeffect of dabigatran on TVBT more effectively than 50 or 25U/kg, both 100 U/kg and 50 U/kg PCC prevented excesshematoma growth. However, we did not examine whetherlong-term treatment with lower doses of DE could causecomparable excess hematoma expansion in the event of ICH.
The mechanisms of how PCC prevents hematoma growthwere not examined. We speculate that administration of PCCor FFP increases the availability of factor II, which reconsti-tutes the coagulation cascade. Another limitation is that wedid not examine the neurological outcome. Finally, our studywas not designed to answer whether repeated administrationof coagulation factors is necessary in OAC-ICH associatedwith dabigatran in patients.
ConclusionsIn conclusion, we provide strong evidence that administeringPCC can prevent excess hematoma expansion in a murineOAC-ICH model associated with dabigatran. Because thepathophysiology of ICH in patients is only partially reflectedin current experimental ICH models, the efficacy and safetyof this strategy must be further evaluated in appropriateclinical studies.
AcknowledgmentsProthrombin complex concentrate (Beriplex) was a kind gift of CSLBehring, Germany.
Sources of FundingR.V. is supported by an Else-Kroner-Memorial Scholarship. S.I. issupported by a Deutscher-Akademischer-Austausch-Dienst (DAAD)Scholarship.
DisclosuresThe study was investigator-initiated. It was planned, performed, andfinanced independently of Boehringer Ingelheim, except for deter-mining dabigatran plasma levels, which were measured by a thirdparty under contract of Boehringer Ingelheim. Prothrombin complexconcentrate (Beriplex) was a kind gift of CSL Behring, Germany.
Figure 4. Effect of different hemostatic agents on hematomavolume 24 hours after collagenase injection. A, Experimentalprotocol of collagenase-induced intracerebral hemorrhage (ICH)in mice anticoagulated with dabigatran-etexilate (DE) and subse-quent hemostatic therapy with different hemostatic agents. B,Representative unstained cryosections of mice without antico-agulation with DE 9.0 mg/kg without antagonization, and withDE 9.0 mg/kg and 100 U/kg of prothrombin complex concen-trate (PCC) intravenously. Hematoma volume at 24 hours afteranticoagulation with (C) hematoma volume in mice receivingeither 9.0 mg/kg (n!12 per each group) or (D) 4.5 mg/kg DE(n!18 in saline treated group and n!10 in other groups) withdifferent hemostatic agents. E, Comparison of mortality in con-trols, mice anticoagulated with DE (4.5 and 9.0 mg/kg) with orwithout antagonization. *P"0.05.
Figure 5. Dose-dependency of antagonistic effect of prothrom-bin complex concentrate (PCC) in mice pretreated withdabigatran-etexilate (DE; 9.0 mg/kg). A, Comparison of tail veinbleeding time (TVBT) in control and anticoagulated mice (pre-treated with 9.0 mg/kg DE for 1 hour before receiving intrave-nously either saline or PCC) in different doses (25, 50, or 100U/kg; n!4 per each group). B, Comparison of hematoma vol-ume at 24 hours after collagenase injection in control and anti-coagulated mice with saline or PCC in different doses (25, 50, or100 U/kg; n!11 per each group). *P"0.05.
3598 Stroke December 2011
Folie 60
FX
FII
FVa
rFVIIa
FXa
FIIa
+
rFVIIa-Wirkung

Folie 61
FX
FII
FVa FXa
FIIa
+
FEIBA-Wirkung
FEIBA FEIBA

Folie 62
Dabigatran reversal: ex vivo
Marlu et al. Thromb Haemost 2012; 108: 217-224
bigatran (10). In the present study, rFVIIa at the higher dose, and FEIBA! corrected the altered LT to nearly baseline value. Neverthe-less, previous data regarding the effect of rFVIIa on thrombin in-hibitors are inconsistent. A single dose of rFVIIa did not reverse the anticoagulant effect of melagatran in healthy volunteers (27), al-though it did in another study (28). In a rat model, the addition of rFVIIa significantly reduced both tail bleeding time and aPTT after the administration of a high dose of dabigatran (29). Again, in ani-mal models, bleeding caused by a high dose of dabigatran was re-duced following the use of FEIBA! (29).
Clinical implications
If immediate reversal of the new anticoagulants is required, i.e. in the event of intra-cerebral haemorrhage, there is currently no clear evidence that any non-specific reversal agent can counteract the anticoagulant effect of either rivaroxaban or dabigatran.
FEIBA! has the theoretical advantage of combining the effect of FVIIa and that of PCC. Therefore, a dose of 50 U/kg FEIBA corre-sponds to 37 µg/kg of FVIIa together with 50 U/kg PCC (30). In the case of rivaroxaban, FEIBA combines the correcting effect on lag time of rFVIIa and the correcting effect on peak value of PCC. Higher doses of FEIBA were responsible for an increase in total thrombin generation, as shown by the increase in ETP-AUC and Peak. This raises the problem of safety of such a product regarding thrombotic risk. For this purpose, the incidence of thrombotic ad-verse events was reported as low, four per 100,000 FEIBA! infu-sions, and a dose-dependent effect on the incidence of thrombosis was reported (31). This underlines the need to avoid over-rever-sion, and to better define the potential minimum dose of reversal agent to use. Regarding TGT, quantitative parameters such as a Peak higher than 400 to 600 nM were correlated with thrombotic risk (32, 33). In our study for rivaroxaban, such an increase in thrombin generation above baseline H0 was not observed with FEIBA!. Moreover, it seems that the lower doses of FEIBA!, corre-sponding to a quarter and a half of the dose usually used, have
222 Marlu et al. Reversal of dabigatran and rivaroxaban
Thrombosis and Haemostasis 108.2/2012 © Schattauer 2012
Figure 4: Effect of non-specific reversal agents on dabigatran-anti coagulated plas-ma. Anticoagulant effect of dabigatran was measured by TGT. Data are mean relative change from H2 (i.e. 2 hours after 150 mg oral dabigatran, without reversal agent) ± SD. A) ETP-AUC denotes endogenous thrombin poten-tial (nM.min); B) LT is the lag time (s). Since thrombin peak was unchanged after dabigatran intake, results with reversal agents are not shown. Also since there is a strong correlation between LT and TTP, only results regarding LT were presented. H0: baseline; PCC: prothrom-bin complex concentrates (U/ml); rFVIIa: recom-binant FVIIa (µg/ml); FEIBA!: activated pro-thrombin complex concentrate (U/ml). All reagents are given at their final concentration. * p < 0.001 vs. H2; # was non-significant vs. baseline H0.
A
B
For personal or educational use only. No other uses without permission. All rights reserved.Downloaded from www.thrombosis-online.com on 2012-08-28 | ID: 1000502741 | IP: 131.220.35.99
Folie 63
DOA-Antidot: Fazit
- Ein spezifisches Antidot ist für keines der neuen DOA verfügbar.
- Dabigatran:
rFVIIa und FEIBA können den Wirkspiegel senken.
- Rivaroxaban/Epixaban:
PPSB kann wahrscheinlich die antikoagu- latorische Wirkung minimieren.

Folie 64
DOA: „minor bleeding“
- Wirkspiegelkontrolle - Therapiepause und/oder Dosisanpassung - lokale hämostyptische Maßnahmen

Folie 65
DOA: bedrohliche Blutung
- sofortige Unterbrechung DOA-Gabe - Monitoring DOA-Wirkung - lokale hämostyptische Maßnahmen Rivaroxaban: 50 IE/kg KG PPSB Dabigatran: 100 µg (5 KIE)/kg KG rFVIIa
oder 50 IE/kg KG FEIBA

Folie 66
- Ist ein Therapiemonitoring möglich? - Was tun bei Überdosierungen? - Was tun bei Interventionen? - Welche Kosten entstehen?
DOA: Fragen

Folie 67
- APTT < 1,3-fach verlängert, TZ < 60s: è gering erhöhtes Blutungsrisiko - APTT 1,3 – 2-fach verlängert, TZ > 60s: è erhöhtes Blutungsrisiko
Eingriffe mit niedrigem bis mittlerem Blutungsrisiko vertretbar
- APTT > 2-fach verlängert: è stark erhöhtes Blutungsrisiko
wenn med. vertretbar, Eingriff um 6-12 h verschieben
Dabigatran: Notfalleingriffe

Folie 68
- anti-FXa-Einheiten < 0,5: è gering erhöhtes Blutungsrisiko - anti-FXa-Einheiten > 0,5 - 1,0: è erhöhtes Blutungsrisiko
Eingriffe mit niedrigem bis mittlerem Blutungsrisiko vertretbar
- anti-FXa-Einheiten > 1,0: è stark erhöhtes Blutungsrisiko
wenn med. vertretbar, Eingriff um 6-12 h verschieben
Riva./Epixa.: Notfalleingriffe

Folie 69
DOA: Bridging
- Ein klassisches periinterventionelles Bridging von DOA ist nicht erforderlich.
- Eine an der HWZ orientierte präinter-
ventionelle Pause ist ausreichend. - Vorgehen vergleichbar mit LMWH.
Folie 70
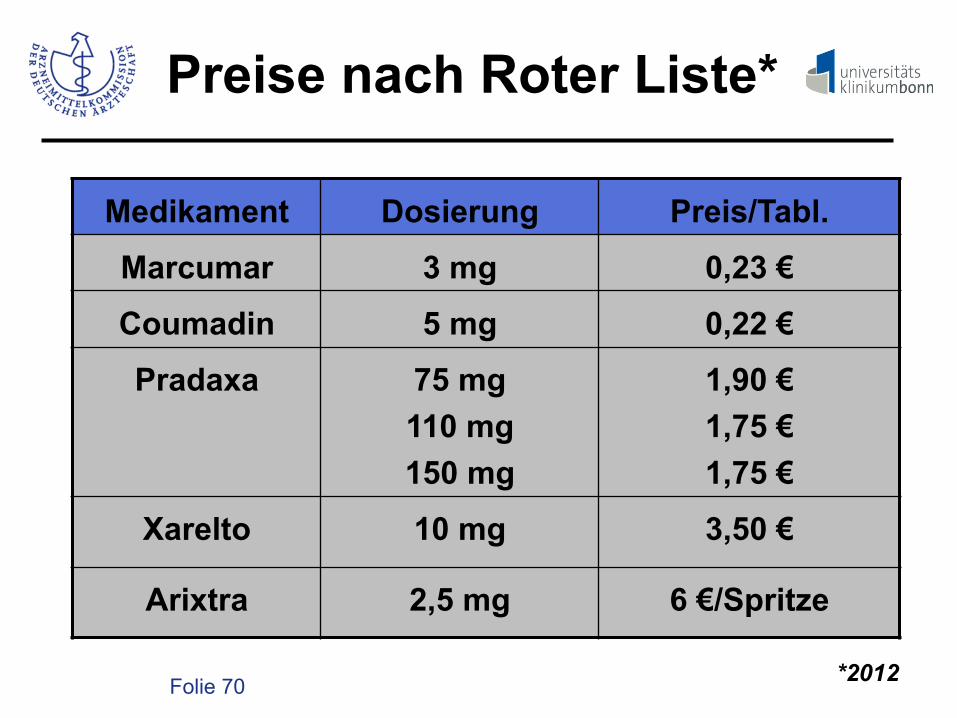
Preise nach Roter Liste*
Medikament Dosierung Preis/Tabl.
Marcumar 3 mg 0,23 €
Coumadin 5 mg 0,22 €
Pradaxa 75 mg 110 mg 150 mg
1,90 € 1,75 € 1,75 €
Xarelto 10 mg 3,50 €
Arixtra 2,5 mg 6 €/Spritze
*2012

Folie 71
- Welcher Patient mit VHF profitiert von den DOA, welcher profitiert nicht?
- Welcher Patient sollte mit DOA
behandelt werden?
DOA: Fragen

Folie 72
DOA: Umstellung
kardiale Indikation
VKA-Therapie
INR stabil?
VKA weiter DOA
ja nein

Folie 73
DOA: Neueinstellung
kardiale Indikation
schlechte Nierenfunktions- störung
VKA

Folie 74
DOA: Neueinstellung
kardiale Indikation
INR-Kontrolle nicht möglich
DOA

Folie 75
VHF: Antikoagulation
kardiale Indikation
Antikoagulation erforderlich
VKA DOA

Folie 76
VHF: Antikoagulation
kardiale Indikation
schlechte Compliance/ Demenz
VKA DOA

Folie 77
Fazit: 04/2013
- Rivaroxaban, Apixaban und Dabigatran ergänzen die Palette der oralen Antikoa- lanzien.
- Alle 3 Medikamente ermöglichen eine
effektive TE-Prophylaxe bei VHF. - Dabigatran 2 x 110 mg/Rivaroxaban 1 x 20 mg
sind unter Studienbedingungen der VKA- Therapie gleichwertig.

Folie 78
Fazit 04/2013
- Dabigatran 2 x 150 mg ist unter Studien- bedingungen der VKA-Therapie überlegen.
- Relevante Nebenwirkungen der DOA sind
Blutungen. - Ein klinisch verfügbares spezifisches Antidot
existiert nicht.

Folie 79
Fazit 04/2013
- Eine medizinische Indikation zum grundsätzlichen Ersatz von VKA durch DOA besteht nicht.
- Individuelle Faktoren (z. B. Lebensum-
stände, Blutungsrisiko) sind ausschlag- gebend für die Antikoagulanzienauswahl.

Folie 80
DOA: Indikationen
kardiale Indikation
VKA kontra- indiziert
gastro-intestinal cerebrales Risiko
DOA VKA