Malgrat Ambulatory Surgery Center - CAP - AIS (Arquitectura hosptalaria / health architecture)

\\H82017dc001\h82017-usf\~Dr's_Documents\RECEPTION\REGISTRATION NEW PATIENT PACK\word docs\1. Registration New Patient Welcome Letter.docx
Dr D W Holwell : Senior Partner Dr S R Fisher Dr M T Jahangir Dr C P M King Dr E M Fisher Dr T Loganathan Dr J Rattan Dr A Ergene Dr J Raphael Dr S Jethwa Dr I Wolff Dr E Jende Non principals: Dr D Potiphar Dr L Sherrington Dr S Slator Dr P Bugden Dr S Khan Dr S McCullough
Park Surgery
Albion Way Horsham
West Sussex RH12 1BG
Tel: 01403 330266 Fax: 01403 214639
www.parksurgery.com [email protected]
Dear Patient
Welcome to Park Surgery – please find enclosed your new patient information pack including some forms that
we would like you to complete to enable you to make the best use of the services that we provide:
1. Family doctor services registration form: complete as per the instructions with the form together
with the new patient health information questionnaire and alcohol screening test.
2. Accessible information standard form – this lets us know if you have any special communication needs.
3. Electronic prescription service – please complete so that we can send ALL your prescriptions to the
pharmacy of your choice.
4. Systmonline Application form – please complete to enable you to have access to online booking for
appointments, to request repeat prescriptions, send messages to the practice and view part of your
medical record (this last with GP authorisation).
5. Friends of Park Surgery – please complete if you would like to join FOPS to receive regular
newsletters and support the practice fundraising efforts for medical equipment. We hope you will be
happy with Park Surgery and welcome your comments and suggestions, via FOPS, to help us improve
what we do.
6. Summary Care Record Consent form – we would like your consent/dissent to share your SCR ie
name, address, medication and allergies with others services eg A&E or district nurses, should the
need arise.
7. Patient Experience – please do comment about the practice via www.iwantgreatcare.org or on NHS
Choices via their website www.nhs.uk/
8. We also enclose a copy of our practice brochure for your information and don’t forget to access our
website www.parksurgery.com for up to date news.
Kind regards
Paula Salerno
Practice Manager
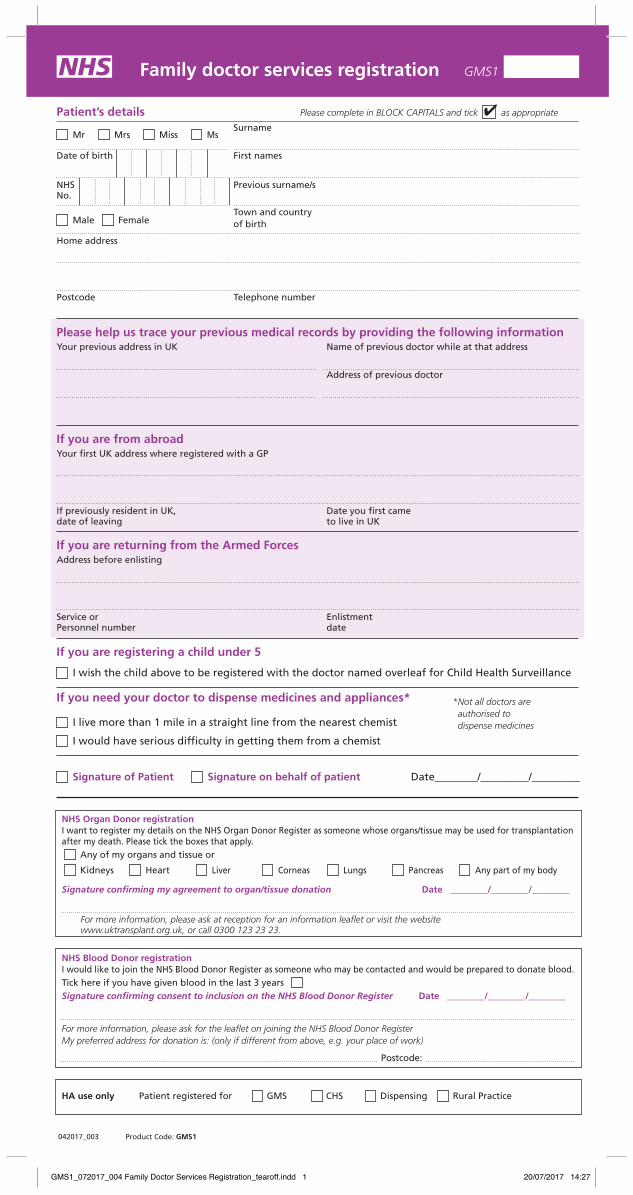
Family doctor services registration GMS1
Patient’s details Please complete in BLOCK CAPITALS and tick as appropriate
Surname
Date of birth First names
NHS Previous surname/sNo.
Male Female Town and country
of birth
Home address
Postcode Telephone number
Please help us trace your previous medical records by providing the following informationYour previous address in UK Name of previous doctor while at that address
Address of previous doctor
If you are from abroadYour first UK address where registered with a GP
If previously resident in UK, Date you first camedate of leaving to live in UK
If you are returning from the Armed ForcesAddress before enlisting
Service or EnlistmentPersonnel number date
If you are registering a child under 5
I wish the child above to be registered with the doctor named overleaf for Child Health Surveillance
If you need your doctor to dispense medicines and appliances*
I live more than 1 mile in a straight line from the nearest chemist
I would have serious difficulty in getting them from a chemist
Signature of Patient Signature on behalf of patient Date________/_________/_________
Mr Mrs Miss Ms
042017_003 Product Code: GMS1
* Not all doctors are authorised to dispense medicines
NHS Organ Donor registrationI want to register my details on the NHS Organ Donor Register as someone whose organs/tissue may be used for transplantation after my death. Please tick the boxes that apply.
Any of my organs and tissue or
Kidneys Heart Liver Corneas Lungs Pancreas Any part of my body
Signature confirming my agreement to organ/tissue donation Date ________/________/________
For more information, please ask at reception for an information leaflet or visit the websitewww.uktransplant.org.uk, or call 0300 123 23 23.
NHS Blood Donor registrationI would like to join the NHS Blood Donor Register as someone who may be contacted and would be prepared to donate blood.Tick here if you have given blood in the last 3 years Signature confirming consent to inclusion on the NHS Blood Donor Register Date ________/________/________
For more information, please ask for the leaflet on joining the NHS Blood Donor RegisterMy preferred address for donation is: (only if different from above, e.g. your place of work)
Postcode:
HA use only Patient registered for GMS CHS Dispensing Rural Practice
GMS1_072017_004 Family Doctor Services Registration_tearoff.indd 1 20/07/2017 14:27

Family doctor services registration GMS1
To be completed by the doctorDoctors Name HA Code
I have accepted this patient for general medical services For the provision of contraceptive services
I have accepted this patient for general medical services on behalf of the doctor named below who is a member of this practice
Doctors Name, if different from above HA Code
I am on the HA CHS list and will provide Child Health Surveillance to this patient or
I have accepted this patient on behalf of the doctor named below, who is a member of this practice and is on the HA CHS list and will provide Child Health Surveillance to this patient.
Doctors Name, if different from above HA Code
I will dispense medicines/appliances to this patient subject to Health Authority’s Approval
I am claiming rural practice payment for this patient. Distance in miles between my patient’s home address and my main surgery is
I declare to the best of my belief this information is correct and I claim the appropriate payment as set out in the Statement of Fees and Allowances. An audit trail is available at the practice for inspection by the HA’s authorised officers and auditors appointed by the Audit Commission.
Authorised Signature
Name Date _______/_______/_______
Practice Stamp
SUPPLEMENTARY QUESTIONS
PATIENT DECLARATION for all patients who are not ordinarily resident in the UKAnybody in England can register with a GP practice and receive free medical care from that practice.
However, if you are not ‘ordinarily resident’ in the UK you may have to pay for NHS treatment outside of the GP practice. Being ordinarily resident broadly means living lawfully in the UK on a properly settled basis for the time being. In most cases, nationals of countries outside the European Economic Area must also have the status of ‘indefinite leave to remain’ in the UK.
Some services, such as diagnostic tests of suspected infectious diseases and any treatment of those diseases are free of charge to all people, while some groups who are not ordinarily resident here are exempt from all treatment charges.
More information on ordinary residence, exemptions and paying for NHS services can be found in the Visitor and Migrant patient leaflet, available from your GP practice.
You may be asked to provide proof of entitlement in order to receive free NHS treatment outside of the GP practice, otherwise you may be charged for your treatment. Even if you have to pay for a service, you will always be provided with any immediately necessary or urgent treatment, regardless of advance payment.
The information you give on this form will be used to assist in identifying your chargeable status, and may be shared, including with NHS secondary care organisations (e.g. hospitals) and NHS Digital, for the purposes of validation, invoicing and cost recovery. You may be contacted on behalf of the NHS to confirm any details you have provided.
Please tick one of the following boxes:
a) I understand that I may need to pay for NHS treatment outside of the GP practice
b) I understand I have a valid exemption from paying for NHS treatment outside of the GP practice. This includes for example, an EHIC, or payment of the Immigration Health Charge (“the Surcharge”), when accompanied by a valid visa. I can provide documents to support this when requestedc) I do not know my chargeable status
I declare that the information I give on this form is correct and complete. I understand that if it is not correct, appropriate action may be taken against me.A parent/guardian should complete the form on behalf of a child under 16.
Signed: Date: DD MM YY
Print name:Relationship to patient:
On behalf of:
Complete this section if you live in another EEA country, or have moved to the UK to study or retire, or if you live in the UK but work in another EEA member state. Do not complete this section if you have an EHIC issued by the UK.NON-UK EUROPEAN HEALTH INSURANCE CARD (EHIC), PROVISIONAL REPLACEMENT CERTIFICATE (PRC) DETAILS and S1 FORMS
Do you have a non-UK EHIC or PRC? YES: NO: If yes, please enter details from your EHIC or PRC below:
If you are visiting from another EEA country and do not hold a current EHIC (or Provisional Replacement Certificate (PRC))/S1, you may be billed for the cost of any treatment received outside of the GP practice, includingat a hospital.
Country Code:
3: Name
4: Given Names
5: Date of Birth DD MM YYYY
6: Personal Identification Number
7: Identification number of the institution
8: Identification number of the card
9: Expiry Date DD MM YYYY
PRC validity period (a) From: DD MM YYYY (b) To: DD MM YYYY
Please tick if you have an S1 (e.g. you are retiring to the UK or you have been posted here by your employer for work or you live in the UK but work in another EEA member state). Please give your S1 form to the practice staff.
How will your EHIC/PRC/S1 data be used? By using your EHIC or PRC for NHS treatment costs your EHIC or PRC data and GP appointment data will be shared with NHS secondary care (hospitals) and NHS Digital solely for the purposes of cost recovery. Your clinical data will not be shared in the cost recovery process.
Your EHIC, PRC or S1 information will be shared with The Department for Work and Pensions for the purpose of recovering your NHS costs from your home country.
GMS1_072017_004 Family Doctor Services Registration_tearoff.indd 2 20/07/2017 14:27
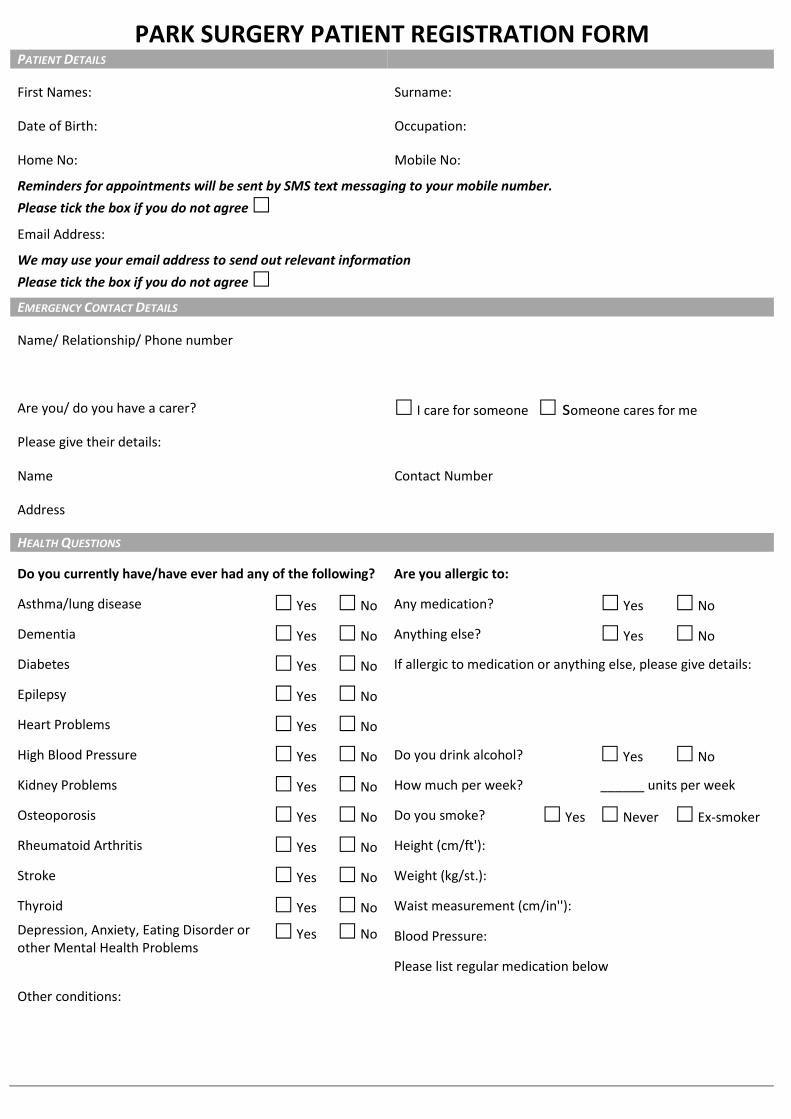
PARK SURGERY PATIENT REGISTRATION FORM PATIENT DETAILS
First Names: Surname:
Date of Birth: Occupation:
Home No: Mobile No:
Reminders for appointments will be sent by SMS text messaging to your mobile number.
Please tick the box if you do not agree
Email Address:
We may use your email address to send out relevant information
Please tick the box if you do not agree
EMERGENCY CONTACT DETAILS
Name/ Relationship/ Phone number
Are you/ do you have a carer? I care for someone someone cares for me
Please give their details:
Name Contact Number
Address
HEALTH QUESTIONS
Do you currently have/have ever had any of the following? Are you allergic to:
Asthma/lung disease Yes No Any medication? Yes No
Dementia Yes No Anything else? Yes No
Diabetes Yes No If allergic to medication or anything else, please give details:
Epilepsy Yes No
Heart Problems Yes No
High Blood Pressure Yes No Do you drink alcohol? Yes No
Kidney Problems Yes No How much per week? ______ units per week
Osteoporosis Yes No Do you smoke? Yes Never Ex-smoker
Rheumatoid Arthritis Yes No Height (cm/ft'):
Stroke Yes No Weight (kg/st.):
Thyroid Yes No Waist measurement (cm/in''):
Depression, Anxiety, Eating Disorder or other Mental Health Problems
Yes No Blood Pressure:
Please list regular medication below
Other conditions:
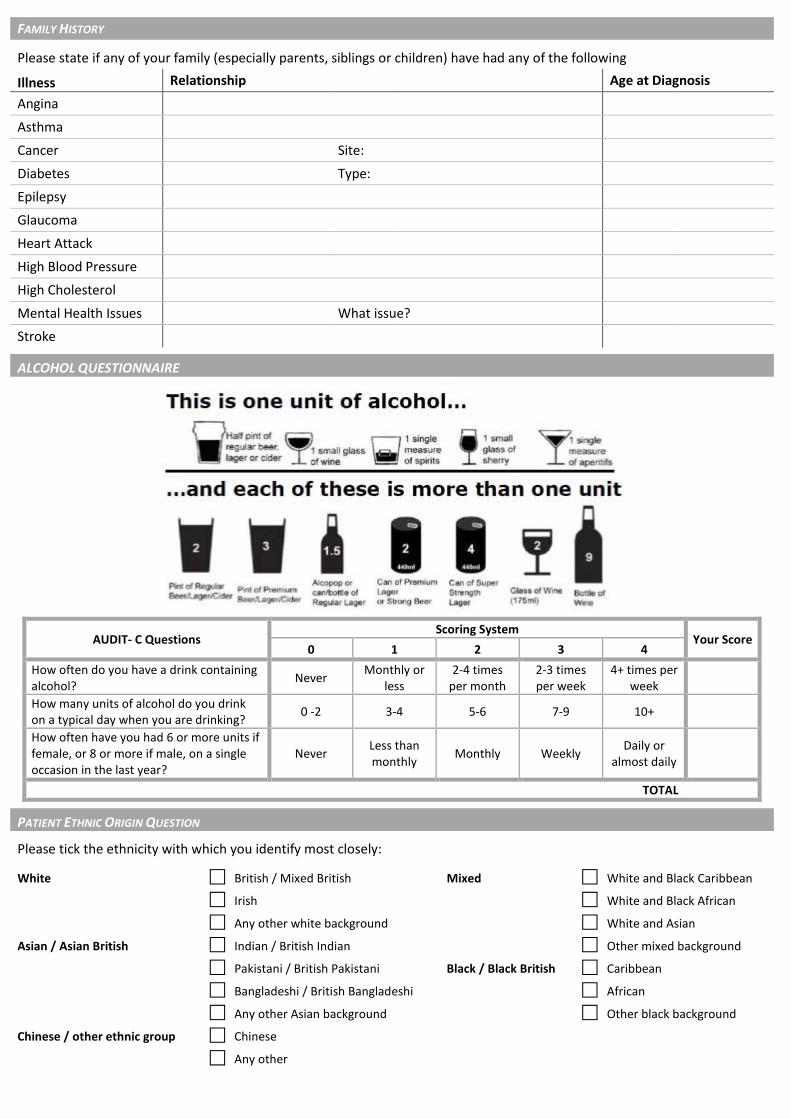
FAMILY HISTORY
Please state if any of your family (especially parents, siblings or children) have had any of the following
Illness Relationship Age at Diagnosis
Angina
Asthma
Cancer Site:
Diabetes Type:
Epilepsy
Glaucoma
Heart Attack
High Blood Pressure
High Cholesterol
Mental Health Issues What issue?
Stroke
ALCOHOL QUESTIONNAIRE
AUDIT- C Questions Scoring System
Your Score 0 1 2 3 4
How often do you have a drink containing alcohol?
Never Monthly or
less 2-4 times
per month 2-3 times per week
4+ times per week
How many units of alcohol do you drink on a typical day when you are drinking?
0 -2 3-4 5-6 7-9 10+
How often have you had 6 or more units if female, or 8 or more if male, on a single occasion in the last year?
Never Less than monthly
Monthly Weekly Daily or
almost daily
TOTAL
PATIENT ETHNIC ORIGIN QUESTION
Please tick the ethnicity with which you identify most closely:
White British / Mixed British Mixed White and Black Caribbean
Irish White and Black African
Any other white background White and Asian
Asian / Asian British Indian / British Indian Other mixed background
Pakistani / British Pakistani Black / Black British Caribbean
Bangladeshi / British Bangladeshi African
Any other Asian background Other black background
Chinese / other ethnic group Chinese
Any other
\ \ H 8 2 0 1 7 d c 0 0 1 \ h 8 2 0 1 7 - u s f \ ~ D r ' s _ D o c u m e n t s \ R E C E P T I O N \ R E G I S T R A T I O N N E W P A T I E N T P A C K \ 2 . H a n d o u t
f o r p a t i e n t s a c c e s s i b l e i n f o r m a t i o n . d o c x
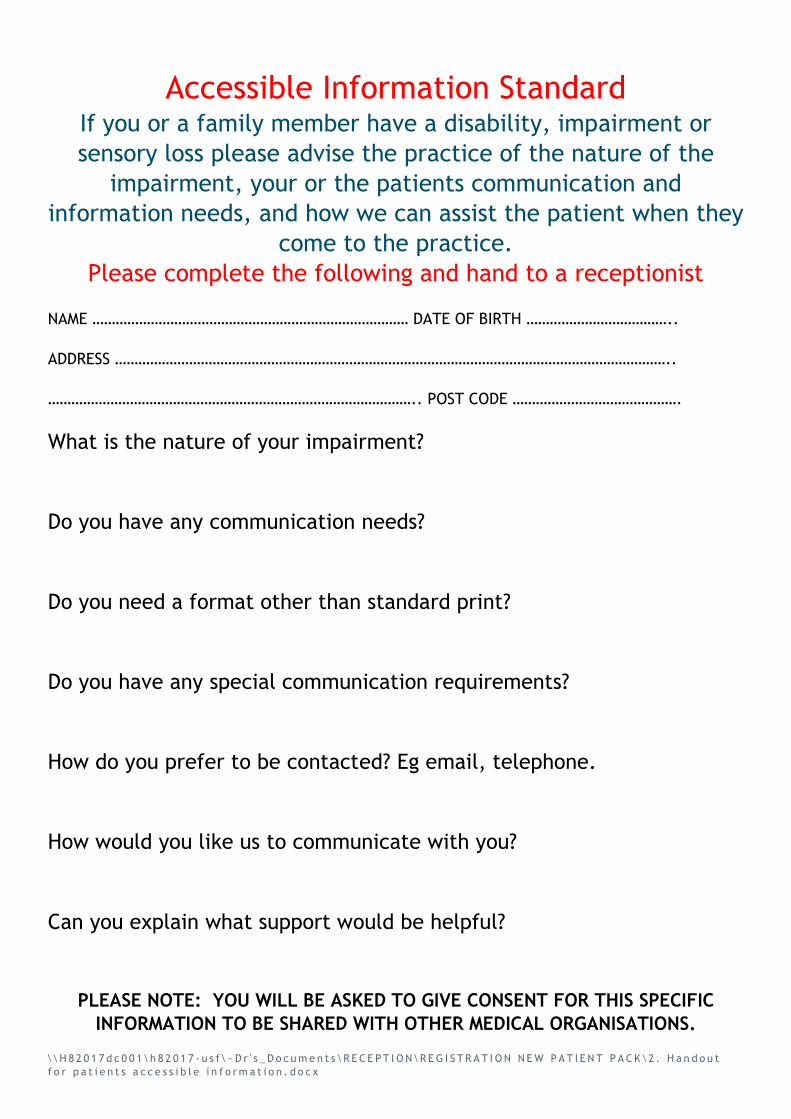
Accessible Information Standard If you or a family member have a disability, impairment or
sensory loss please advise the practice of the nature of the
impairment, your or the patients communication and
information needs, and how we can assist the patient when they
come to the practice.
Please complete the following and hand to a receptionist
NAME ……………………………………………………………………… DATE OF BIRTH ………………………………..
ADDRESS ……………………………………………………………………………………………………………………………..
………………………………………………………………………………….. POST CODE …………………………………….
What is the nature of your impairment?
Do you have any communication needs?
Do you need a format other than standard print?
Do you have any special communication requirements?
How do you prefer to be contacted? Eg email, telephone.
How would you like us to communicate with you?
Can you explain what support would be helpful?
PLEASE NOTE: YOU WILL BE ASKED TO GIVE CONSENT FOR THIS SPECIFIC
INFORMATION TO BE SHARED WITH OTHER MEDICAL ORGANISATIONS.
The Electronic Prescription Service (EPS) is a new NHS service.
It gives you the chance to choose ie ‘nominate’ the pharmacy the doctor should electronically send
your repeat and other prescriptions to.
What does this mean for you?
If you collect your repeat prescriptions from your GP you will no longer have to visit your GP
practice to pick up your paper prescription. Instead it will be sent electronically to the place
you choose.
You will have more choice about where to get your medicines from because they can be collected
from a pharmacy near to where you live, work or shop.
Is this service right for you?
Yes, if you have a stable condition and you:
don’t want to go to your GP practice every time to collect your repeat prescription.
collect your medicines from the same place most of the time or use a prescription collection
service now.
It may not be if you: ‘
do not need prescriptions very often.
pick up your medicines from different places.
How can you use EPS?
IF YOU HAVE NOT ALREADY DONE SO You need to choose a pharmacy for your GP practice to
electronically send your prescription to. This is called nomination. You can choose:
a pharmacy.
And a different dispensing appliance contractor (if you use one).
Ask any pharmacy or dispensing appliance contractor that offers EPS or your GP practice to add your
nomination for you. Some pharmacies have already started collecting nominations from patients and
your repeat prescription will automatically go to this pharmacy. If you are not sure whether or not
you have a nominated pharmacy recorded please check with your pharmacy.
Can I change my nomination or cancel it and get a paper prescription?
Yes you can. If you don’t want your prescription to be sent electronically tell your GP. If you want to
change or cancel your nomination speak to any pharmacist or dispensing appliance contractor that
offers EPS, or your GP practice. Tell them before your next prescription is due or your prescription
may be sent to the wrong place.
Is EPS reliable, secure and confidential?
Yes. Your electronic prescription will be seen by the same people in GP practices, pharmacies and
NHS prescription payment and fraud agencies that see your paper prescription now.
Sometimes dispensers may see that you have nominated another dispenser. For example, if you
forget who you have nominated and ask them to check or, if you have nominated more than one
dispenser. Dispensers will also see all the items on your reorder slip if you are on repeat
prescriptions.
For more information visit www.hscic.gov.uk/epspatients, your pharmacy or GP practice

Electronic Prescription Service
Patient Nomination Request
Patient name ………………………………………………………………………………………………
Address ………………………………………………………………………………………………………
……………………………………………………………………………………………………………………
Telephone Number.....…………………………………………………………………………………
DOB ………………….………………………………………………………………………………………..
NHS Number (if known)………………………………………………………………………………
I am the patient named above/carer of the patient named above. I confirm I have read and
understood the information about the EPS overleaf.
I NOMINATE THE FOLLOWING PHARMACY TO RECEIVE MY ELECTRONIC PRESCRIPTIONS UNTIL ADVISED
OTHERWISE—please tick
BOOTS Swan Walk DAY LEWIS –Park Surgery SAINSBURY’S
BOOTS Bartholomew Way DENNE—North Heath Lane SUPERDRUG
BOOTS Southwater NORIES TESCO
Rudgwick ROFFEY OTHER
PLEASE TAKE THIS FORM TO YOUR NOMINATED
PHARMACY
Patient Signature……………………….………………………………………..………………………
Date………………………………………………………………….…………………………….

PARK SURGERY - SYSTMONLINE ENHANCED APPLICATION FORM
You need to bring along some photographic proof of identification to become registered. To ensure confidentiality we are only able to accept registrations in person. Name………………………………………………………………………………………… Date of Birth……………………….……………….……… Email address…………………………………………………………………………… Mobile Number ……………………….…………………..
I wish to have access to the following online services (please tick all that apply):
Booking appointments
Requesting repeat prescriptions
Summary record
Accessing my detailed coded medical record
I wish to access my medical record online and understand and agree with each statement (tick)
I consent to receiving patient relevant information via email and SMS text messaging
I have read and understood the information leaflet provided by the practice
I will be responsible for the security of the information that I see or download
If I choose to share my information with anyone else, this is at my own risk
If I suspect that my account has been accessed by someone without my agreement, I will contact the practice as soon as possible
If I see information in my record that is not about me or is inaccurate, I will contact the practice as soon as possible
If I think that I may come under pressure to give access to someone else unwillingly I will contact the practice as soon as possible.
Signed……………………………………………………………………….……………………………… Date…………………………………………….
For Practice use only
ID verification will be required if patients are registering for online services for the first time
Photo ID Please state type of ID given
Vouching with information in record
Vouching
Identity verified by:

Friends of Park Surgery
Message from the Committee
July 2017 Charity No 1011608
Friends of Park Surgery is a group of enthusiastic people drawn from among patients with the spe-cific aim of helping to improve the life and work of the surgery. A strong committee is examining ideas on how best the Friends can operate but, above all, is seeking the active involvement of many more in-terested people from among the 24,000 patients. Our prime objectives are: • Education • Communication • Support These targets can be achieved in many ways, in-cluding making more information available, or-ganising talks by experts and arranging social and specific fund raising activities for state of the art equipment. We need your input to help us decide on the best way forward. If you are interested please spare us a few minutes to complete both sides of this form, which offers you the chance to put forward your own ideas and
WILL YOU JOIN US? 1. Would you be prepared to become involved in the activities of the Friends? YES / NO 2. Would you support informal talks by experts on health care matters? YES / NO 3. Would you support fund raising to buy equipment for the surgery? YES / NO 4. Would you be prepared to pay an annual donation of £5 per family? YES / NO 5. Have you any constructive ideas to improve the working of Park Surgery? (see over the page)
We need your help - please turn over the page.......
Please give us your ideas about improving the practice in the space below
PLEASE COMPLETE THESE DETAILS: Name __________________________________________ (Mr/Mrs/Miss) Address _______________________________________________________ _______________________________________________________ Email _______________________________________________________ Telephone _____________________________________________________
PLEASE RETURN THE FORM TO:
Tara Ledger Membership Secretary Friends of Park Surgery
Park Surgery, Albion Way Horsham, West Sussex RH12 1BG

1
Sharing Your Health Record We are writing to ask you for your permission to share some aspects of your health record with other organisations that may look after you, for example the district nursing team or the local hospital. What is your health record? Your health record contains all the clinical information about the care you receive. When you need medical assistance it is essential that clinicians can securely access your health record. This allows them to have the necessary information about your medical background to help them identify the best way to help you. This information may include your medical history, medications and allergies. Why is sharing important? Health records about you can be held in various places, including your GP practice, the district nurse community team and any hospital where you have had treatment. Sharing your health record will ensure you receive the best possible care and treatment wherever you are and whenever you need it. Choosing not to share your health record could have an impact on the future care and treatment you receive. Below are some examples of how sharing your health record can benefit you:
Sharing your contact details Ensures you receive any medical appointments without delay
Sharing your medical history Ensures emergency services accurately assess you if needed
Sharing your medication list Ensures that you receive the most appropriate medication
Sharing your allergies Prevents you being given something to which you are allergic
Sharing your test results Prevents further unnecessary tests being required
Is my health record secure? Yes. There are safeguards in place to make sure only organisations you have authorised to view your records can do so. You can also request information regarding who has accessed your information from both within and outside of your surgery. Can I decide who I share my health record with?
Yes. You decide who has access to your health record. For your health record to be shared between
organisations that provide care to you, your consent must be gained.
Can I change my mind? Yes. You can change your mind at any time about sharing your health record, please just let us know.
Park Surgery Albion Way
Horsham West Sussex
RH12 1BG Tel: 01403 330266 Fax: 01403 214639
www.parksurgery.com
Dr D W Holwell Senior Partner Dr S R Fisher Dr M T Jahangir Dr C P M King Dr E M Fisher Dr T Loganathan Dr J Rattan Dr E Jende Dr A Ergene Dr J Raphael Dr S Jethwa Dr I Wolff Non principals: Dr D Potiphar Dr L Sherrington Dr S Slator Dr P Bugden Dr S Khan Dr S McCullough

2
Can someone else consent on my behalf? If you do not have capacity to consent and have a Lasting Power of Attorney, they may consent on your behalf. If you do not have a Lasting Power of Attorney, then a decision in best interests can be made by those caring for you.
What about parental responsibility?
If you have parental responsibility and your child is not able to make an informed decision for
themselves, then you can make a decision about information sharing on behalf of your child. If
your child is competent then this must be their decision.
What is your Summary Care Record? Your Summary Care Records is used by many different computer systems and contains basic information including your contact details, NHS number, medications and allergies. If you do not want a Summary Care Record, please ask your GP practice for the appropriate opt out form. With your consent, additional information can be added to create an Enhanced Summary Care Record which will help improve your care. Enhanced SCRs include significant medical history and procedures, anticipatory care information, immunisations, and communication preferences.
For further information, please see: www.nhs.uk/NHSEngland/thenhs/records
Yours sincerely
Paula Salerno
Practice Manager

3
Sharing Your Health Record 1. Your Health Record Do you consent to your GP Practice sharing your health record with other organisations who care for you?
YES (recommended option)
No, except in an emergency No, never (not recommended, please discuss this with your GP before ticking this option)
Do you consent to your GP Practice viewing your health record from other organisations that care for you?
YES (recommended option)
No
2. Your Summary Care Record (SCR)
Do you consent to having an Enhanced Summary Care Record with Additional Information?
YES (recommended option)
No
Signature ______________________________________________________
Date: Signed on behalf of patient
Name: Date of Birth: