
Pathophysiologie der Sepsis Sylvia Knapp Klinik f. Innere Medizin 1 - Intensivstation 13i2 - Med....
27
Pathophysiologie der Sepsis Sylvia Knapp Klinik f. Innere Medizin 1 - Intensivstation 13i2 - Med. Univ. Wien
-
Upload
detlef-zell -
Category
Documents
-
view
108 -
download
3
Transcript of Pathophysiologie der Sepsis Sylvia Knapp Klinik f. Innere Medizin 1 - Intensivstation 13i2 - Med....

Pathophysiologie der Sepsis
Sylvia Knapp
Klinik f. Innere Medizin 1 - Intensivstation 13i2 - Med. Univ. Wien

Infektion, Sepsis & SIRS

Pathophysiologie der Sepsis
Riedemann et al. Nature Medicine 2003;9:517

Wheeler, N Engl J Med 1999
Ausgangspunkt- primäre Infektion & Sepsis
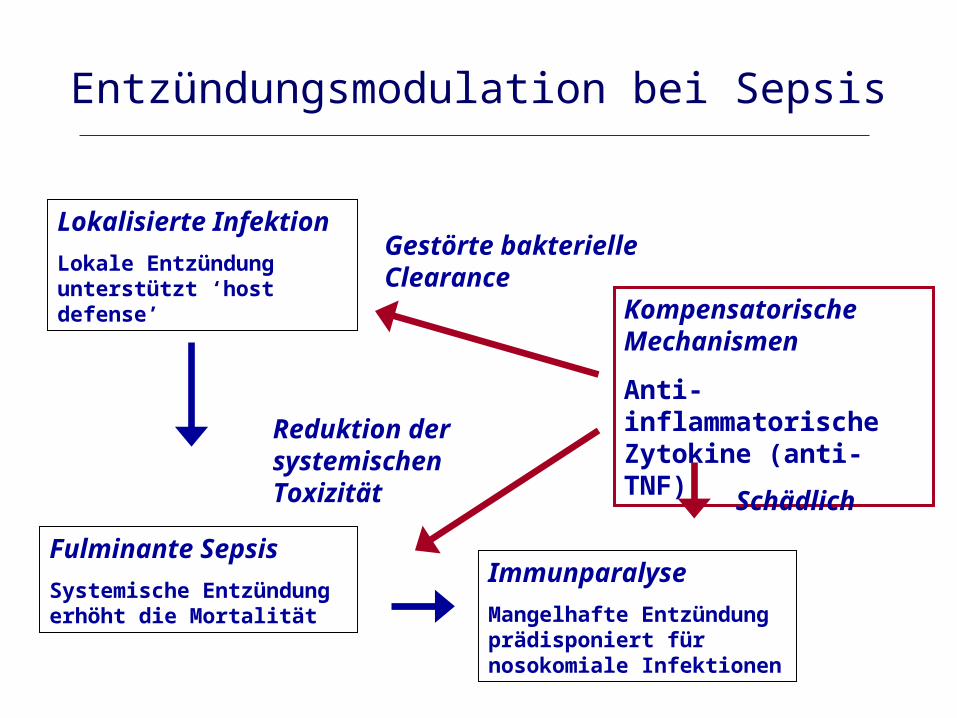
Lokalisierte Infektion
Lokale Entzündung unterstützt ‘host defense’
Fulminante Sepsis
Systemische Entzündung erhöht die Mortalität
Kompensatorische Mechanismen
Anti-inflammatorische Zytokine (anti-TNF)
Gestörte bakterielle Clearance
Reduktion der systemischen Toxizität
Entzündungsmodulation bei Sepsis
Immunparalyse
Mangelhafte Entzündung prädisponiert für nosokomiale Infektionen
Schädlich
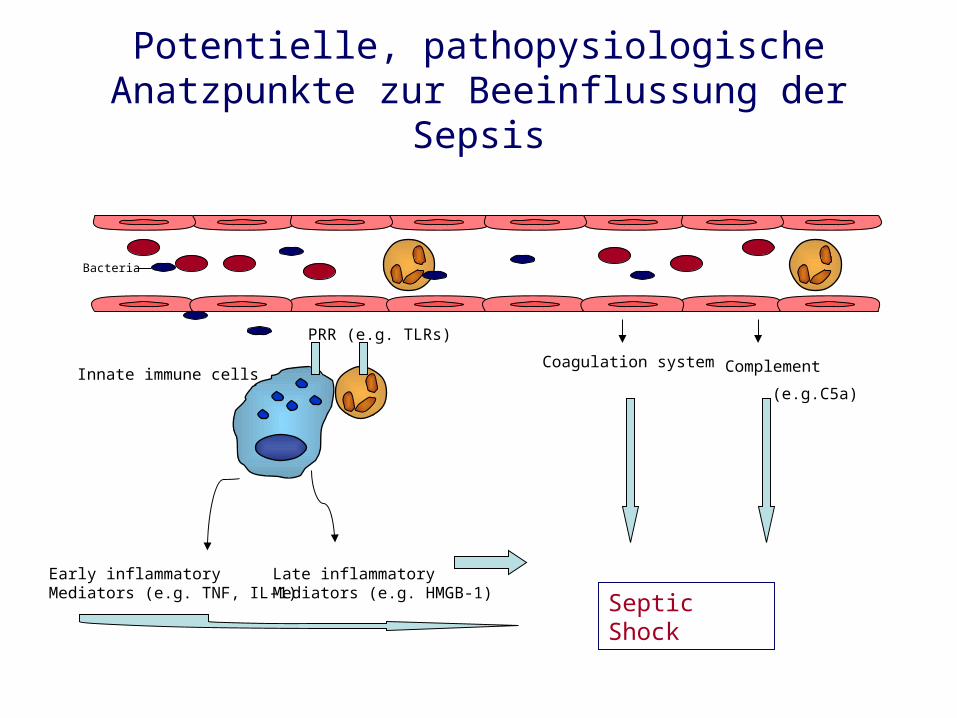
Potentielle, pathopysiologische Anatzpunkte zur Beeinflussung der Sepsis
Coagulation system
Septic Shock
Complement
(e.g.C5a)
Bacteria
Early inflammatory Mediators (e.g. TNF, IL-1)
Late inflammatory Mediators (e.g. HMGB-1)
Innate immune cells
PRR (e.g. TLRs)
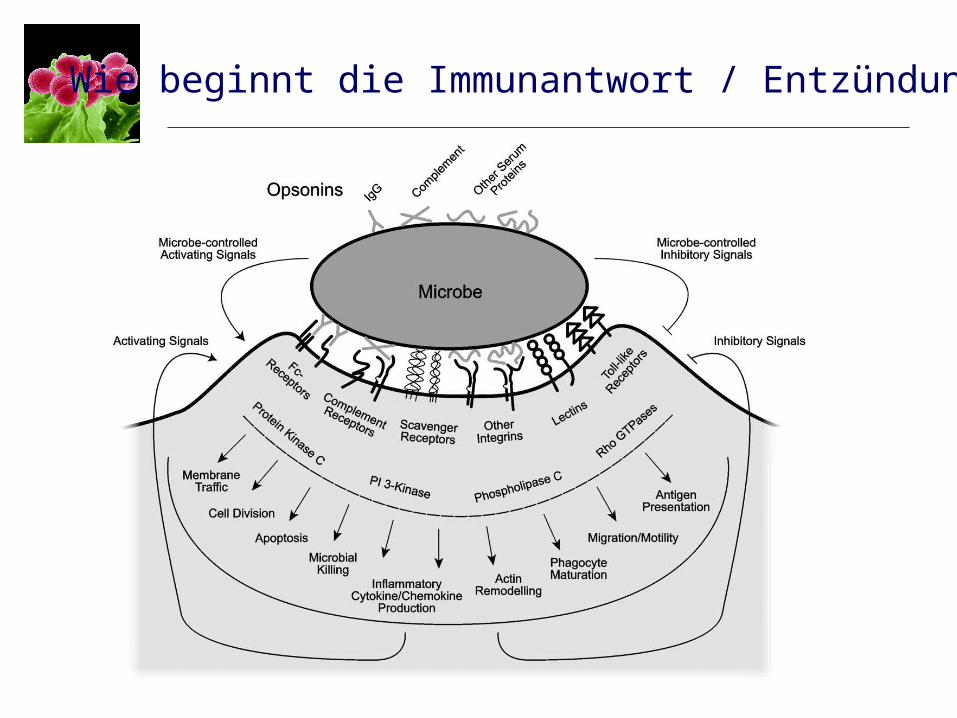
Wie beginnt die Immunantwort / Entzündung?

TLR4
TLR2CD14CD14 TLR5
TLR9TLR6
MyD88 IRAK
TRAF6
LPS
NFkBProinflammatorische Zytokine
Gram- BakterienGram+ Bakterien Viren
TLR1
TLR7
TLR3
TLR8
TLR10
Flagellin
dsRNA CpG
Imiquimod???
LTA
PGN
Lipopeptid
LAM
Zymosan
Toll-like Rezeptoren

Lipoprotein
Toll-like Rezeptor 2 (TLR2)
Zellwand Gram-positiver Bakterien
Peptidoglykan – TeichonsäureLipoteichonsäure

TLR2-blocking Antikörper reduziert die Entzündungsantwort gegen Gram+ Bakterien
controlLPS
Pam3CSK4
Bacillus subtilis
NF-B/p65 nuclear translocation
Meng et al. J. Clin. Invest. 2004; 113:1473
LPS: LipopolysaccharideLTA: Lipoteichoic Acid
Knapp et al. J. Immunol 2004; 172:3132

Anti-TLR2 verbessert Überleben bei Gram+ septischem Schock
Meng et al. J. Clin. Invest. 2004; 113:1473
0.5 – 1mg T2.5-0.5h T2.5
+1h: T2.5
0.25mg T2.5
Knapp et al. J. Immunol 2004; 172:3132
Wild type TLR2-/-

S. pneumoniae Pneumonie in TLR2-/-: Kein Einfluss auf Überleben
Knapp et al. J. Immunol 2004; 172:3132
Lunge: Bakterien
6h 48h
Überleben

Acinetobacter Pneumonie: TLR2 hemmtbakterielle Clearance via reduziertem PMN Einstrom
Knapp et al. AJRCCM 2006
3
4
5
6
7
8
9
*
* 4h 24h 44h
log
CF
U/m
l lu
ng
Wt TLR2-/-0
7000
14000
21000
28000
35000
*
MIP
-2 p
g/m
l lu
ng
Wt TLR2 -/-0
5
10
15
20
25
*
MP
O g
/ml
lun
g
Wt TLR2-/-
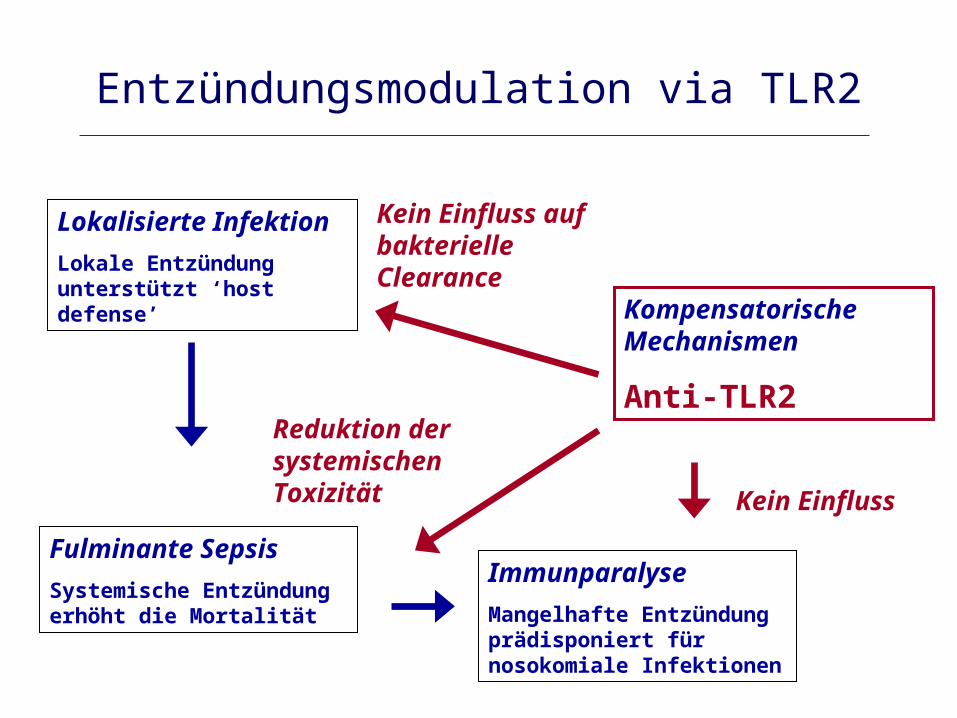
Lokalisierte Infektion
Lokale Entzündung unterstützt ‘host defense’
Fulminante Sepsis
Systemische Entzündung erhöht die Mortalität
Kompensatorische Mechanismen
Anti-TLR2
Kein Einfluss auf bakterielle Clearance
Reduktion der systemischen Toxizität
Entzündungsmodulation via TLR2
Immunparalyse
Mangelhafte Entzündung prädisponiert für nosokomiale Infektionen
Kein Einfluss

Disseminated Intravascular Coagulation (DIC) und Sepsis
Levi. NEJM 1999; 341:586

Konsequenz der DIC
Levi M. NEJM 1999; 341:586

Tissue factor/VIIa
Tissue factor/VIIa
VIIIa IXa
Va Xa
Thrombin
FibrinHemmt die Gerinnung
APC
TAFI
PAI-1
Profibrinolytisch
Angriffspunkte von aktiviertem Protein C
Inhibiert ‘rolling’
Inhibition der TNF Produktion APC

Long-term survival – APACHE II score
Angus DL et al. Crit Care Med 2004, 32:2199
33.8%
45.6%
P=.001
n.s.
52.1%
41.3%
P=.002
n.s.
Significantly improved hospital survivalNo difference in long-term survival
Significantly improved long-term survival when APACHEII >25 at baseline
Treatment effect depends on severity of illness

Rh APC improves outcome in Severe Community Acquired Pneumonia (CAP)
Laterre et al. Crit Care Med, 2005; 33:952
35,6% mit severe CAP
68.2%
61.2%
80%
67.1%% s
urv
iva
l
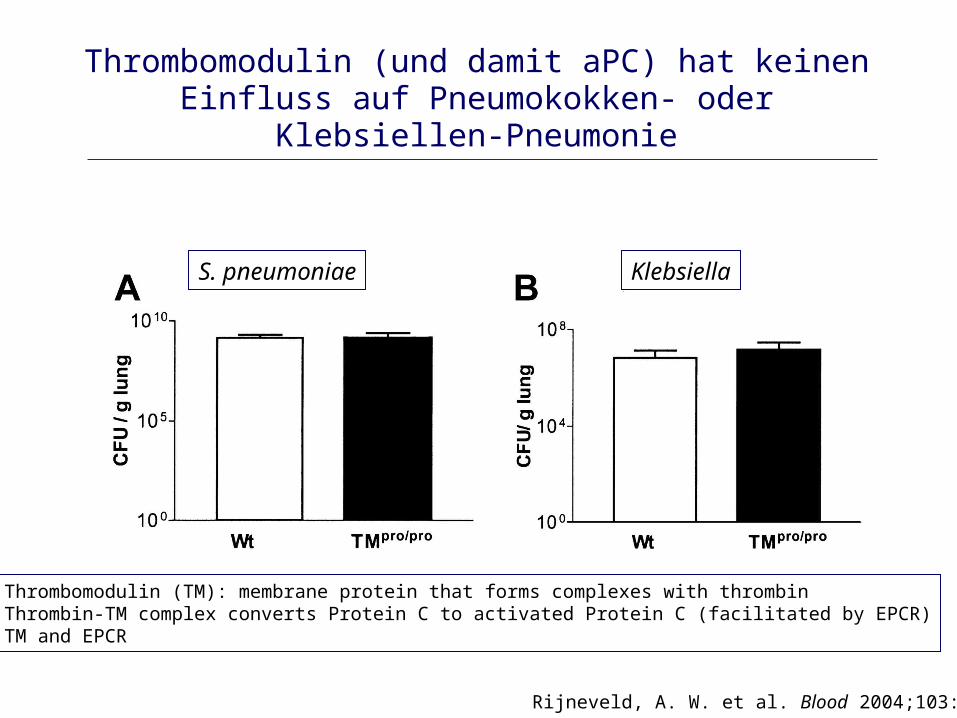
Thrombomodulin (und damit aPC) hat keinen Einfluss auf Pneumokokken- oder Klebsiellen-Pneumonie
Rijneveld, A. W. et al. Blood 2004;103:1702
S. pneumoniae Klebsiella
Thrombomodulin (TM): membrane protein that forms complexes with thrombinThrombin-TM complex converts Protein C to activated Protein C (facilitated by EPCR)TM and EPCR
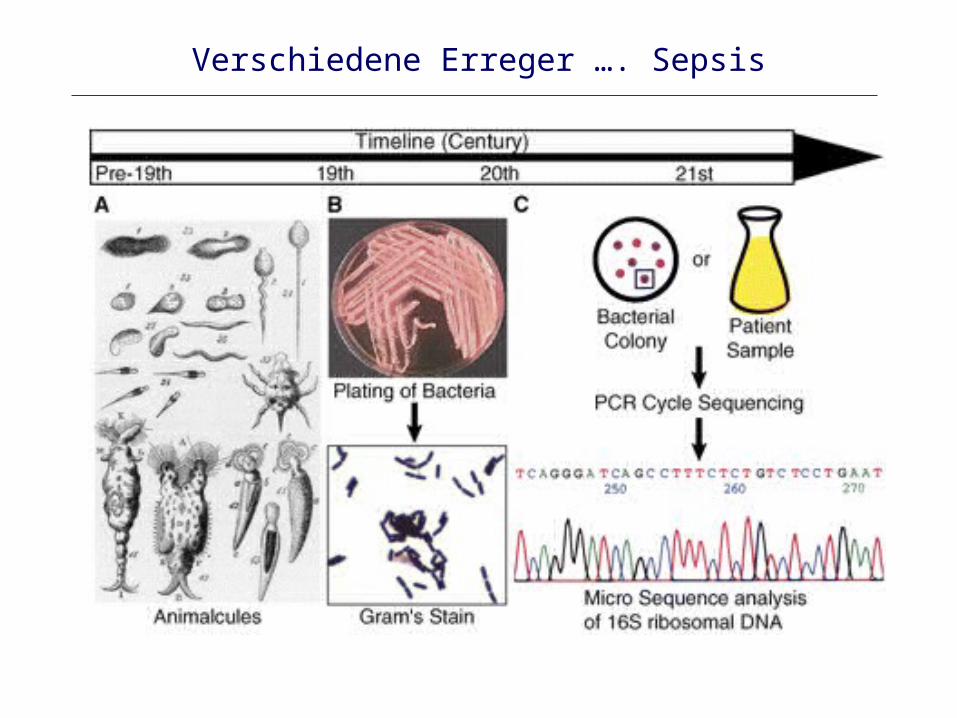
Verschiedene Erreger …. Sepsis
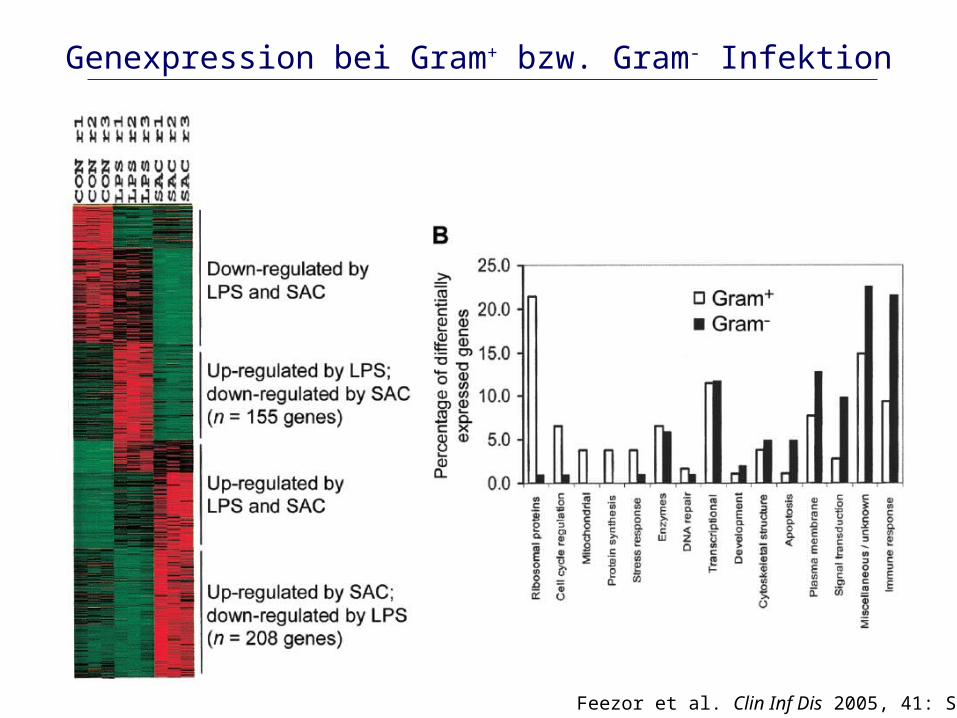
Feezor et al. Clin Inf Dis 2005, 41: S427
Genexpression bei Gram+ bzw. Gram- Infektion

Zytokin-Dynamik bei Endotoxämie
0 1 2 3 4 6 8 9
0
1000
2000
3000
4000
5000
IL-10TNFIL-6IL-8
0
200
400
600
800
time (h) after LPS iv
pg/m
lpg/m
l IL-10
4ng/kg LPS i.v.
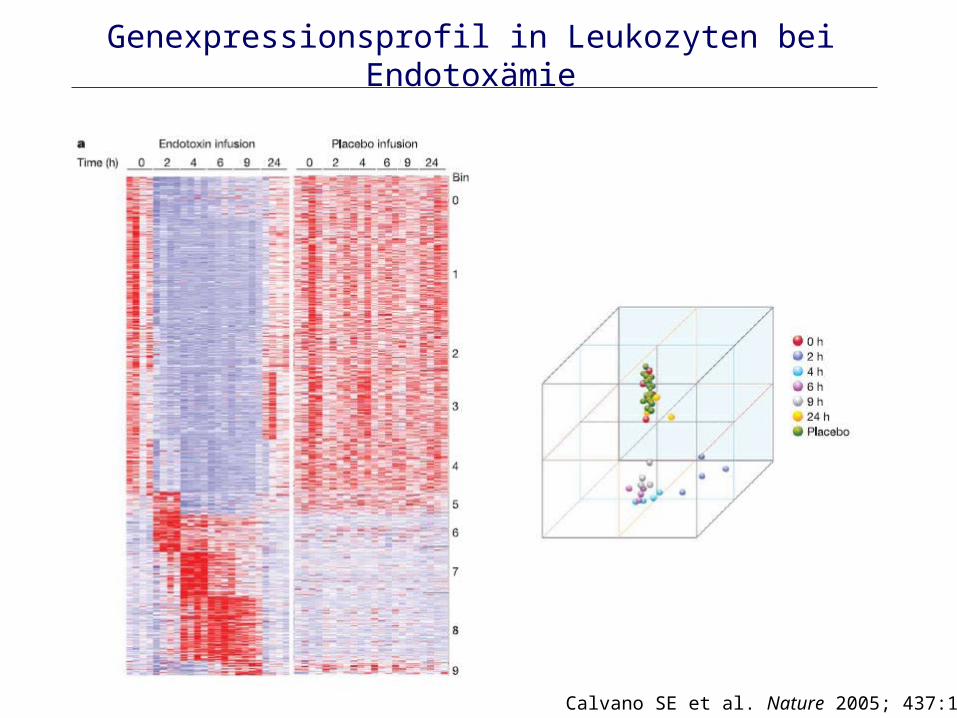
Calvano SE et al. Nature 2005; 437:1032
Genexpressionsprofil in Leukozyten bei Endotoxämie
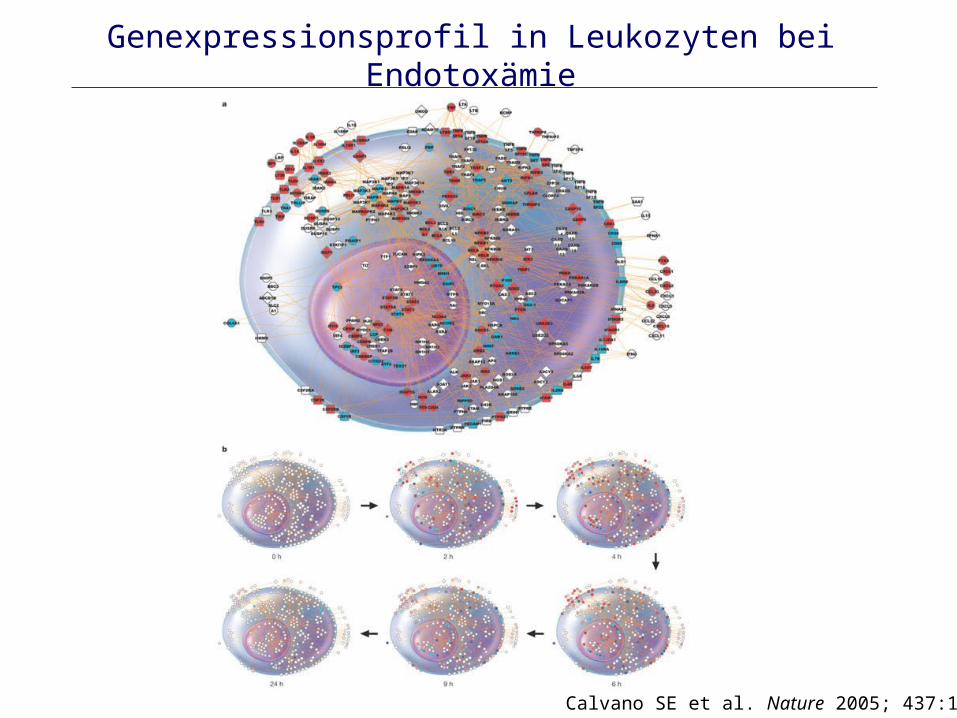
Genexpressionsprofil in Leukozyten bei Endotoxämie
Calvano SE et al. Nature 2005; 437:1032

www.gluegrant.org
Pseudomonas (nosokomial)
S. aureus
Pseudomonas (CF)
E. coli
Pro-inflammatorische Mediatoren
An
ti-in
flam
ma
toris
che
Me
dia
tore
n

Zukunft: Individualisierte, Patienten-bezogene Diagnose & Therapie
• 1. “Bedside tests”– Infektion oder SIRS?– Phase: Hyper- or Hypoinflammation?– Erreger?– Grunderkrankung?
• 2. Anti- or pro-inflammatorische Therapie?


















