Reanimation nach Traumap100527.typo3server.info/images/DIVIKongress/DIVI2015/03.12.2015... · m)...
81
Bundeswehrkrankenhaus Ulm Akademisches Krankenhaus der Universität Ulm Klinik für Anästhesie und Intensivmedizin Sektion Notfallmedizin Dr. Martin Kulla, DESA Dr. Martin Kulla, DESA Klinik für Anästhesiologie und Intensivmedizin Sektion Notfallmedizin Bundeswehrkrankenhaus Ulm Reanimation nach Trauma ...Zeit zum Umdenken!
Transcript of Reanimation nach Traumap100527.typo3server.info/images/DIVIKongress/DIVI2015/03.12.2015... · m)...

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Dr. Martin Kulla, DESA Klinik für Anästhesiologie und Intensivmedizin
Sektion Notfallmedizin
Bundeswehrkrankenhaus Ulm
Reanimation nach Trauma
...Zeit zum Umdenken!

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Einsatzmeldung Verkehrsunfall

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Einsatzmeldung: Verkehrsunfall

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Einsatzmeldung Verkehrsunfall

Aspekte der Traumareanimation
Fallberichte
Erfahrung
Misserfolge
Erkenntnisse
ZukünftigesPraktisches
Was ist im
Sinne des
Patienten?Ethik
Therapie Prähospital
Schockraum
InzidenzLeitlinien und
Literatur
Outcome
Maßnahmen
Algorithmen
Ursachen
Indikation und Abbruch

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Inzidenz
Ursachen des prähospitalen Herzkreislaufstillstandes in Australien
Deasy C, Bray J, Smith K et al. Traumatic out-of-hospital cardiac arrests in Melbourne,
Australia. Resuscitation 2012; 83: 465-470

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Ursachen des Kreislaufstillstands 2013 im deutschen
Reanimationsregister
0
10
20
30
40
50
60
70
kardial Trauma Ertrinken Hypoxie sonstiges
Chr. 22
gesamt
Deutsches Reanimationsregister - RTH Christoph 22

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Reanimation nach Trauma
Kein ROSC
Patient verstirbt

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
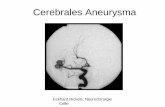
Reanimation nach Trauma
Verlauf
ROSC nach
Blutungskontrolle,
Volumentherapie
und unter offener
HDM
Durchschuss Aorta
abdominalis
Aortenersatz im SR
Tod: 6 Stunden post
OP auf ICU

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Reanimation nach Trauma
Notthorakotomie im Schockraum

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Reanimation nach Trauma

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Reanimation nach Trauma
Exsanguination
aufgrund
Mittelgesichtstrauma
Prähospital keine
Möglichkeit der
Blutstillung

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Reanimation nach Trauma
• ROSC nach Blutstillung
und Volumengabe
• Operative Versorgung

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Reanimation nach Trauma
„persönliche NNT aktuell 10“
NNH ???

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Reanimation nach Trauma
Rosemurgy AS, Norris PA, Olson SM, Hurst JM, Albrink MH. Prehospital traumatic cardiacarrest: the cost of futility. J Trauma 1993; 35: 468-473; discussion 473-464
12.462 Trauma
? (?%) OHCA
138 (?%) Trauma-
CPR
? (?%) ROSC
0 (0%) Überleben
Trauma patients who require CPR at the scene or in
transport die. Infrequent organ procurement does not
seem to justify the cost (primarily borne by hospitals),
consumption of resources, and exposure of health care
providers to occupational health hazards. The wisdom of
transporting trauma victims suffering cardiopulmonary
arrest at the scene or during transport must be
questioned

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
ERC Guideline 2010
Soar J, Perkins GD, Abbas G et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 8. Cardiac arrest in special circumstances: Electrolyte abnormalities, poisoning, drowning, accidental hypothermia, hyperthermia, asthma, anaphylaxis, cardiac surgery, trauma, pregnancy, electrocution. Resuscitation 2010; 81: 1400-1433

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
ERC Guideline 2015
Truhlar A et. al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 4. Cardiac arrest in
special circumstances. Resuscitation 95 148-201 (2015)

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Trauma-CPR
DSTC® Kurs – mit freundlicher Genehmigung von Sascha Flohé

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
CPR
Trauma-CPR
≠

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Autoren Section 4
a) Emergency Medical Services of the Hradec Králové
Region, Hradec Králové, Czech Republic
b) Department of Anaesthesiology and Intensive Care
Medicine, University Hospital Hradec Králové, Hradec
Králové, Czech Republic
c) Cardiac Anaesthesia and Cardiac Intensive Care, NIHR
Southampton Respiratory Biomedical Research Unit,
Southampton University Hospital NHS Trust,Southampton,
UK
d) Anaesthesia and Intensive Care Medicine, Southmead
Hospital, North Bristol NHS Trust, Bristol, UK
e) Emergency and Disaster Medicine, Six October University
Hospital, Cairo, Egypt
f) Departments of Renal and Internal Medicine, Victoria
Hospital, Kirkcaldy, Fife, UK
g) Society to Rescue People from Drowning, Amsterdam, The
Netherlands
h) Bergen Emergency Medical Services, Department of
Anaesthesia and Intensive Care, Haukeland University
Hospital, Bergen, Norway
i) EURAC Institute of Mountain Emergency Medicine, Bozen,
Italy
j) Department of Cardiothoracic Surgery, James Cook
University Hospital, Middlesbrough, UK
k) Center for Emergency Medicine, Clinical Hospital Center
Zagreb, Zagreb, Croatia
l) Department of Cardiology, Academic Medical Center,
Amsterdam, The Netherlands
m) Intensive Care Medicine and Anaesthesia, Southmead
Hospital, North Bristol NHS Trust, Bristol, UK
n) Department of Anesthesiology, University Medical Center,
Johannes Gutenberg-Universitaet, Mainz, Germany
o) Barts Heart Centre, St Bartholomew’s Hospital, Barts
Health NHS Trust, Queen Mary University of London,
London, UK
p) Department of Anaesthesiology and Critical Care Medicine,
University Hospital Innsbruck, Austria
q) Warwick Medical School, University of Warwick, Coventry,
UK
r) Critical Care Unit, Heart of England NHS Foundation Trust,
Birmingham, UK
s) Department of Anaesthesiology and Intensive Care,
Catholic University School of Medicine, Rome, Italy
t) Birmingham Children’s Hospital, Birmingham, UK
u) Department of Anaesthetics, Imperial College Healthcare
NHS Trust, London, UK
v) Anaesthesia and Intensive Care Medicine, Royal United
Hospital, Bath, UK
w) School of Clinical Sciences, University of Bristol, UK

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Collaborators Section 4
Intensive Care Medicine and Clinical Toxicology,Catholic University School of
Medicine, Rome, ItalyBernd
´Department of Anaesthesiology and IntensiveCare Medicine, University Hospital
of Cologne, Cologne, Germany
American Medical Center Nicosia, Cyprus
Honorary Consultant Physician, Colchester, UK
Department of Anaesthesiology and Intensive Care,Stavanger University Hospital,
Stavanger, Norway; Norwegian AirAmbulance Foundation, Drøbak, Norway
NIHR Surgical Reconstruction and Microbiology Research Centre, University of
Birmingham, UK
Emergency Medicine, Faculty of Medicineand Health Sciences, University of
Antwerp, Antwerp, Belgium / Faculty of Medicine and Health Sciences, University
of Ghent,Ghent, Belgium; Emergency Medicine, Ghent University, Ghent,
Belgium
Department of Anaesthesiology and IntensiveCare Medicine, University Hospital
of Cologne, Cologne, Germany

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
ERC Guideline 2015
There are no reliable predictors of survival for traumatic cardiac arrest.
A large systematic review reported an overall survival rate of 3.3% in blunt
and 3.7% in penetrating trauma, with good neurlogical outcome in 1.6% of
all cases
One study reported good neurological outcome in 36.4% of TCA patients
presenting with VF, but only in 7% with PEA and 2.7% of those in asystole...
For reasons that are unclear, reported survival rates in the last 5 years
are better than reported previously. In those who survive (and where data
are available) neurological outcome is good in only 1.6% of those sustaining
traumatic cardiorespiratory arrest (ERC Guideline 2010)
Truhlar A et. al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 4. Cardiac
arrest in special circumstances. Resuscitation 95 148-201 (2015)

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
ERC Guideline 2015
Truhlar A et. al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 4. Cardiac
arrest in special circumstances. Resuscitation 95 148-201 (2015)
1. Emphasis on rapid treatment of all potentially reversible pathology is the
basis of treatment guidelines.
• Hypoxaemia (oxygenation, ventilation).
• Compressible haemorrhage (pressure, pressure dressings,
tourniquets,novel haemostatic agents).
• Non-compressible haemorrhage (splints, intravenous fluid).
• Tension pneumothorax (chest decompression).
• Cardiac tamponade (immediate thoracotomy)
2. Chest compressions: although they may not be effective in hypovolaemic
cardiac arrest most survivors do not have hypovolaemia and in this
subgroup standard advanced life support may be lifesaving.
3. Standard CPR should not delay the treatment of reversible causes
(e.g., thoracotomy for cardiac tamponade).
4. Do not delay for unproven interventions such as spinal immobilisation.

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Leitlinie Schwerstverletztenversorgung
Deutsche Gesellschaft für Unfallchirurgie, Deutsche Gesellschaft für Allgemein- und Viszeralchirurgie, Deutsche Gesellschaft für Anästhesiologie und Intensivmedizin et al. S3 Leitlinie Polytrauma - AWMF-Register Nr. 012/019: AWMF; 2011
PrähospitalphaseKEINE Aussage
SchockraumBei definitiv vorliegendem Herzkreislauf-
stillstand, bei Unsicherheiten im Nachweis
eines Pulses oder bei anderen klinischen
Zeichen, die einen HKS wahrscheinlich
machen, soll unverzüglich mit der
Reanimation begonnen werden. (GoR A)

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Rosemurgy AS, Norris PA, Olson SM, Hurst JM, Albrink MH. Prehospital traumatic cardiac arrest: thecost of futility. J Trauma 1993; 35: 468-473; discussion 473-464
12.462 Trauma
? (?%) OHCA
138 (?%) Trauma-CPR
? (?%) ROSC
0 (0%) Überleben
Tabelle 6:Causes of death in 138 patients experiencing prehospital
cardiopulmonary arrest prior to or during transport to county trauma
centers:
Exsanguination 42
Closed head injury 31
Multiple organ system injuries 29
Cardiac injuries 12
Pneumohemothorax 7
Progression of preterminal state 4
Coagulopathy 3
High spinal injury 3
Traumatic asphyxia 3
Hypoxia/anoxia 2
Pulmonary edema 1
Late septic death 1
Summe: 138
ABER:
mind. 14 (10%) potentiell
überlebbare
Todesursachen!

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Fialka C, Sebok C, Kemetzhofer P et al. Open-chest cardiopulmonary resuscitation after cardiac arrest in casesof blunt chest or abdominal trauma: a consecutive series of 38 cases. J Trauma 2004; 57: 809-814
38 (100%) stumpfes
Rumpftrauma mit
max. 20min CCCPR
prähospital und
OCCPR im SR
4 (10,5%) überleben

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
ROSC after cardiac arrest
Gräsner JT, Meybohm P, Lefering R et al. ROSC after cardiac arrest--the RACA score topredict outcome after out-of-hospital cardiac arrest. Eur Heart J 2011; 32: 1649-1656
X=
0.3
+ (-0.2 männlicher Patient)
+ (-0.2 Patientenalter ≥80 Jahre)
+ (-0.6 Trauma) + (0.7 Hypoxie) + (0.5 Intoxikation)
+ (0.6 durch Laien) + (0.5 durch professionelles Personal beobachtet)
+ (-0.3 Pflegeheim) + (1.2 Arztpraxis) + (0.3 öffentlicher Raum) + (0.5 Krankenhaus)
+ (-0.8 PEA) + (-1.1 Asystole)
+ (0.2 Laienreanimation)
+ (-0.04 pro Minute bis Rettungsdienst ankommt)
Probability of ROSC =
1
(1 + e )-X
Konstante
Geschlecht?
Alter?
Ursache?
Beobachtet?
Ort?
EKG?
Laienreanimation
Dauer?
Aber: nicht für den Individuellen Patient
einsetzbar!

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
0%
10%
20%
30%
40%
50%
60%
70%
0 10 20 30 40 50 60
RO
SC W
ahrs
chei
nlic
hke
it g
em R
AC
A
Zeit [min]
ROSC after cardiac arrest

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
0%
10%
20%
30%
40%
50%
60%
70%
0 10 20 30 40 50 60
RO
SC W
ahrs
chei
nlic
hke
it g
em R
AC
A
Zeit [min]
ROSC after cardiac arrest

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
0%
10%
20%
30%
40%
50%
60%
70%
0 10 20 30 40 50 60
RO
SC W
ahrs
chei
nlic
hke
it g
em R
AC
A
Zeit [min]
ROSC after cardiac arrest

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
0%
10%
20%
30%
40%
50%
60%
70%
0 10 20 30 40 50 60
RO
SC W
ahrs
chei
nlic
hke
it g
em R
AC
A
Zeit [min]
ROSC after cardiac arrest
40 Jahre alt, kardialer Ursache,
im, EKG Kammerflimmern
80 Jahre alt, kardialer Ursache,
EKG Kammerflimmen
• 40 Jahre alt
• Trauma als Ursache
• EKG Kammerflimmern
40 Jahre alt, kardialer
Ursache EKG PEA
80 Jahre alt, kardialer
Ursache, EKG PEA

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Outcome
Gräsner JT, Wnent J, Seewald S et al. Cardiopulmonary resuscitation traumatic cardiac arrest--there aresurvivors. An analysis of two national emergency registries. Crit Care 2011; 15: R276
Zusammenführung der Ergebnisse aus
Deutschem Reanimationsregister
TraumaRegister DGU®

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Outcome
Gräsner JT, Wnent J, Seewald S et al. Cardiopulmonary resuscitation traumatic cardiac arrest--there are survivors. An analysis of two national emergency registries. Crit Care 2011; 15: R276
Traumatic Prehospital Cardiac Arrest 100%
ROSC 29%
Hospital admission after ROSC 26%
24h Survivial 13%
Discharged alive 7%
Discharged home 2%
De
uts
ch
es
Re
an
ima
tio
nsre
gsite
r
Tra
um
aR
eg
iste
r D
GU
®
n=368
n=107
n=95 n=814
n=369
n=221
n=56

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Reanimation nach Trauma
Therapie

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
ERC Guideline 2015
Truhlar A et. al. European Resuscitation Council Guidelines forResuscitation 2015: Section 4. Cardiac arrest in special circumstances.Resuscitation 95 148-201 (2015)
1. Treatment of reversible causes:
• Hypoxaemia (oxygenation, ventilation).
• Compressible haemorrhage (pressure, pressure dressings,
tourniquets,novel haemostatic agents).
• Non-compressible haemorrhage (splints, intravenous fluid).
• Tension pneumothorax (chest decompression).
• Cardiac tamponade (immediate thoracotomy)
2. Chest compressions: although they may not be effective in hypovolaemic
cardiac arrest most survivors do not have hypovolaemia and in this
subgroup standard advanced life support may be life-saving.
3. Standard CPR should not delay the treatment of reversible causes (e.g.,
thoracotomy for cardiac tamponade).
4. Do not delay for unproven interventions such as spinal immobilisation.

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Atemwegsmanagement
„Treatment of reversible Causes“
ERC Guideline 2015:
Hypoxaemia due to airway obstruction and
traumatic asphyxia has been reported as cause of
TCA in 13% of all cases.
Tracheal intubation in traumapatients is a difficult
procedure with a high failure rate if carried out by
less experienced care providers.
Use basic airway manoeuvres and second-
generation supraglottic airways to maintain
oxygenation if tracheal intubation cannot be
accomplished immediately.
NEU: KEIN Surgical Airway

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Blutung nach Aussen
„Treatment of reversible Causes“
ERC Guideline 2015:
Uncontrolled haemorrhage is the cause of TCA in
48% of all TCA.
The main principle is to achive ‘haemostasis without
delay’, usually with surgical or radiological intervention.
Treat compressible external haemorrhage with direct
pressure (with or without a dressing), use tourniquets if
needed and/orapply topical haemostatic agents
Non-compressible haemorrhage is more difficult. Use
splints(pelvic splint), blood products, intravenous fluids
and tranexamicacid while moving the patient to surgical
haemorrhage control.

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Kritische Blutung
Kulla M, Josse F, Helm M, Lampl L, Hossfeld B. Prähospitale Traumaversorgung - Versorgung kritischer
Blutungen, in DIVI Jahrbuch 2015/2016, S Kluge, A Markewitz, G Jorch, C Putensen, M Quintel, GW Sybrecht,
Editors. 2015, MWV - Medizinisch Wissenaschaftliche Verlagsgesellschaft: Berlin, Deutschland. 351-359.

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Beckenschlinge
Problem:
Kontinuierliche Blutung aus
venösen Gefäßen im
Plexus Sakralis

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Kritische Blutung nach Innen?
„Treatment of reversible Causes“
ERC Guideline2015:
„Non-compressible haemorrhage is more
difficult. Use splints (pelvic splint), blood
products, intravenous fluids and
tranexamicacid while moving the patient to
surgical haemorrhage control.“
Beckenschlinge (RTH Chr 22 SOP)
Reposition und Schienung?
CAVE: Versorgungszeit?

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Kritische Blutung

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Pleuraentlastung
„Treatment of reversible Causes“
ERC Guideline 2015:
13% of all cases of TCA are caused by tension
pneumothorax.
...perform bilateral thoracostomies in the 4th
intercostal space, extending to a clamshell
thoracotomy if required.
In the presence of positive pressure
ventilation, thoracostomies are likely to be
more effective than needle thoracocentesis
and quicker than inserting a chest tube

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Perikardentlastung
„Treatment of Reversible Causes“
ERC Guideline 2015:
..is the underlying cause of 10% of TCA.
Where there is TCA and penetrating trauma to the
chest or epigastrium, immediate resuscitative
thoracotomy via a clamshell incision can be life
saving.
ERC Guideline 2010 prähospital:
In patients with suspected trauma-related cardiac
tamponade, needle pericardiocentesis is probably
not a useful procedure.

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
ERC Guideline 2015
Truhlar A et. al. European Resuscitation Council Guidelines forResuscitation 2015: Section 4. Cardiac arrest in special circumstances.Resuscitation 95 148-201 (2015)
1. Treatment of reversible causes:
• Hypoxaemia (oxygenation, ventilation).
• Compressible haemorrhage (pressure, pressure dressings,
tourniquets,novel haemostatic agents).
• Non-compressible haemorrhage (splints, intravenous fluid).
• Tension pneumothorax (chest decompression).
• Cardiac tamponade (immediate thoracotomy)
2. Chest compressions: although they may not be effective in hypovolaemic
cardiac arrest most survivors do not have hypovolaemia and in this
subgroup standard advanced life support may be life-saving.
3. Standard CPR should not delay the treatment of reversible causes (e.g.,
thoracotomy for cardiac tamponade).
4. Do not delay for unproven interventions such as spinal immobilisation.
✓

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Herzdruckmassage
ERC Guideline 2015:
Chest compressions are still the standard of care in
patients with cardiac arrest, irrespective of aetiology.
In cardiac arrest caused by hypovolaemia, cardiac tamponade
or tension pneumothorax, chest compressions are unlikely to
be as effective as in normovolaemic cardiac arrest.
Because of this fact, chest compressions take a lower
priority than the immediate treatment of reversible causes,
e.g. thoracotomy, controlling haemorrhage, etc.
In an out-of-hospital setting, only essential lifesaving
interventions should be performed onscene followed by rapid
transfer to the nearest appropriate hospital

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Herzdruckmassage
ERC Guideline 2015
„In cardiac arrest caused by hypovolaemia, cardiac tamponade or tension
pneumothorax, chest compressions are unlikelyto be as effective as in
normovolaemic cardiac arrest.“

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Herzdruckmassage
Mechanische Reanimationshilfen

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Zugang zum venösen System
Sheldon Katheter periphervenöser Zugang intraossär

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Volumengabe
ERC Guideline 2015 (prähospital)
Uncontrolled haemorrhage is the cause of trau-matic
cardiac arrest in 48% of all TCA
Limited evidence and general consensus have supported a
conservative approach to intravenous fluid infusion, with
permissive hypotension until surgical haemostasis is
achieved.
Spahn DR, Bouillon B, Cerny V et al. Management of
bleeding and coagulopathy following major trauma: an
updated European guideline. Crit Care 2013; 17: R76
AWMF S3 Leitlinie Intravasale Volumentherapie beim
Erwachsenen AWMF Register-Nr.: 001/020
Intravasale Blutverluste sind
durch VOLUMEN ZU ERSETZEN

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Katecholamine
ERC Guidelines 2015
• The possible role of vasopressors (e.g., vasopressin) in trauma resuscitation
is unclear and is based mainly on case reports
Suprarenin Vasopressoren
???
Siehe auch:
Chiang WC et al. Prehospital intravenous epinephrine may boost survival of patients with traumatic cardiac arrest:
a retrospective cohort study. Scand J Trauma Resusc Emerg Med 23 (1): 102 (2015)
Jacobs IG et al. Effect of adrenaline on survival in out-of-hospital cardiac arrest: A randomised double-blind
placebo-controlled trial. Resuscitation 82 (9): 1138-1143 (2011)

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Vasopressoren
Fallberichte zu Vasopressoren
• Krismer AC, Wenzel V, Voelckel WG et al. Employing vasopressin as an adjunct vasopressor in uncontrolled traumatic hemorrhagic shock. Threecases and a brief analysis of the literature. Anaesthesist 2005; 54: 220-224
Vasopressoren
???

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Vasopressoren
Fallberichte zu Vasopressoren
• Krismer AC, Wenzel V, Voelckel WG et al. Employing vasopressin as an adjunct vasopressor in uncontrolled traumatic hemorrhagic shock. Threecases and a brief analysis of the literature. Anaesthesist 2005; 54: 220-224
Vasopressoren
???

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Defibrillation
ERC Guidelines 2015:
Grundsatz:
– Ja, bei Kammerflimmern immer
CAVE:
– Soll die Therapie reversibler Ursachen
nicht behindern...

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
ERC Guideline 2015
Truhlar A et. al. European Resuscitation Council Guidelines forResuscitation 2015: Section 4. Cardiac arrest in special circumstances.Resuscitation 95 148-201 (2015)
1. Treatment of reversible causes:
• Hypoxaemia (oxygenation, ventilation).
• Compressible haemorrhage (pressure, pressure dressings,
tourniquets,novel haemostatic agents).
• Non-compressible haemorrhage (splints, intravenous fluid).
• Tension pneumothorax (chest decompression).
• Cardiac tamponade (immediate thoracotomy)
2. Chest compressions: although they may not be effective in hypovolaemic
cardiac arrest most survivors do not have hypovolaemia and in this
subgroup standard advanced life support may be life-saving.
3. Standard CPR should not delay the treatment of reversible causes (e.g.,
thoracotomy for cardiac tamponade).
4. Do not delay for unproven interventions such as spinal immobilisation.

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Prähospitale Trauma-CPR
Indikation zur Trauma-CPR?
Therapie reversibler Ursachen
Reevaluation
Beckenschlinge / Schienung
erwägen
HypoxieSpannungs-
pneumothoraxKatastrophale
Blutung
Perikardtam-
ponade
Tourniquet bei V.a.
Extremitätentrauma
Transport in nächstes Traumazentrum unter CPR gem. ERC Leitlinie
HDM
Defibrillation?
HDM
Supra-
renin
Anmel-
dung
Sonstige
Maßnahmen

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Publikation Gässler et al. Mai 2015
Gässler H, Helm M, Lampl L, Kulla M. Cardiopulmonary Resuscitation after Traumatic Event. Notarzt 31 (4): 210-
216 (2015)

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Trauma-CPR (ERC Guideline 2015)

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Reanimation nach Trauma
Sonstige Therapieoptionen

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Einsatztaktik HEMS – London 1/2
Sherren PB, et al.: Algorithm for the resuscitation of traumatic cardiac arrest patients in a physician-staff ed helicopter emergency medical service. Critical Care 2013, 17:308.

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Einsatztaktik HEMS – London 2/2
Sherren PB, et al.: Algorithm for the resuscitation of traumatic cardiac arrest patients in a physician-staff ed helicopter emergency medical service. Critical Care 2013, 17:308.

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
ERC Guidelines 2015
Notfallthorakotomie (RT)
The prerequisites for a successful RT can be summarised as the ‘four Es rule’ (4E):
Expertise: teams that perform RT must be led by a highly trained and competent
healthcare practitioner.
Equipment: adequate equipment to carry out RT and to deal with the
intrathoracic findings is mandatory
Environment: ideally RT should be carried out in an operating theatre. RT
should not be carried out if there is inadequate physical access to the patient, or
if the receiving hospital is not easy to reach.
Elapsed time: the time from loss of vital signs to commencing aRT should not be
longer than 10 min.
If any of the four criteria is not met, RT is futile and exposes the team to
unnecessary risks.

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Tranexamsäure
Ker K, Kiriya J, Perel P et al. Avoidable mortality from giving tranexamic acid tobleeding trauma patients: an estimation based on WHO mortality data, a systematicliterature review and data from the CRASH-2 trial. BMC Emerg Med 2012; 12: 3
Bei Schwersteverletzten mit Verdacht auf
Hyperfibrinolyse
1g als Bolus i.v. prähospital
1g über 8 Stunden innerklinisch

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Temperaturmanagement
34.0°C

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Aktuell: Normothermie bei Trauma + CPR
36.5°C

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Reanimation nach Trauma
Einsatztaktik

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Einsatztaktik - Notarzt
Klein KR. Traumatic cardiac arrests - the action or the provider, what makes thedifference? Crit Care 2013; 17: 156
... In multiple European studies it was noted that
there was a decrease in mortality of trauma
patients without a decrease in scene time when a
physician was part of the flight crew . In the US,
less than 5% of HEMS are staffed by physicians, and
most of those involved in such teams are in their first
few years out of medical school . Thus, no US EMS
systems have fully trained physicians as part of their
standard ambulance crew...

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Einfluss des Rettungsmittels
Di Bartolomeo S, Sanson G, Nardi G, Michelutto V, Scian F. HEMS vs. Ground-BLS care in traumatic
cardiac arrest. Prehosp Emerg Care 2005; 9: 79-84

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Einsatztaktik bei Trauma-CPR
ERG Guideline 2015
Prehospital care. Short prehospital times are
associated with increased survival rates for major
trauma and TCA. The time elapsed between injury
and surgical control of bleeding should therefore be
minimised and the patient should be immediately
transferred to a trauma centre for ongoing damage
control resuscitation.
A ‘scoop and run’ concept for these patients may be
life saving.

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Personelle Resourcen
Lehren aus dem eigenen Bereich
• Teamleader (erfahrenster Oberarzt)
• Operativ
– 2 Chirurgen
– 2 OP Pfleger
• Anästhesie
– 2 Anästhesisten
– 1 Fachschwester Anästhesie
• Bildgebung
– Facharzt Radiologie
– MTRA
• ZINA
– 2 Pflegekräfte
– 1-2 Springer
– Dokumentation
• Weiter Fachdisziplinen (Facharzt mit Entscheidungskompetenz!)
ca. 17 Beteiligte

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Innerklinische Bildgebung
eFAST Trauma-
spirale
???

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
REBOA
Stannard A, Eliason JL, Rasmussen TE. Resuscitative endovascular balloon occlusion ofthe aorta (REBOA) as an adjunct for hemorrhagic shock. J Trauma 2011; 71: 1869-1872

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Herzkreislaufunterstützung
Tseng YH, Wu TI, Liu YC, Lin PJ, Wu MY. Venoarterial extracorporeal life support in post-traumatic shockand cardiac arrest: lessons learned. Scand J Trauma Resusc Emerg Med 2014; 22: 12

Endergebnis
• Gräsner JT, Wnent J, Seewald S et al. Cardiopulmonary resuscitation traumatic cardiac arrest--there aresurvivors. An analysis of two national emergency registries. Crit Care 2011; 15: R276
• Smith K, Andrew E, Lijovic M, Nehme Z, Bernard S. Quality of Life and Functional Outcomes 12 Months After Out-of-Hospital Cardiac Arrest. Circulation 2015; 131: 174-181
Reanimation in Australien (med. Ursache)• 40% Transport ins Krankenhaus• 35% ROSC auf Transport oder im Krankenhaus• 13% Klinkentlassung• 6-8% mit gutem Ergebnis
Trauma im SR
ISS 24±12
100% Klinikaufnahme86% Klinikentlassung50% gutes Ergebnis
Reanimation nach Trauma30-45% ROSC10-15% Klinikaufnahme5-10% Klinikentlassung2-5% gutes neurologisches Ergebnis

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Reanimation nach Trauma
Abbruchkriterien

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Trauma-CPR – Pro und Contra
Reanimation nach Trauma indiziert
Potentiell überlebbare Verletzung
Beobachteter HKST
Laufende Laienreanimation
Kammerflimmern
Reversible Ursachen noch nicht ausgeschlossen
KEINE Indikation
Mehrere Verletzte
Sichere Todeszeichen
Nicht überlebbares Trauma

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Trauma-CPR – Pro und Contra
Reanimation indiziert
Potentiell überlebbare
Verletzung
Beobachteter HKST
Laufende Laienreanimation
Kammerflimmern / PEA
Reversible Ursachen noch
nicht ausgeschlossen
Fraglich
Einfluss des
Verletzungsmechanismus
Patientenalter
Fahrzeit bis Klinik >15min
Asystolie
KEINE Indikation
Mehrere Verletzte
Sichere Todeszeichen
Nicht überlebbares Trauma
???

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Reanimation nach Trauma
Zusammenfassung

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Prähospitale Reanimation nach Trauma
CPR ≠ Trauma-CPR
Indikation!
Das Team ist entscheidend!

Bundeswehrkrankenhaus UlmAkademisches Krankenhaus der Universität Ulm
Klinik für Anästhesie und Intensivmedizin
Sektion Notfallmedizin
Dr. Martin Kulla, DESA
Dr. Martin Kulla, DESAKlinik für Anästhesie und IntensivmedizinBundeswehrkrankenhaus UlmOberer Eselsberg 4089081 Ulm
Vielen Dank