Therapie der diastolischen Herzinsuffizienz
51
Therapie der diastolischen Herzinsuffizienz Prof. Burkert Pieske Department of Cardiology Med.University of Graz Kardiologie Update München, 15.-16.12.2012
Transcript of Therapie der diastolischen Herzinsuffizienz

Therapie der
diastolischen Herzinsuffizienz
Prof. Burkert Pieske
Department of Cardiology
Med.University of Graz
Kardiologie UpdateMünchen, 15.-16.12.2012
physical
acvity ↓
CVD risk
factors &
biomarkers
environmental
determinants
genetic
determinants
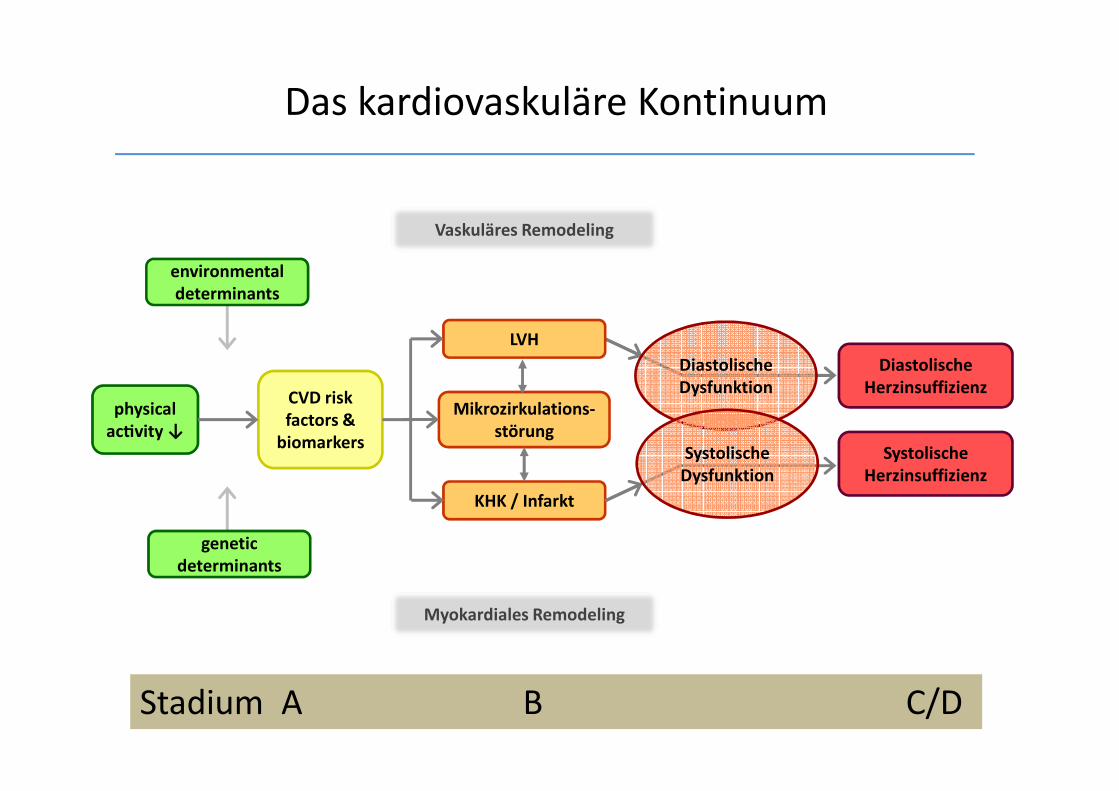
Diastolische
Herzinsuffizienz
Systolische
Herzinsuffizienz
Vaskuläres Remodeling
LVH
KHK / Infarkt
Mikrozirkulations-
störung
Myokardiales Remodeling
Diastolische
Dysfunktion
Systolische
Dysfunktion
Das kardiovaskuläre Kontinuum
Stadium A B C/D

Diastolische Herzinsuffizienz
• Pathophysiologie
• Diagnose & Epidemiologie
• Therapie

The Relationship Between Pressure and Volume
HFPEF, HFNEF, oder Diastolische Herzinsuffizienz?

Pathophysiologie HFPEF
Kardiale Dysfunktion & Remodeling
Diastolische DysfunktionSystolische Dysfunktion
VorhofdysfunktionEnergiestoffwechsel
Mikrozirkulation
Autonome DysfunktionChronotrope Inkompetenz
Frequenzstarre
Vaskuläre VeränderungenEndotheldysfunktionCompliancestörung
Ventrikulo-arterielle Kopplung
NierenfunktionsstörungVerminderte GFR
(Latente) ÜberwässerungGestörte Na-Homöostase
(renale) Anämie
Pulmonale FunktionPostkapilläre/präkapilläre
HypertoniePulmonale
Begleiterkrankungen (COPD)
Alter/LebensstilAdipositas
Dekonditionierung

Diastolische Herzinsuffizienz
• Pathophysiologie
• Diagnose & Epidemiologie
• Therapie
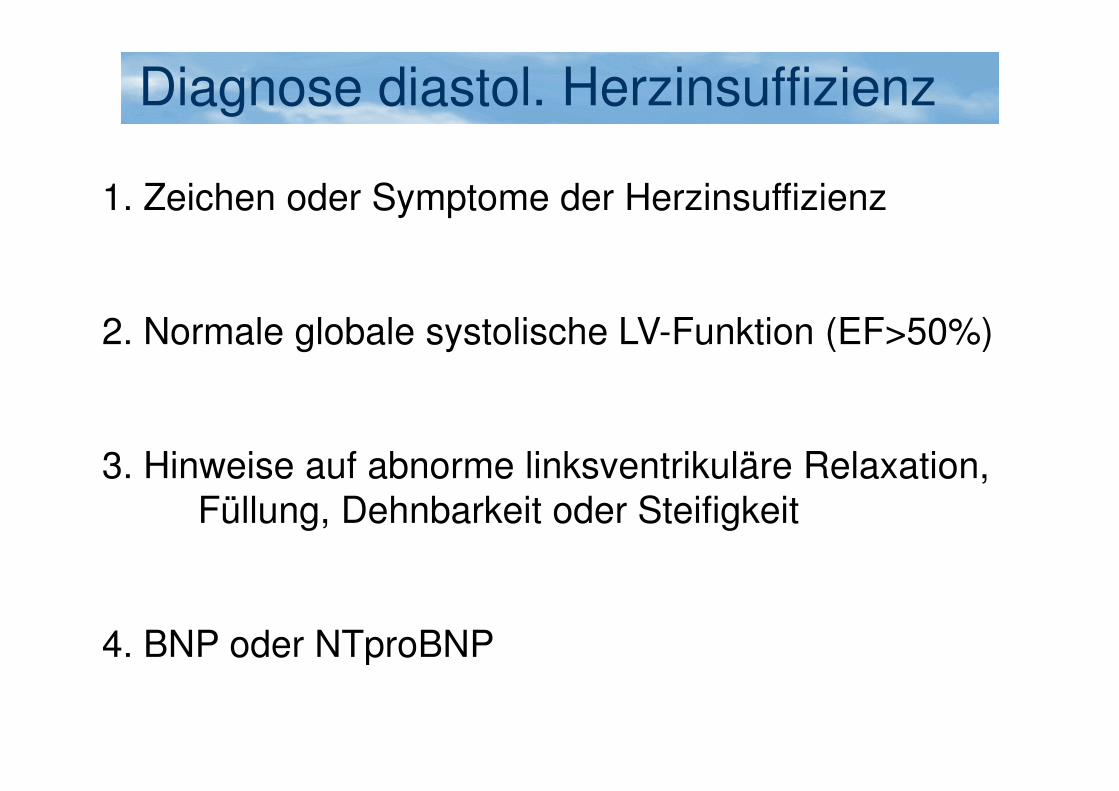
Diagnose diastol. Herzinsuffizienz
1. Zeichen oder Symptome der Herzinsuffizienz
2. Normale globale systolische LV-Funktion (EF>50%)
3. Hinweise auf abnorme linksventrikuläre Relaxation, Füllung, Dehnbarkeit oder Steifigkeit
4. BNP oder NTproBNP

Diagnose diastolische Herzinsuffizienz
HFA/ESC 2007
Paulus W et al.

Baseline plasma NT-proBNP and clinical characteristics: results from the irbesartan
in heart failure with preserved ejection fraction trial.
McKelvie RS, Komajda M, McMurray J, Zile M, Ptaszynska A, Donovan M, Carson P,
Massie BM; I-Preserve Investigators.
Majority in NYHA III
Median NTproBNP: 341 (135-974) pg/ml
No Atrial fibrillation: around 250 pg/ml (ca. 75%)
With atrial fibrillation: >900 pg/ml (ca. 25%)
NTproBNP in I-Preserve

Diagnose diastolische Herzinsuffizienz
Paradigmenwechsel 2011:
• Neue Echo-Techniken & Parameter
• Belastungstests („Diastolic Stress Test“)!
• Neue Biomarker: Subgruppen, Response to Therapy
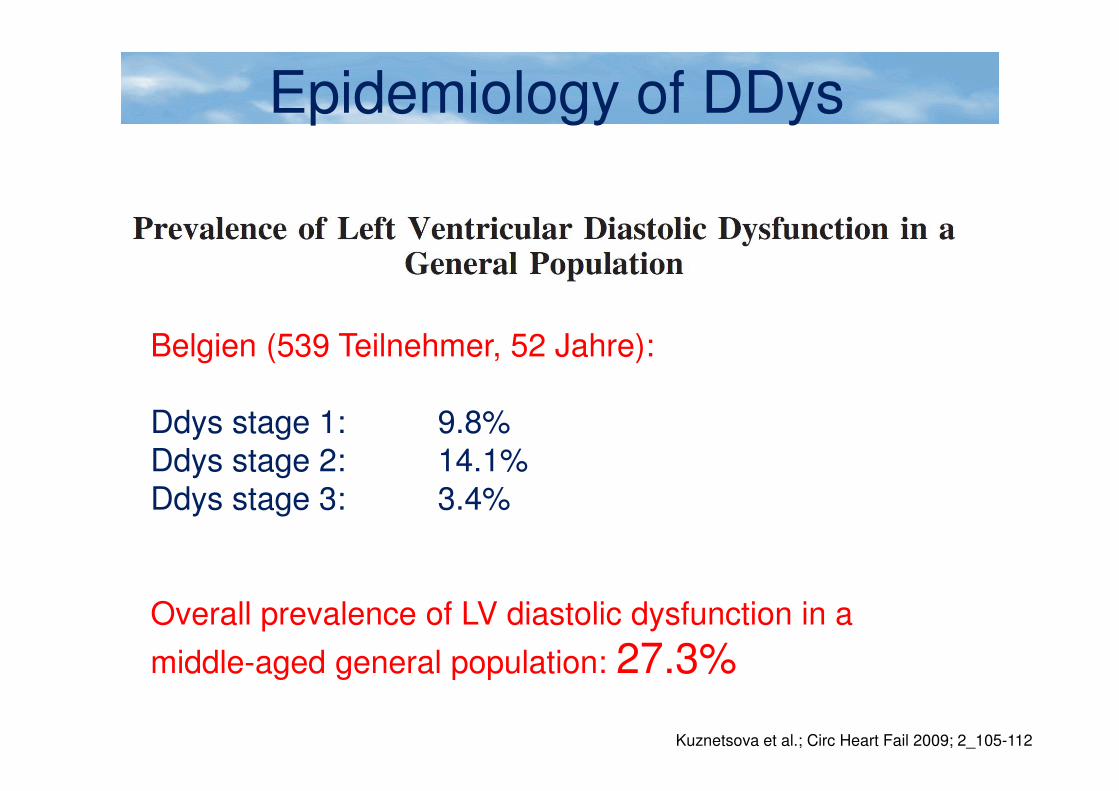
Epidemiology of DDys
Kuznetsova et al.; Circ Heart Fail 2009; 2_105-112
Belgien (539 Teilnehmer, 52 Jahre):
Ddys stage 1: 9.8%Ddys stage 2: 14.1%Ddys stage 3: 3.4%
Overall prevalence of LV diastolic dysfunction in a
middle-aged general population: 27.3%

Zunahme der diastol. Herzinsuffizienz
Owan et al., N Engl J 2006; 355
6076 CHF patients, EF >50% vs. EF <50%
Relative proportion of EF>50%
DHF – Can we predict therapy?
• Problems:
• DHF is no single disease entity
• Pathophysiology is multifacetted
• Prevalence of diastolic dysfunction high
• 2012: >50% of HF cases are HFPEF

Diastolische Herzinsuffizienz
• Pathophysiologie
• Diagnose & Epidemiologie
• Therapie

Systolische Herzinsuff.: Therapie 2012
NYHA I NYHA II NYHA III NYHA IV
Beta-Blocker
Diuretika
ACE – Hemmer
Digitalis
Spironolacton
AT-1-Antagonisten

Diastolische Herzinsuff.: Therapie 2012
NYHA I NYHA II NYHA III NYHA IV
?
Diuretika ?
?
?
?
?
Therapie der diastolischen HI
1. Prävention ?
2. Allgemeinmassnahmen
3. Spezifische Behandlungsansätze
4. Neue therapeutische Optionen

Age-dependent decline in diast. Fct.
Redfield et al., Circulation 2005;112:2254
Population-based, >45Jahre
Filling pressure (E/É)LV-Relaxation
Diastolic LV stiffness


Physical activity & Heart FailureFramingham Heart Study, 1142 Teilnehmer
Elisabeth Kraigher-Krainer et al., Circulation 2010; 122: A15104 (Abstract)

Therapie DHF
1. Prävention ?
2. Allgemeinmassnahmen
3. Spezifische Behandlungsansätze
4. Neue therapeutische Optionen

1. Sind alle Risikofaktoren optimal kontrolliert?
BP < 130/80 mmHg? (v.a. durch RAS-Blocker)
HbA1c < 7.0 mg% ?
Statin-Therapie, wenn indiziert
2. Liegt ein inadäquater RR-Anstieg unter Belastung vor?
Belastungstest - Therapieren!
3. Wie ist die Herzfrequenz unter Belastung?
Tachykard – Antitachykarde Therapie
Chronotrope Inkompetenz? – Bradykardisierende Substanzen ab
4. Vorhofflimmern? – SR wieder herstellen?
5. Zeichen der Überwässerung?
Diuretika beginnen/steigern, Salz-Restriktion
6. Gewichtsreduktion, regelmässige körperliche Aktivität
Therapie der diastolischen HI
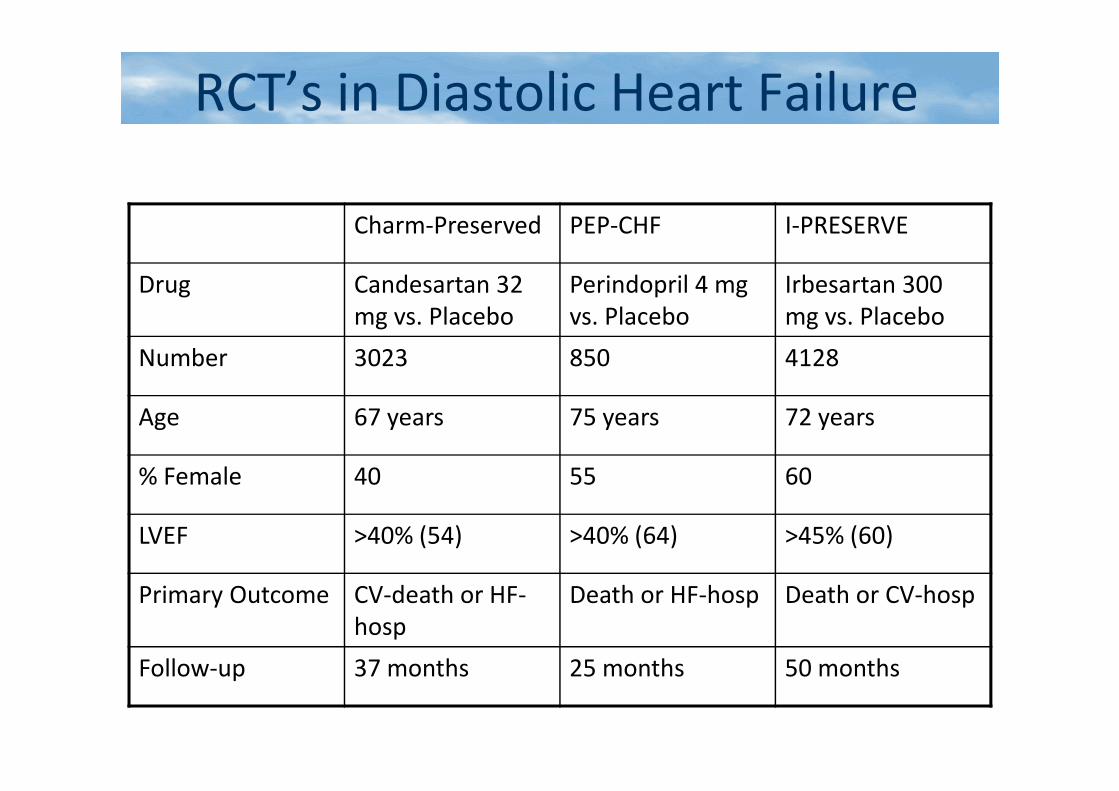
RCT’s in Diastolic Heart Failure
Charm-Preserved PEP-CHF I-PRESERVE
Drug Candesartan 32
mg vs. Placebo
Perindopril 4 mg
vs. Placebo
Irbesartan 300
mg vs. Placebo
Number 3023 850 4128
Age 67 years 75 years 72 years
% Female 40 55 60
LVEF >40% (54) >40% (64) >45% (60)
Primary Outcome CV-death or HF-
hosp
Death or HF-hosp Death or CV-hosp
Follow-up 37 months 25 months 50 months

I-Preserve: Irbesartan in HFNEF
Massie BM et al., N Engl J Med 2008; 359
Primary endpoint: All-cause mortality or cardiovascular hospitalisation
At 49 months:
742 (Irbesartan) vs. 763 (Placebo)

I-Preserve: Echo-Substudie
Zile et al.; Circulation 2011; 124
1/3 ohne LA-Remodeling! 1/3 normale diastol. Funktion!
Therapy of diastolic Heart Failure
1. Prevention ?
2. General recommendations
3. Specific therapeutical modalities
4. Neue Therapieoptionen

202 Studien zu DHF/HFPEFwww.clinicaltrials.gov

Diastolic dysfunction
Sosalla and Maier; Pharmacololgy&Therapeutics 2011; doi: 10.1016/j.pharmathera.2011.11.003
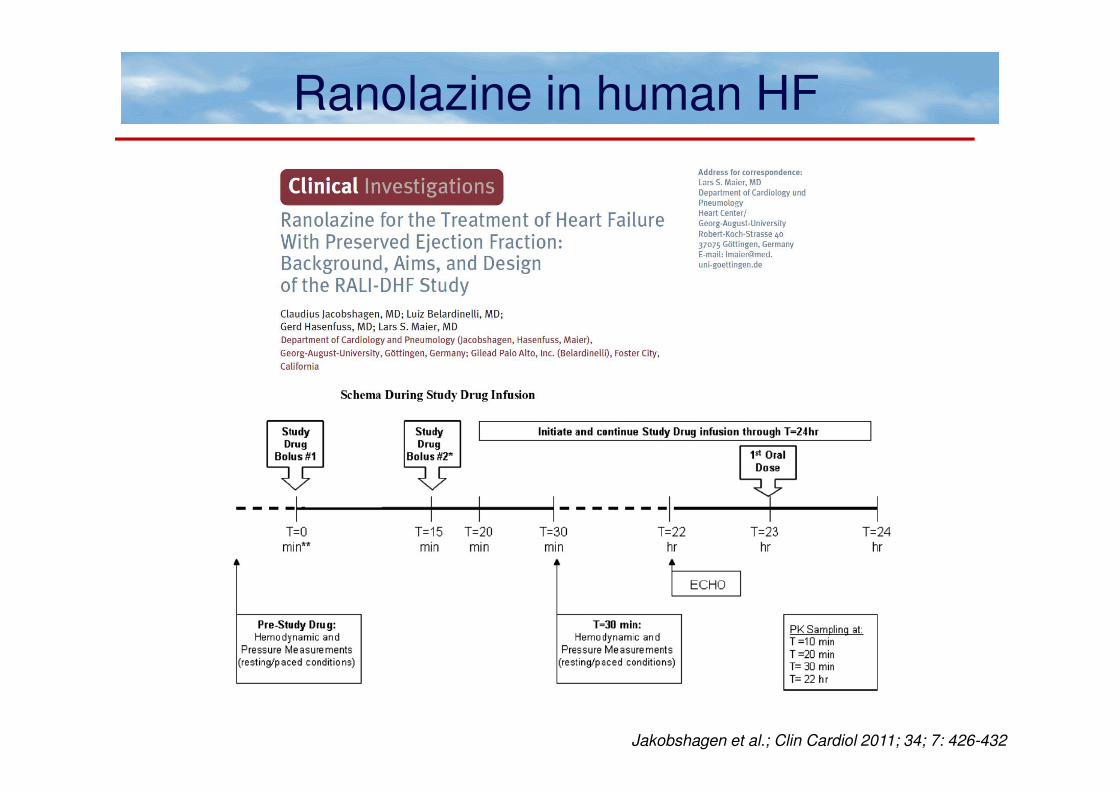
Ranolazine in human HF
Jakobshagen et al.; Clin Cardiol 2011; 34; 7: 426-432
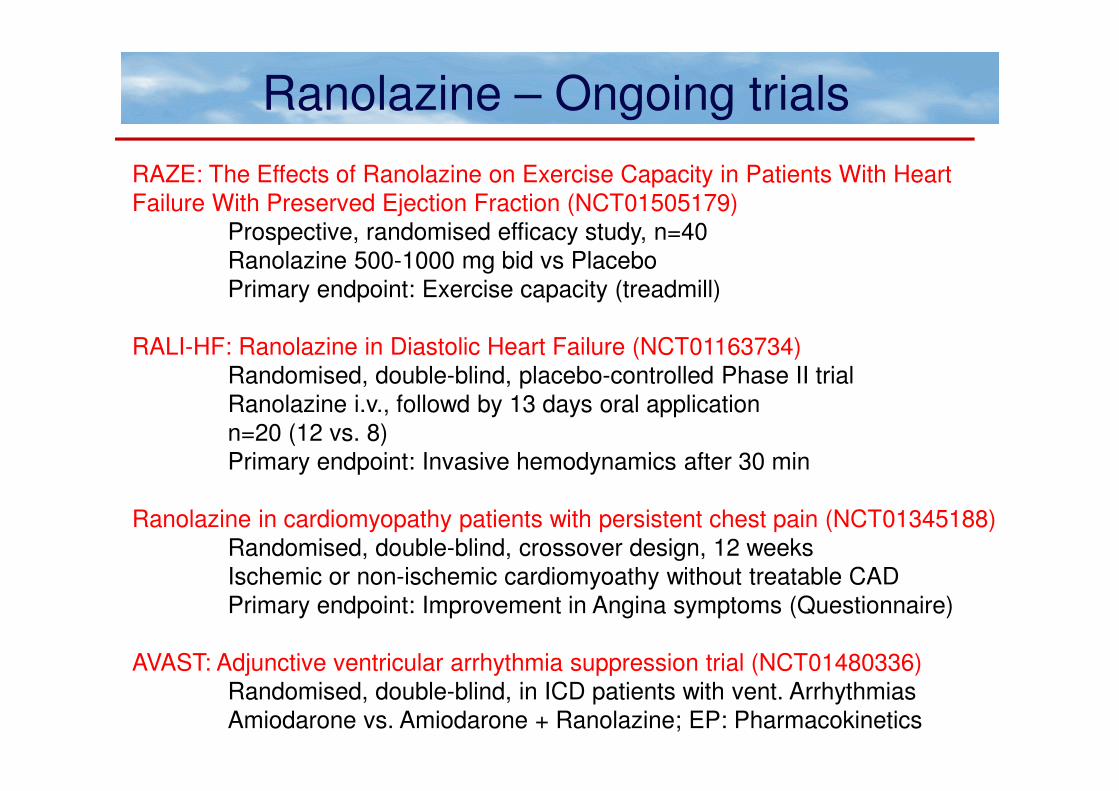
Ranolazine – Ongoing trials
RAZE: The Effects of Ranolazine on Exercise Capacity in Patients With Heart Failure With Preserved Ejection Fraction (NCT01505179)
Prospective, randomised efficacy study, n=40Ranolazine 500-1000 mg bid vs PlaceboPrimary endpoint: Exercise capacity (treadmill)
RALI-HF: Ranolazine in Diastolic Heart Failure (NCT01163734)Randomised, double-blind, placebo-controlled Phase II trialRanolazine i.v., followd by 13 days oral applicationn=20 (12 vs. 8)Primary endpoint: Invasive hemodynamics after 30 min
Ranolazine in cardiomyopathy patients with persistent chest pain (NCT01345188)Randomised, double-blind, crossover design, 12 weeksIschemic or non-ischemic cardiomyoathy without treatable CADPrimary endpoint: Improvement in Angina symptoms (Questionnaire)
AVAST: Adjunctive ventricular arrhythmia suppression trial (NCT01480336)Randomised, double-blind, in ICD patients with vent. ArrhythmiasAmiodarone vs. Amiodarone + Ranolazine; EP: Pharmacokinetics

PDE-5 Hemmung (Sildenafil)
44 Patienten, EF>50% + PA systol. Druck >40 mmHgSildenafil 3x50mg vs. Placebo, FU 12 Monate
Rechtsherzkatheter

Sildenafil
Guazzi et al.; Circulation 2011; 124: 164-174

RELAX• Study Design: Randomized (1:1), double-blind, placebo
controlled treatment study• Intervention: PDE-5 inhibition with sildenafil (20 mg tid for 12
weeks followed by 60 mg tid for 12 weeks) or placebo for 24 weeks
• Study population: 190 patients with a clinical diagnosis of HF and normal EF ( 50%) enrolled over a planned 3.25 year enrollment period.
• Primary outcome: The primary endpoint will be exercise capacity as assessed by the change in peak peak VO2 at 24 weeks of double blinded therapy compared to the baseline peak VO2 .
• Secondary outcomes:• 1. Change in a composite score reflective of clinical status after
24 weeks of double-blinded treatment with PDE-5 inhibitor or placebo.
• 2. Change in submaximal exercise capacity at 12 and 24 weeks as assessed by 6 minute walk test
• 3. Change in peak VO2 at 12 weeks
Scott D. Solomon, MD, Michael Zile, MD, Burkert Pieske, MD,
Adriaan Voors, MD, Amil Shah, MD, Elisabeth Kraigher-Krainer, MD,
Victor Shi, MD, Toni Bransford, MD, Madoka Takeuchi, MS,
Jianjian Gong, PhD, Martin Lefkowitz, MD, Milton Packer, MD,
John J.V. McMurray, MD for the PARAMOUNT Investigators
The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with
Preserved Ejection FractionThe Prospective comparison of ARNI with ARB on
Management Of heart failUre with preserved ejectioN fraction (PARAMOUNT) Trial
Objectives and Hypothesis
• The PARAMOUNT trial was designed to test the safety and efficacy of LCZ696 in patients with HFpEF.
• We hypothesized that LCZ696 would reduce NT-proBNP to a greater extent than the ARB valsartan at 12 weeks, and would be associated with favorable changes in cardiac structure and function at 36 weeks

Weeks Post Randomization
LCZ696
Valsartan
0 5 10200
300
400
500
600
700
800
900
1000N
Tpr
oBN
P(p
g/m
l)
LCZ696/Valsartan:0.77 (0.64, 0.92)P = 0.005
p = 0.063
12
Primary Endpoint: NT-proBNP at 12 Weeks
783 (670,914)
862 (733,1012) 835 (710, 981)
605 (512, 714)

Lancet. 2012 Aug 24 [Epub]

Aldosterone Receptor Blockade
in Diastolic Heart Failure
The Aldo-DHF Trial
Frank Edelmann, M.D., Rolf Wachter, M.D., Albrecht Schmidt, M.D., Elisabeth Kraigher-
Krainer,M.D., Caterina Colantonio, M.D., Wolfram Kamke, M.D., André Duvinage, M.D.,
Raoul Stahrenberg, M.D., Kathleen Dustewitz, M.D., Markus Löffler, M.D., Hans-Dirk
Düngen, M.D., Carsten Tschöpe, M.D., Christoph Herrmann-Lingen, M.D., Martin Halle,
M.D., Gerd Hasenfuss, M.D., Götz Gelbrich,Ph.D., and Burkert Pieske, M.D.
For the Aldo-DHF Investigators
Registered at www.controlled-trials.com: ISCRTN94726526; Eudra-CT no. 2006-002605-31
ESC Munich, Aug 26, 2012
Hot Line I

Objective and Hypothesis
Aldo-DHF was designed to test the efficacy and
safety of the aldosterone receptor antagonist
spironolactone in patients with diastolic heart
failure.
We hypothesized that spironolactone would improve
diastolic function and exercise capacity as compared
to placebo after 12 months of treatment .
Aldo-DHF Study protocol published:
Edelmann et al., Eur J Heart Fail 2010;12:874-882
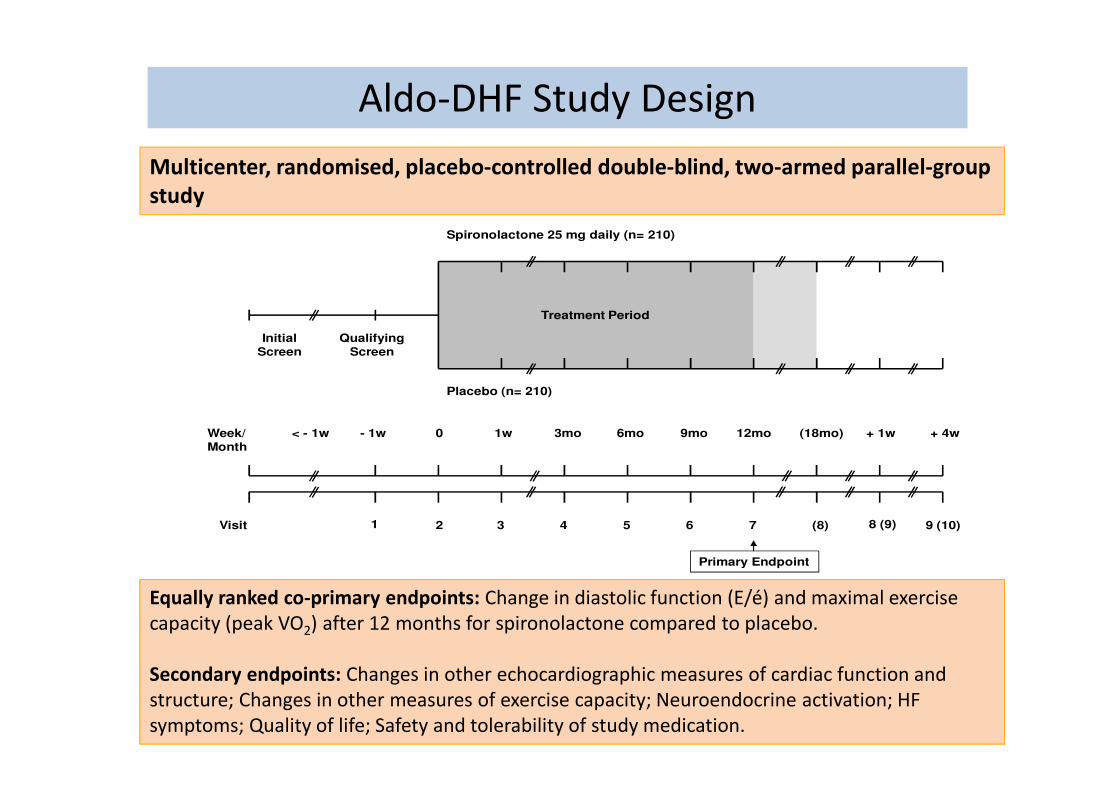
Placebo (n= 210)
Spironolactone 25 mg daily (n= 210)
Week/Month
QualifyingScreen
InitialScreen
Visit
< - 1w - 1w + 1w0 1w 3mo 6mo + 4w9mo 12mo (18mo)
2 31 4 5 76 8 (9)(8) 9 (10)
Treatment Period
Primary Endpoint
Equally ranked co-primary endpoints: Change in diastolic function (E/é) and maximal exercise
capacity (peak VO2) after 12 months for spironolactone compared to placebo.
Secondary endpoints: Changes in other echocardiographic measures of cardiac function and
structure; Changes in other measures of exercise capacity; Neuroendocrine activation; HF
symptoms; Quality of life; Safety and tolerability of study medication.
Multicenter, randomised, placebo-controlled double-blind, two-armed parallel-group
study
Aldo-DHF Study Design

Placebo (n=209) Spironolactone (n=213)
Age (years) 67±8 67±8
Female sex (%) 53 52
Heart failure hospitalisation
(past 12 months; %)36 38
Coronary heart disease (%) 37 43
Hypertension (%) 91 92
Diabetes mellitus (%) 16 17
NYHA class (%)
Class II 88 85
Class III 12 15
BMI - kg/m2 28·9±3·6 28·9±3·6
BP systolic - mmHg 135±18 135±18
BP diastolic - mmHg 80±12 79±10
eGFR - mL/min/1·73m2 78±18 79±19
NT-proBNP (ng/L; median) 148 (80-276) 179 (81-276)
Baseline characteristics

Ch
an
ge
in
E/e
‘
1
0
-1
Baseline 6 months 12 months
p < 0.001 p < 0.001
Placebo
Spironolactone
Time since randomisation
Spironolactone: 12.7±3.6 to 12.1±3.7
Placebo: 12.8±4.4 to 13.6±4.3
(P<0.001 for difference between groups)
Primary endpoint - E/é

TOPCAT: Trial Design
• AGE ≥≥≥≥ 50 YRS• EF ≥≥≥≥ 45% WITHIN 6 MONTHS • HEART FAILURE SYMPTOMS AND SIGNS• CONTROLLED SYSTOLIC BP (< 140 mm Hg)*
• SERUM K+ ≤≤≤≤ 5.0 MMOL/L
PLUS ONE OF THE FOLLOWING:• HF HOSPITALIZATION WITHIN 12 MONTHS • BNP ≥≥≥≥ 100 PG/ML• N-TERMINAL PRO-BNP ≥≥≥≥ 360 PG/ML
RANDOMIZE
SPIRONOLACTONE 15 MG
PLACEBO 15 MG
DOSE TITRATION (TARGET 30 MG)* Optional Titration to 45 mg at 4 mos
COMPOSITE PRIMARY ENDPOINTCV death, Aborted cardiac arrest, Hospitalization for
management of HF
Week 4
Week 0
~ 3.25 yrs
N=3500

Edelmann F1, Gelbrich G2, Düngen H-D3, Fröhling S1, Wachter R1, Binder L1, Töpper A3, Jahandar Lashki D3, Schwarz S4, Löffler M2, Herrmann-
Lingen C1, Hasenfuß G1, Halle M4, Pieske B5
1 University of Göttingen, Germany; 2 Coordination Centre of Clinical Trails Leipzig,Germany; 3 Charité University Medicine Berlin, Germany; 4 Technical UniversityMunich, Germany; 5 Medical University, Graz, Austria
Exercise training in heart failure with preserved ejection fraction (Ex-DHF)
ISRCTN 42524037

Baseline Visit
n= 71
Randomisation
n= 67
n= 46 n= 21
3 months follow up
n= 20
3 months follow up
n= 44
Training Controls
Return of consent, n= 2
Fulfilled any of the exclusion criteria, n= 2; clinically eligible, rejected participation; n= 2
Violation of protocol, n=1
Patients Follow up
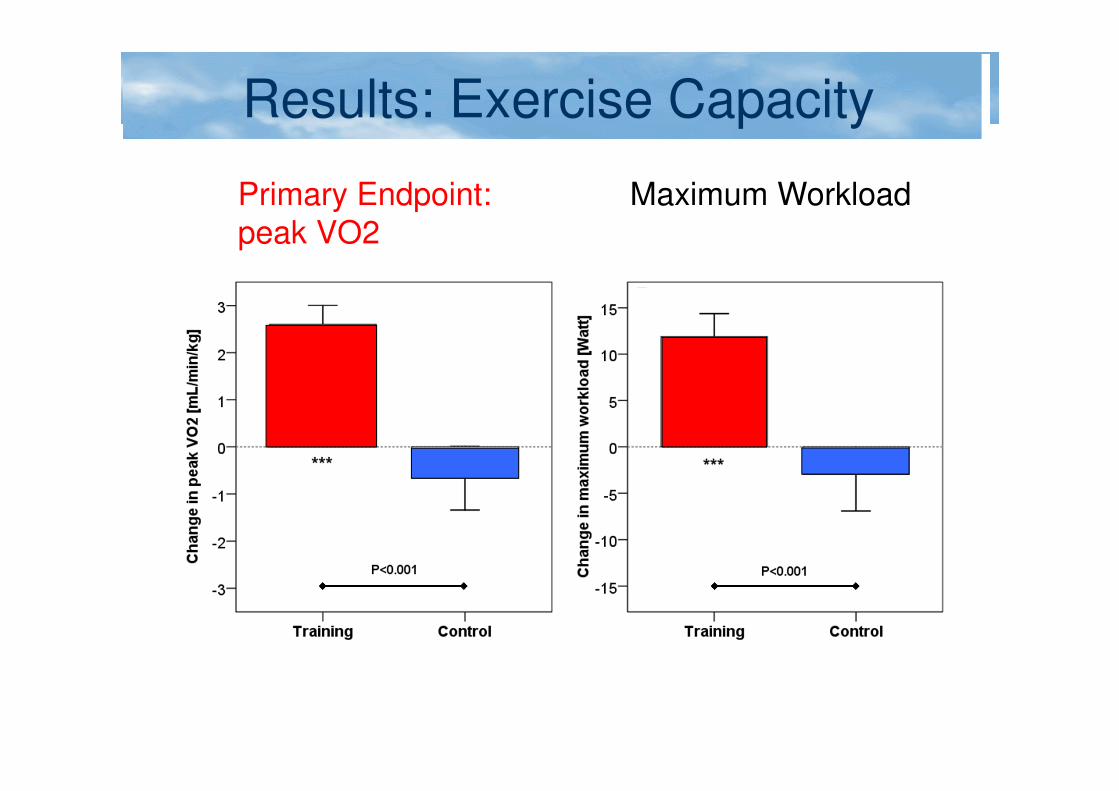
Results: Exercise Capacity
Primary Endpoint: peak VO2
Maximum Workload

Diastolic Function & LA remodeling
Change in E/é Ratio Change in LA Volume Index

New: Ex-DHF: Exercise traininig in DHF
n= 320, combined clinical endpoint (mod. Cleland-Score)
Multicenter, prospective, controlled trial to assess the effects of exercise in DHF
Pieske B, Edelmann F, Gelbrich G, Halle M, BMBF Förderprogramm „Klinische Studien“

Modulation of Autonomic Nervous System
• Renal nerve ablation
• Vagal stimulation
• Spinal cord stimulation
• Baroreceptor stimulation

Zusammenfassung1. Diastolische Herzinsuffizienz wird zu wenig erkannt und zu
wenig therapiert
2. Dies liegt an unzureichendem pathophysiologischem Verständnis, dem Fehlen einheitlicher diagnostischer Kriterien, und der noch unzulänglichen Therapieoptionen
3. Die bisherigen Studien mit ARBs, ACE-Hemmern und Beta-Blocker nicht überzeugend
4. Neue Therapieoptionen in klinischer Prüfung: MR-Antagonisten, PDE-5-Hemmer, Neprilysin-Blockade, Körperliches Trainingsprogramm
5. „On the Edge“: Ranolazin, Ivabradin, sGuanylatzyklase-Stimulation, Devices (CRT, Autonome Modulation, intraatrialer Shunt)