Therapie des HER2 positiven metastasierten Mammakarzinoms · Therapie des HER2 positiven...
49
Therapie des HER2 positiven metastasierten Mammakarzinoms DGHO Stuttgart 3.10.2017 Jens Huober Univ.-Frauenklinik Ulm Integratives Tumorzentrum des Universitätsklinikums und der Medizinischen Fakultät Comprehensive Cancer Center Ulm
Transcript of Therapie des HER2 positiven metastasierten Mammakarzinoms · Therapie des HER2 positiven...

Therapie des HER2 positiven metastasierten Mammakarzinoms
DGHO Stuttgart
3.10.2017
Jens Huober
Univ.-Frauenklinik Ulm
Integratives Tumorzentrum des Universitätsklinikums
und der Medizinischen Fakultät
Comprehensive Cancer Center Ulm
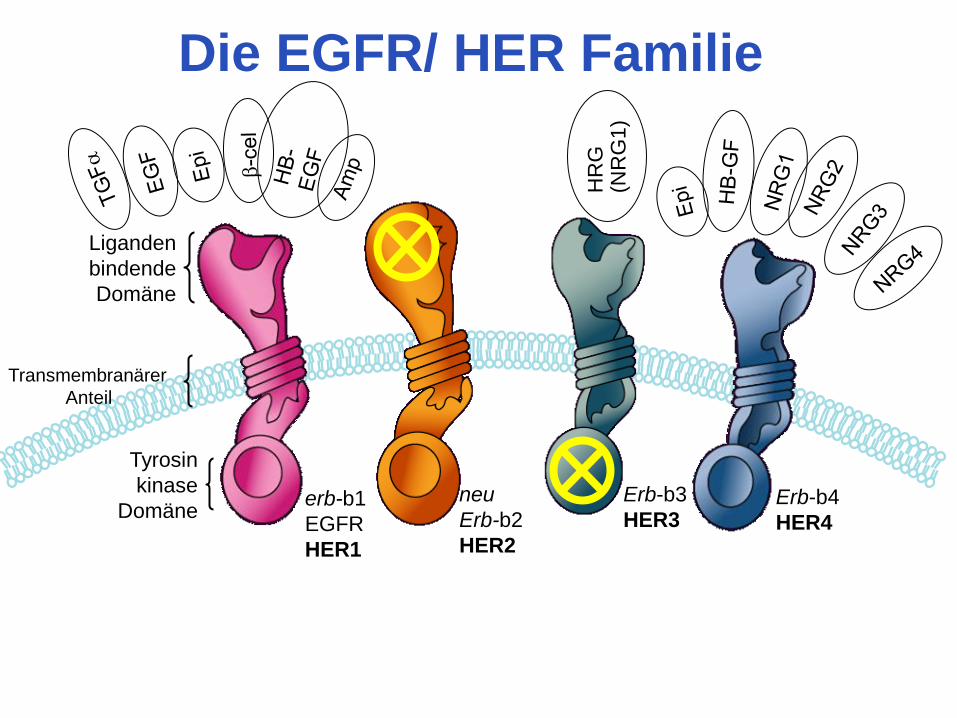
erb-b1
EGFR
HER1
neu
Erb-b2
HER2
Erb-b3
HER3 Erb-b4
HER4
HR
G
(NR
G1)
Tyrosin
kinase
Domäne
Liganden
bindende
Domäne
Transmembranärer
Anteil
Die EGFR/ HER Familie
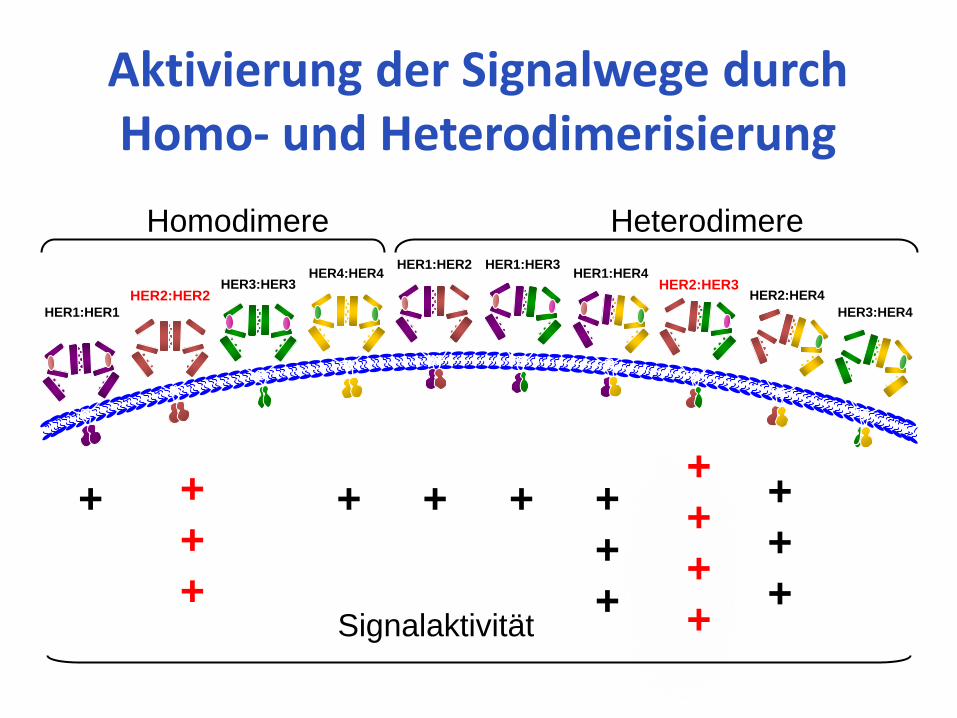
Homodimere Heterodimere
Aktivierung der Signalwege durch Homo- und Heterodimerisierung
HER1:HER1
HER2:HER2 HER3:HER3
HER4:HER4 HER1:HER2 HER1:HER3
HER1:HER4
HER2:HER4
HER3:HER4
+ + + + +
+
+
+
+
+
HER2:HER3
+
+
+
+
+
+
+ Signalaktivität
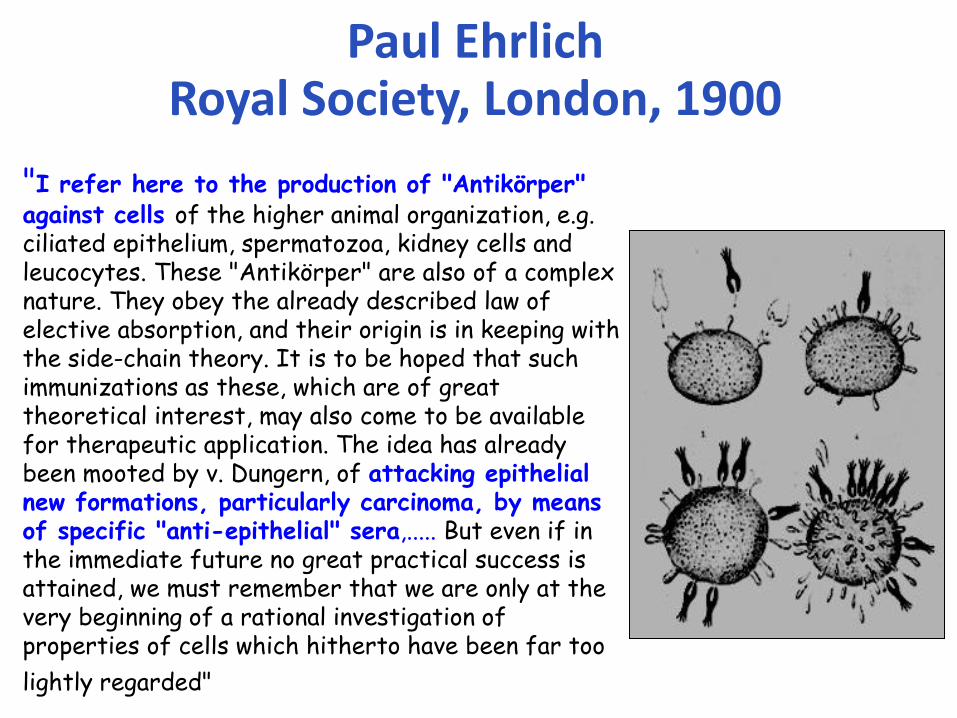
Paul Ehrlich Royal Society, London, 1900
"I refer here to the production of "Antikörper" against cells of the higher animal organization, e.g. ciliated epithelium, spermatozoa, kidney cells and leucocytes. These "Antikörper" are also of a complex nature. They obey the already described law of elective absorption, and their origin is in keeping with the side-chain theory. It is to be hoped that such immunizations as these, which are of great theoretical interest, may also come to be available for therapeutic application. The idea has already been mooted by v. Dungern, of attacking epithelial new formations, particularly carcinoma, by means of specific "anti-epithelial" sera,..... But even if in the immediate future no great practical success is attained, we must remember that we are only at the very beginning of a rational investigation of properties of cells which hitherto have been far too
lightly regarded"
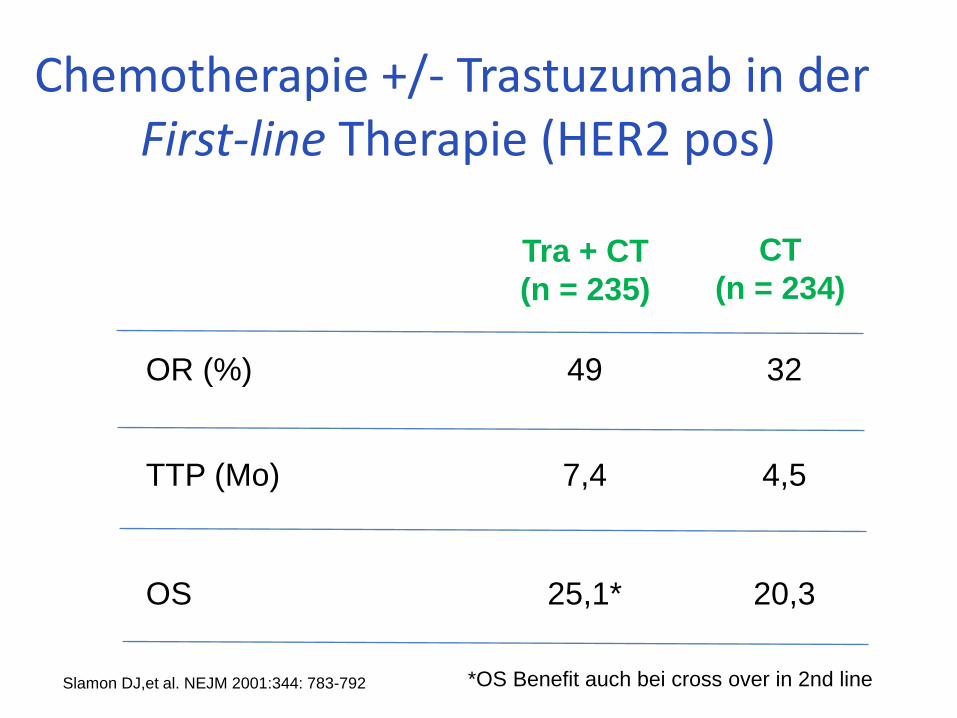
OR (%) 49 32
TTP (Mo) 7,4 4,5
OS 25,1* 20,3
Tra + CT
(n = 235)
CT
(n = 234)
Chemotherapie +/- Trastuzumab in der First-line Therapie (HER2 pos)
Slamon DJ,et al. NEJM 2001:344: 783-792 *OS Benefit auch bei cross over in 2nd line
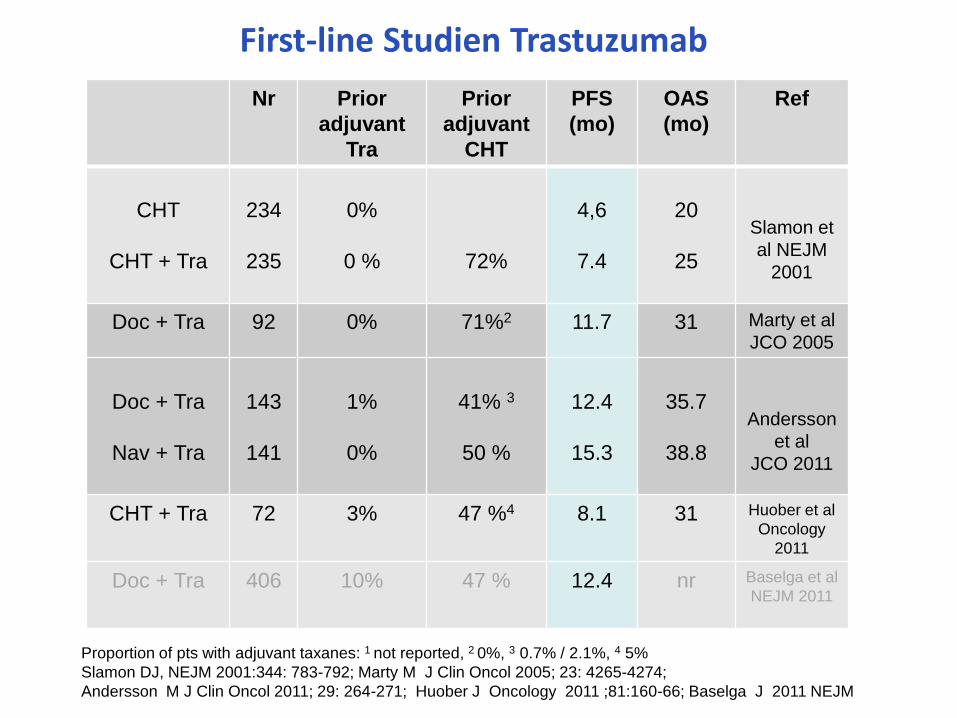
Nr Prior
adjuvant
Tra
Prior
adjuvant
CHT
PFS
(mo)
OAS
(mo)
Ref
CHT
CHT + Tra
234
235
0%
0 %
72%
4,6
7.4
20
25
Slamon et
al NEJM
2001
Doc + Tra 92 0% 71%2 11.7 31 Marty et al
JCO 2005
Doc + Tra
Nav + Tra
143
141
1%
0%
41% 3
50 %
12.4
15.3
35.7
38.8
Andersson
et al
JCO 2011
CHT + Tra 72 3% 47 %4 8.1 31 Huober et al
Oncology
2011
Doc + Tra 406 10% 47 % 12.4 nr Baselga et al
NEJM 2011
First-line Studien Trastuzumab
Proportion of pts with adjuvant taxanes: 1 not reported, 2 0%, 3 0.7% / 2.1%, 4 5%
Slamon DJ, NEJM 2001:344: 783-792; Marty M J Clin Oncol 2005; 23: 4265-4274;
Andersson M J Clin Oncol 2011; 29: 264-271; Huober J Oncology 2011 ;81:160-66; Baselga J 2011 NEJM
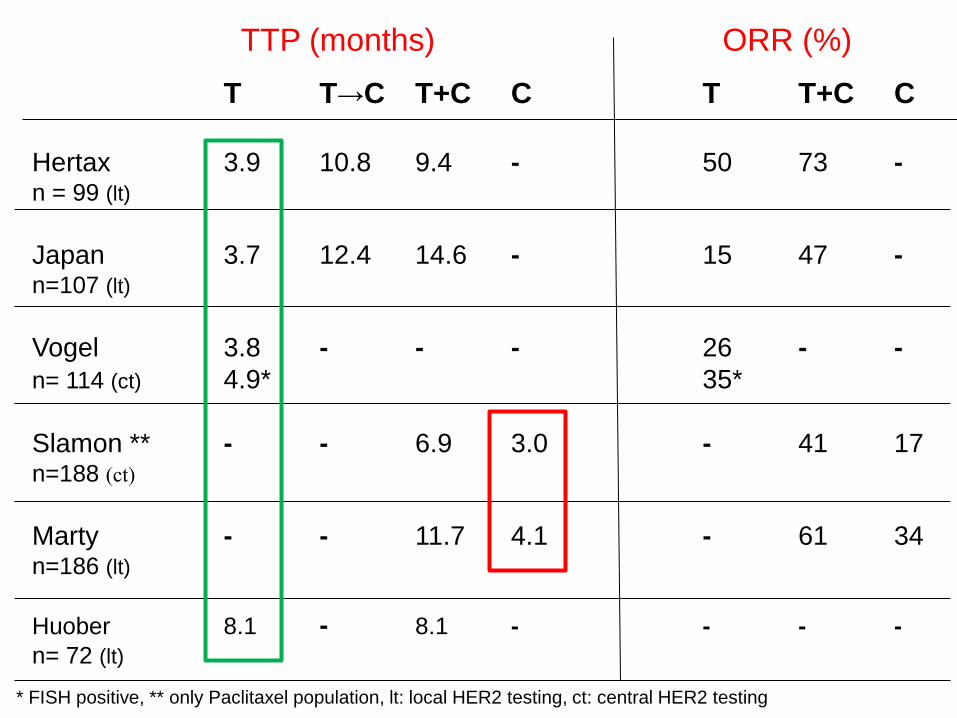
T T→C T+C C T T+C C
Hertax 3.9 10.8 9.4 - 50 73 - n = 99 (lt)
Japan 3.7 12.4 14.6 - 15 47 - n=107 (lt)
Vogel 3.8 - - - 26 - -
n= 114 (ct) 4.9* 35*
Slamon ** - - 6.9 3.0 - 41 17 n=188 (ct)
Marty - - 11.7 4.1 - 61 34 n=186 (lt)
Huober 8.1 - 8.1 - - - -
n= 72 (lt)
TTP (months) ORR (%)
* FISH positive, ** only Paclitaxel population, lt: local HER2 testing, ct: central HER2 testing
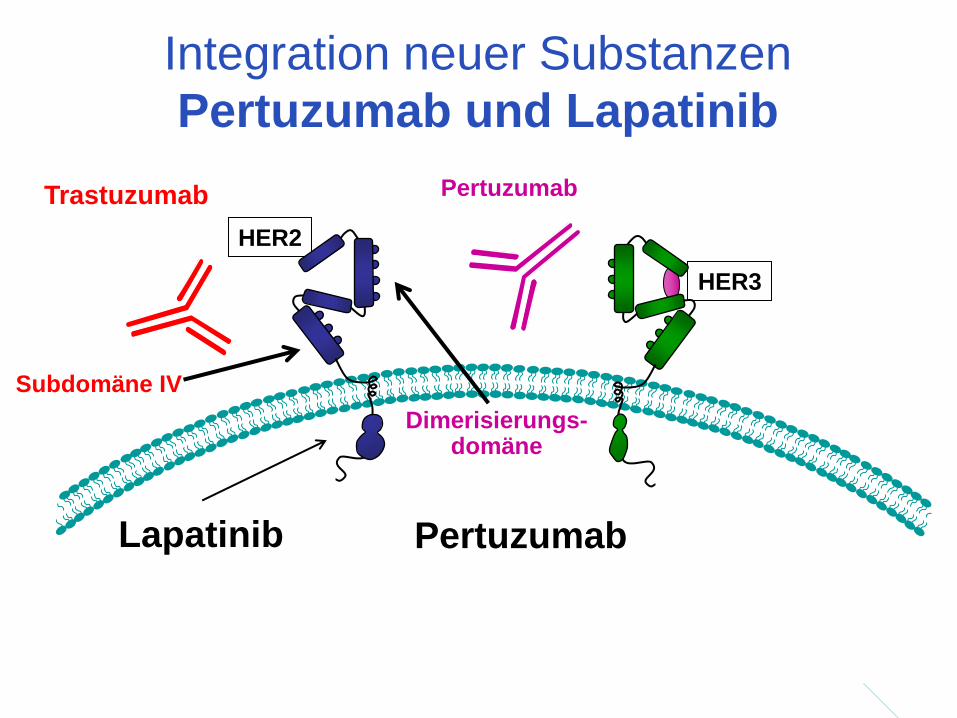
Integration neuer Substanzen
Pertuzumab und Lapatinib
HER2
Dimerisierungs- domäne
Pertuzumab
HER3
Trastuzumab
Subdomäne IV
Lapatinib Pertuzumab
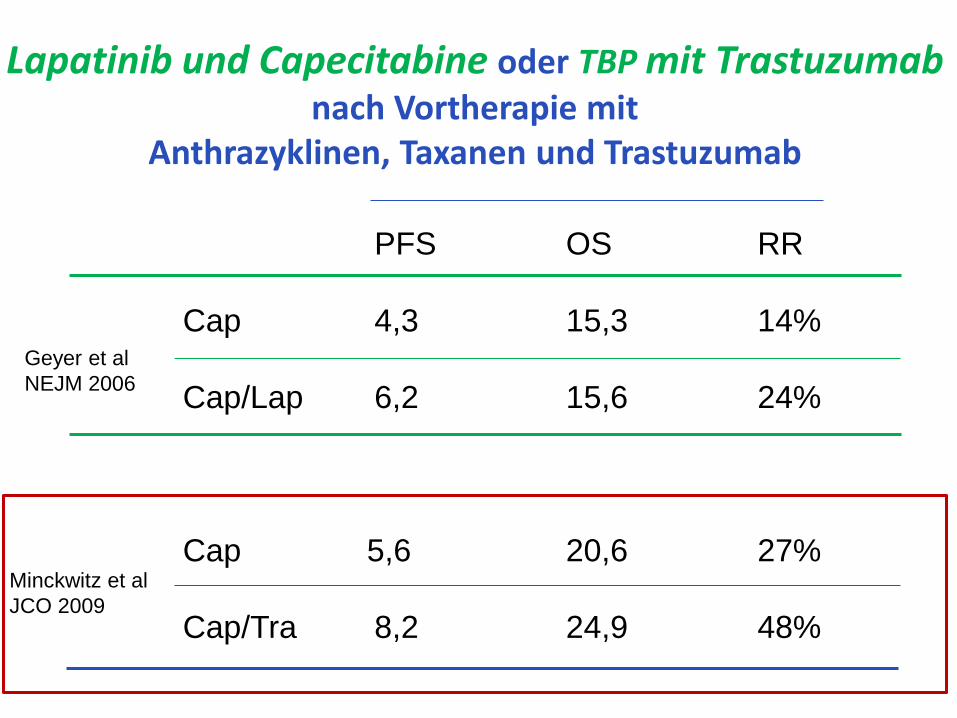
PFS OS RR
Cap 4,3 15,3 14%
Cap/Lap 6,2 15,6 24%
Cap 5,6 20,6 27%
Cap/Tra 8,2 24,9 48%
Geyer et al
NEJM 2006
Minckwitz et al
JCO 2009
Lapatinib und Capecitabine oder TBP mit Trastuzumab nach Vortherapie mit
Anthrazyklinen, Taxanen und Trastuzumab
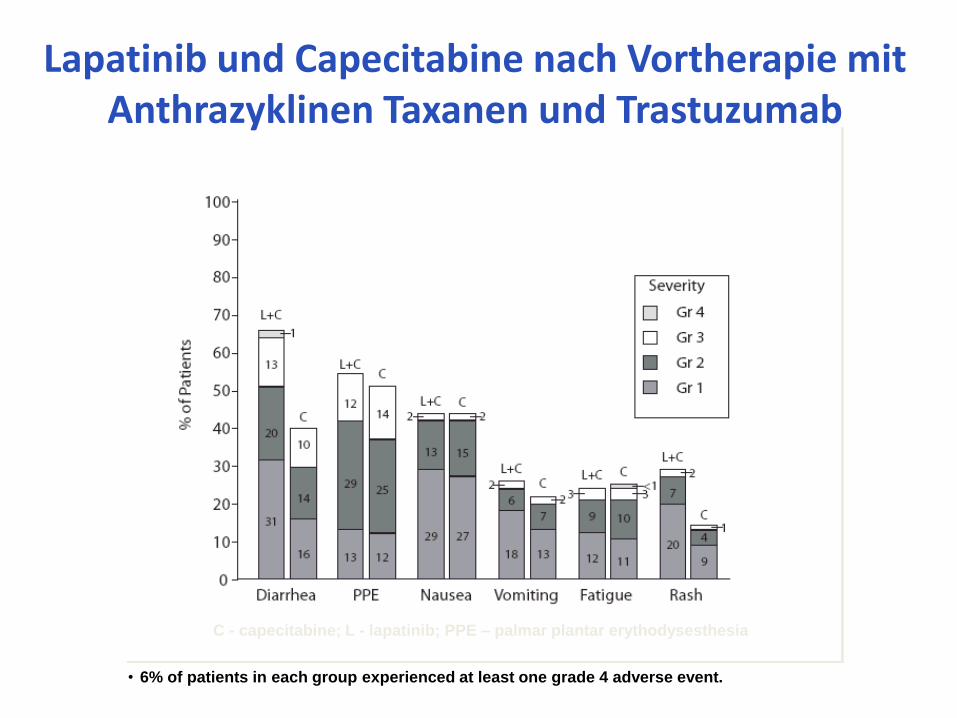
C - capecitabine; L - lapatinib; PPE – palmar plantar erythodysesthesia
• 6% of patients in each group experienced at least one grade 4 adverse event.
Lapatinib und Capecitabine nach Vortherapie mit Anthrazyklinen Taxanen und Trastuzumab
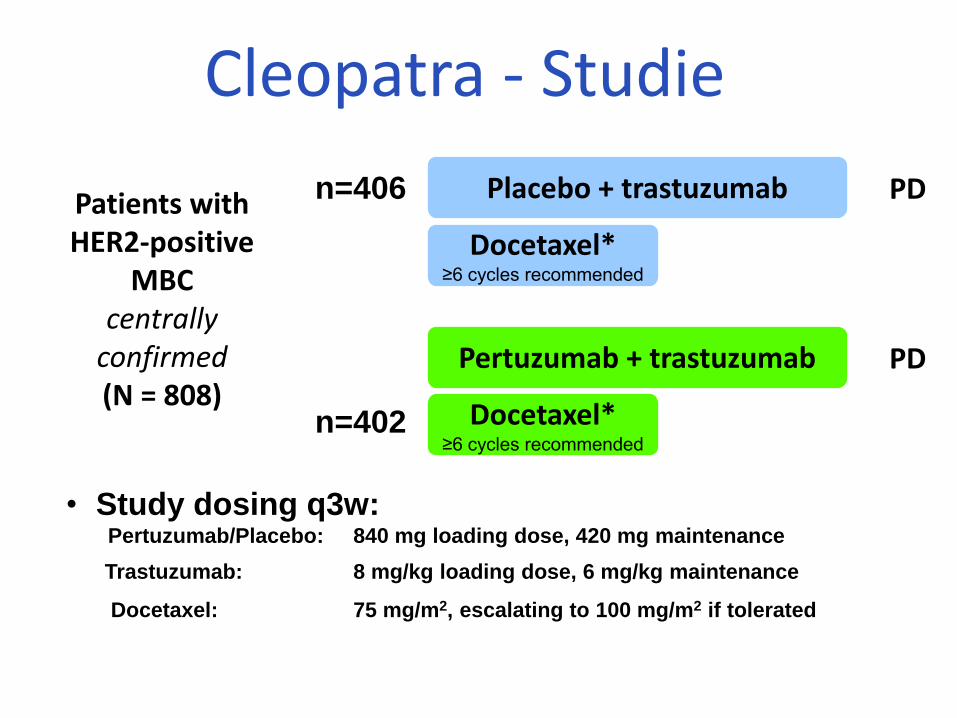
Cleopatra - Studie
Patients with HER2-positive
MBC centrally
confirmed (N = 808)
Placebo + trastuzumab n=406
• Study dosing q3w: Pertuzumab/Placebo: 840 mg loading dose, 420 mg maintenance
Trastuzumab: 8 mg/kg loading dose, 6 mg/kg maintenance
Docetaxel: 75 mg/m2, escalating to 100 mg/m2 if tolerated
1:1
n=402
Docetaxel* ≥6 cycles recommended
PD
Pertuzumab + trastuzumab
Docetaxel* ≥6 cycles recommended
PD
* <6 cycles allowed for unacceptable toxicity or PD; >6 cycles allowed at investigator discretion
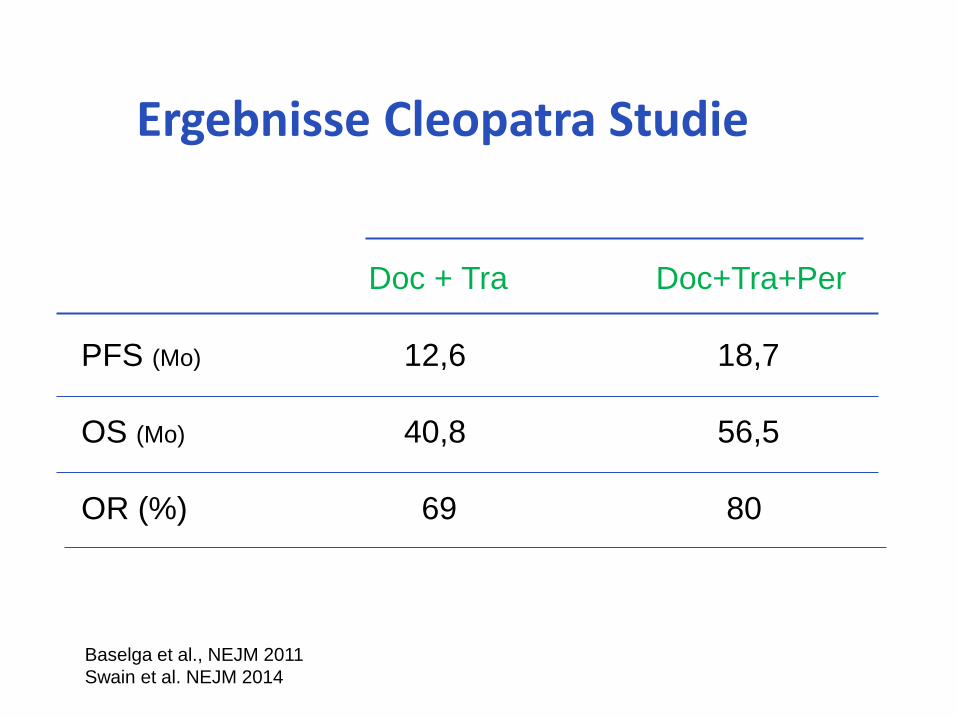
Doc + Tra Doc+Tra+Per
PFS (Mo) 12,6 18,7
OS (Mo) 40,8 56,5
OR (%) 69 80
Ergebnisse Cleopatra Studie
Baselga et al., NEJM 2011
Swain et al. NEJM 2014
Pro
gressio
nsfr
eie
s Ü
berle
ben
Monate Docetaxel Paclitaxel
nab-Paclitaxel
775 589 65
751 574 63
721 557 60
672 524 55
603 473 47
544 429 43
485 395 40
439 365 36
406 338 34
373 315 32
327 290 28
280 264 27
235 222 26
204 184 24
161 149 23
118 124 19
87 93 15
67 75 10
39 41 3
18 27 2
12 11 1
8 1 1
3 0 0
0 0 0
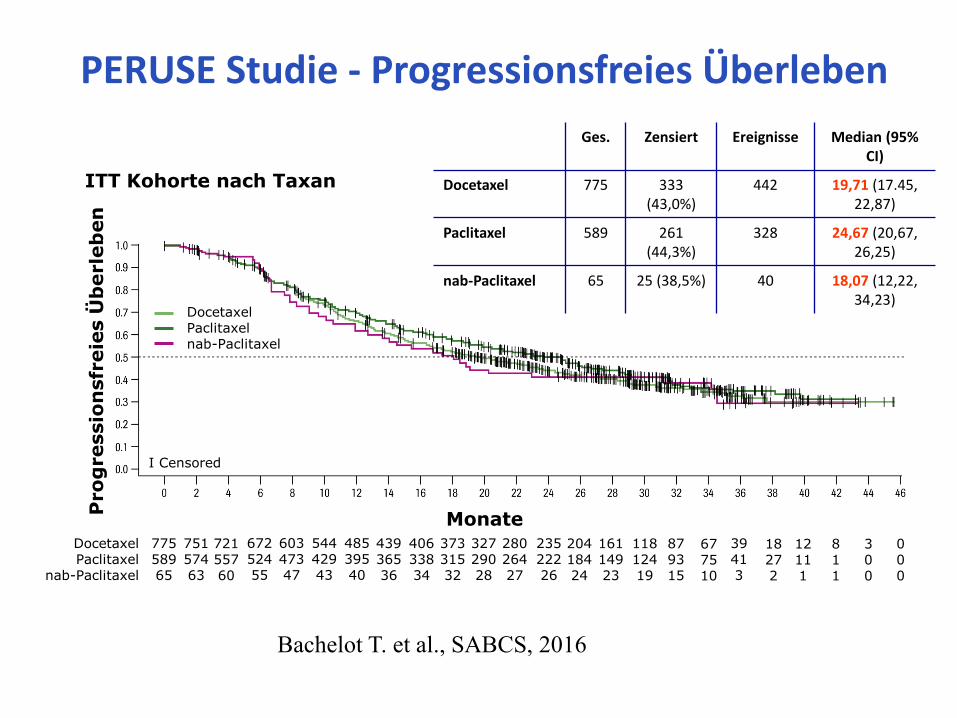
ITT Kohorte nach Taxan
Ges. Zensiert Ereignisse Median (95% CI)
Docetaxel 775 333 (43,0%)
442 19,71 (17.45, 22,87)
Paclitaxel 589 261 (44,3%)
328 24,67 (20,67, 26,25)
nab-Paclitaxel 65 25 (38,5%) 40 18,07 (12,22, 34,23)
Docetaxel Paclitaxel nab-Paclitaxel
I Censored
PERUSE Studie - Progressionsfreies Überleben
Bachelot T. et al., SABCS, 2016
© AGO e. V. in der DGGG e.V.
sowie
in der DKG e.V.
Guidelines Breast
Version 2017.1D
www.ago-online.de
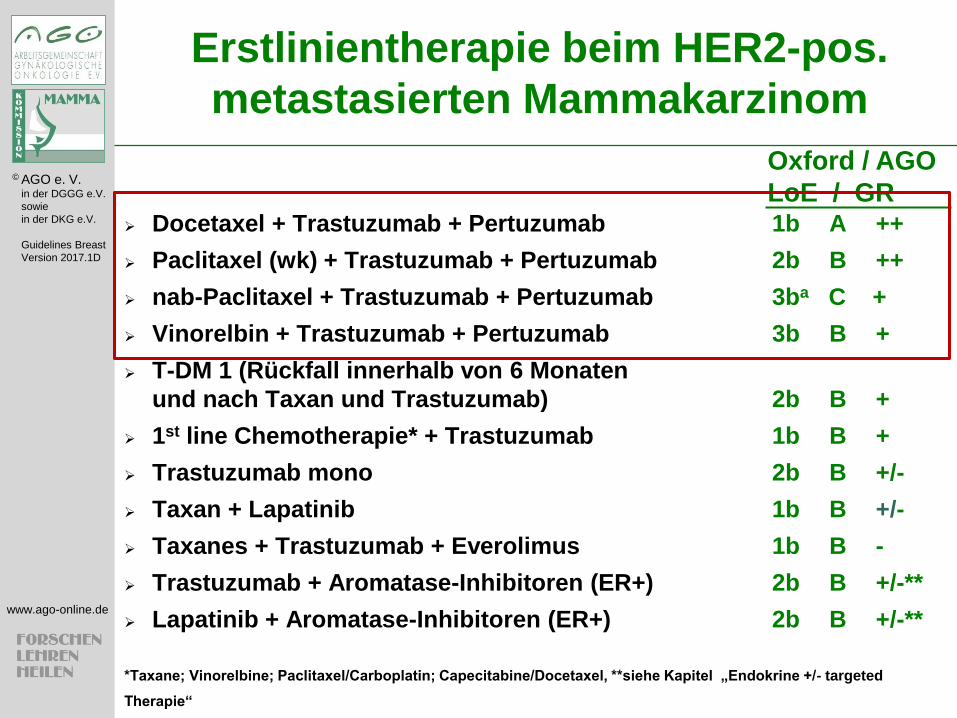
Erstlinientherapie beim HER2-pos.
metastasierten Mammakarzinom
Docetaxel + Trastuzumab + Pertuzumab 1b A ++
Paclitaxel (wk) + Trastuzumab + Pertuzumab 2b B ++
nab-Paclitaxel + Trastuzumab + Pertuzumab 3ba C +
Vinorelbin + Trastuzumab + Pertuzumab 3b B +
T-DM 1 (Rückfall innerhalb von 6 Monaten
und nach Taxan und Trastuzumab) 2b B +
1st line Chemotherapie* + Trastuzumab 1b B +
Trastuzumab mono 2b B +/-
Taxan + Lapatinib 1b B +/-
Taxanes + Trastuzumab + Everolimus 1b B -
Trastuzumab + Aromatase-Inhibitoren (ER+) 2b B +/-**
Lapatinib + Aromatase-Inhibitoren (ER+) 2b B +/-**
*Taxane; Vinorelbine; Paclitaxel/Carboplatin; Capecitabine/Docetaxel, **siehe Kapitel „Endokrine +/- targeted
Therapie“
Oxford / AGO
LoE / GR
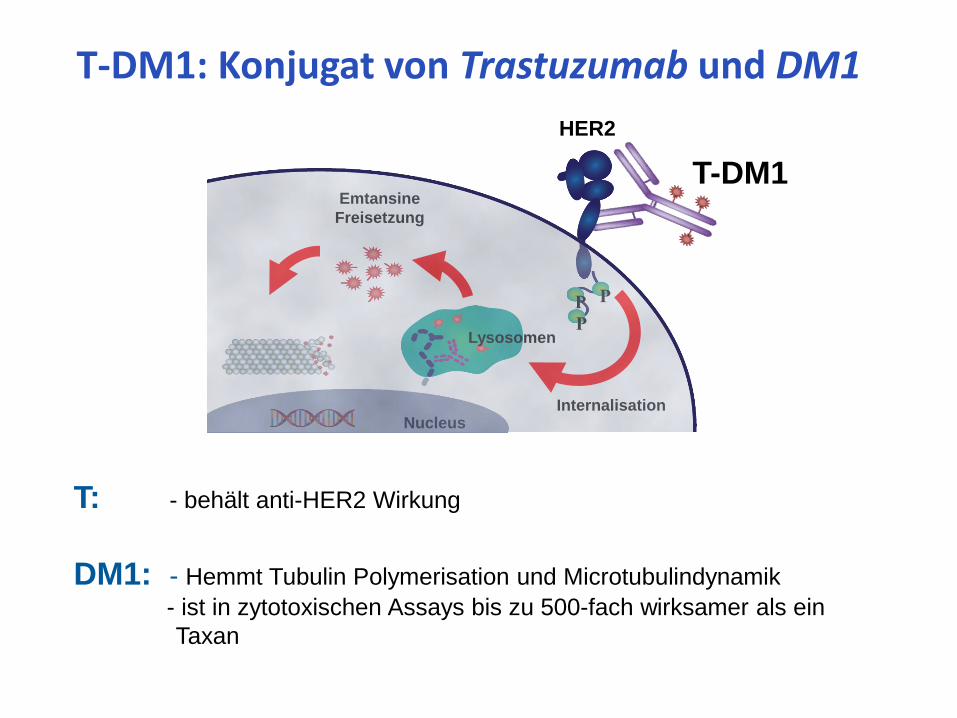
T: - behält anti-HER2 Wirkung
DM1: - Hemmt Tubulin Polymerisation und Microtubulindynamik
- ist in zytotoxischen Assays bis zu 500-fach wirksamer als ein
Taxan
T-DM1: Konjugat von Trastuzumab und DM1
Emtansine
Freisetzung
Internalisation
HER2
T-DM1
Lysosomen
Nucleus
P P
P
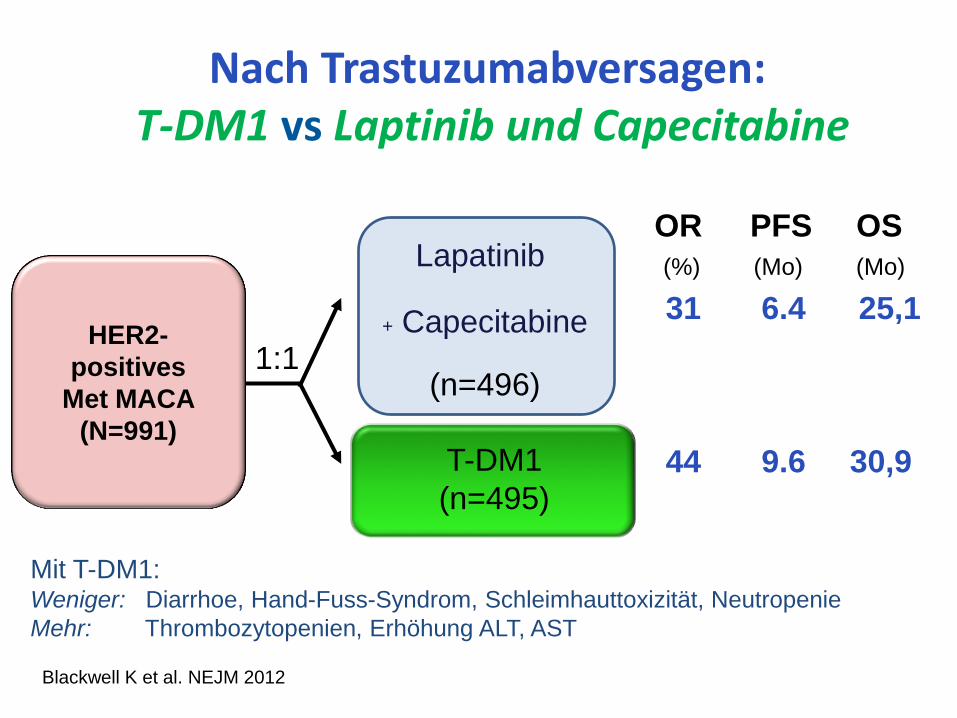
T-DM1
(n=495)
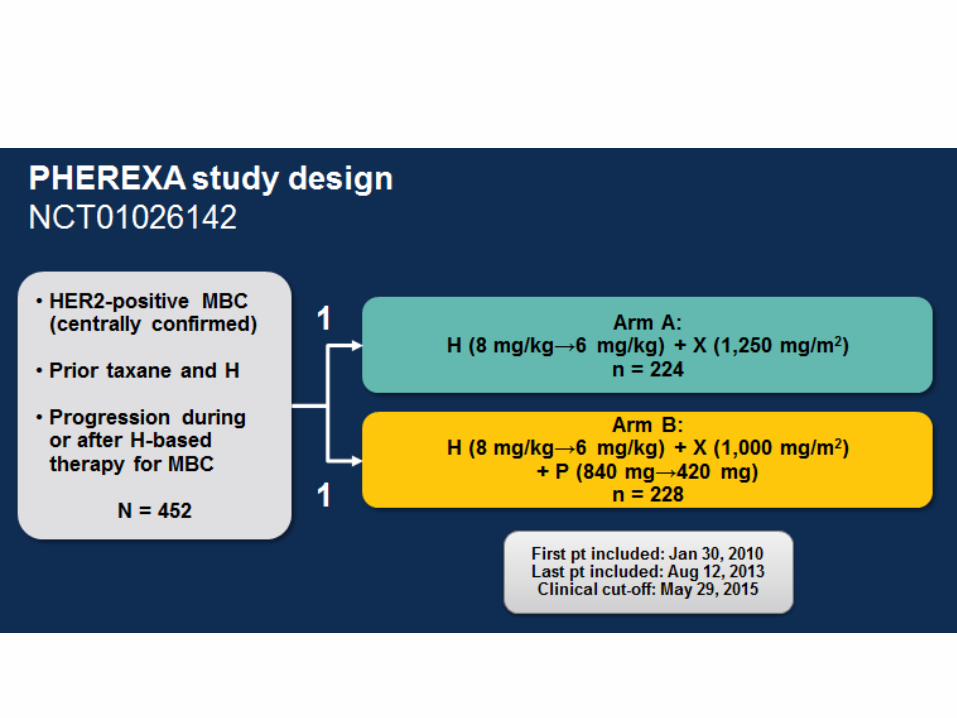
Nach Trastuzumabversagen: T-DM1 vs Laptinib und Capecitabine
1:1 HER2-
positives
Met MACA
(N=991)
Lapatinib
+ Capecitabine
(n=496)
31 6.4 25,1
44 9.6 30,9
Mit T-DM1: Weniger: Diarrhoe, Hand-Fuss-Syndrom, Schleimhauttoxizität, Neutropenie
Mehr: Thrombozytopenien, Erhöhung ALT, AST
OR PFS OS
(%) (Mo) (Mo)
Blackwell K et al. NEJM 2012
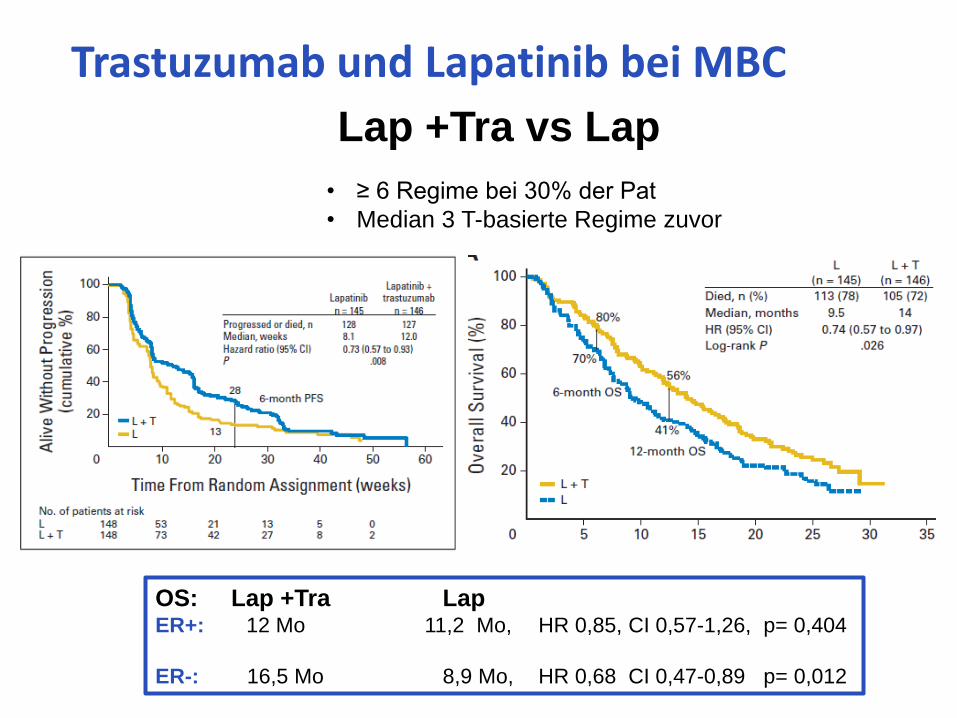
• ≥ 6 Regime bei 30% der Pat
• Median 3 T-basierte Regime zuvor
Trastuzumab und Lapatinib bei MBC
Lap +Tra vs Lap
OS: Lap +Tra Lap ER+: 12 Mo 11,2 Mo, HR 0,85, CI 0,57-1,26, p= 0,404
ER-: 16,5 Mo 8,9 Mo, HR 0,68 CI 0,47-0,89 p= 0,012
© AGO e. V. in der DGGG e.V.
sowie
in der DKG e.V.
Guidelines Breast
Version 2017.1D
www.ago-online.de
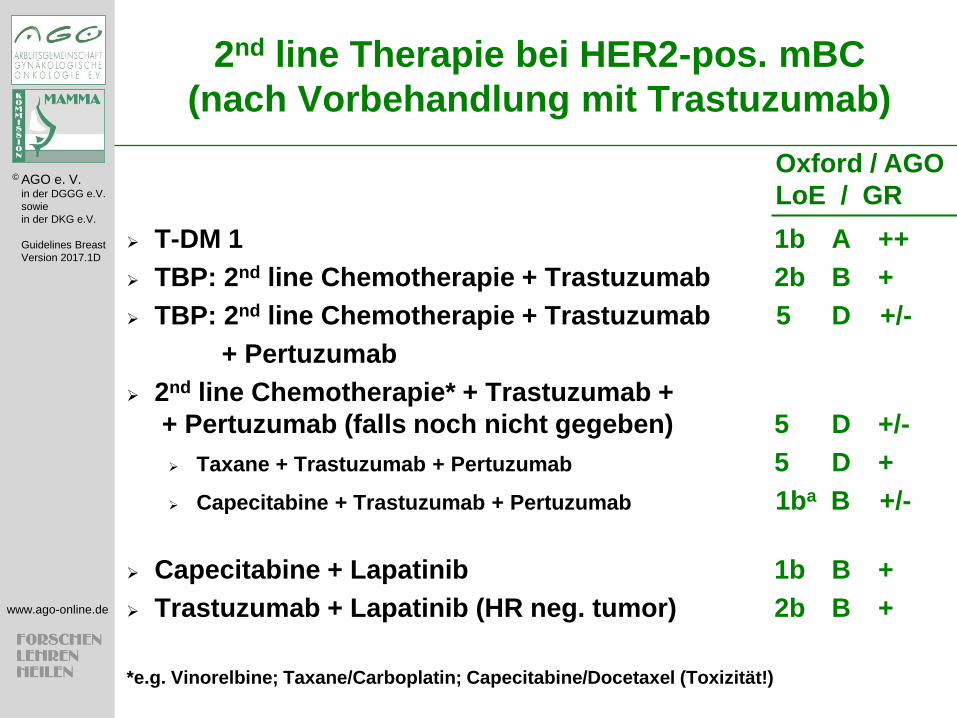
2nd line Therapie bei HER2-pos. mBC
(nach Vorbehandlung mit Trastuzumab)
T-DM 1 1b A ++
TBP: 2nd line Chemotherapie + Trastuzumab 2b B +
TBP: 2nd line Chemotherapie + Trastuzumab 5 D +/-
+ Pertuzumab
2nd line Chemotherapie* + Trastuzumab +
+ Pertuzumab (falls noch nicht gegeben) 5 D +/-
Taxane + Trastuzumab + Pertuzumab 5 D +
Capecitabine + Trastuzumab + Pertuzumab 1ba B +/-
Capecitabine + Lapatinib 1b B +
Trastuzumab + Lapatinib (HR neg. tumor) 2b B +
*e.g. Vinorelbine; Taxane/Carboplatin; Capecitabine/Docetaxel (Toxizität!)
Oxford / AGO
LoE / GR
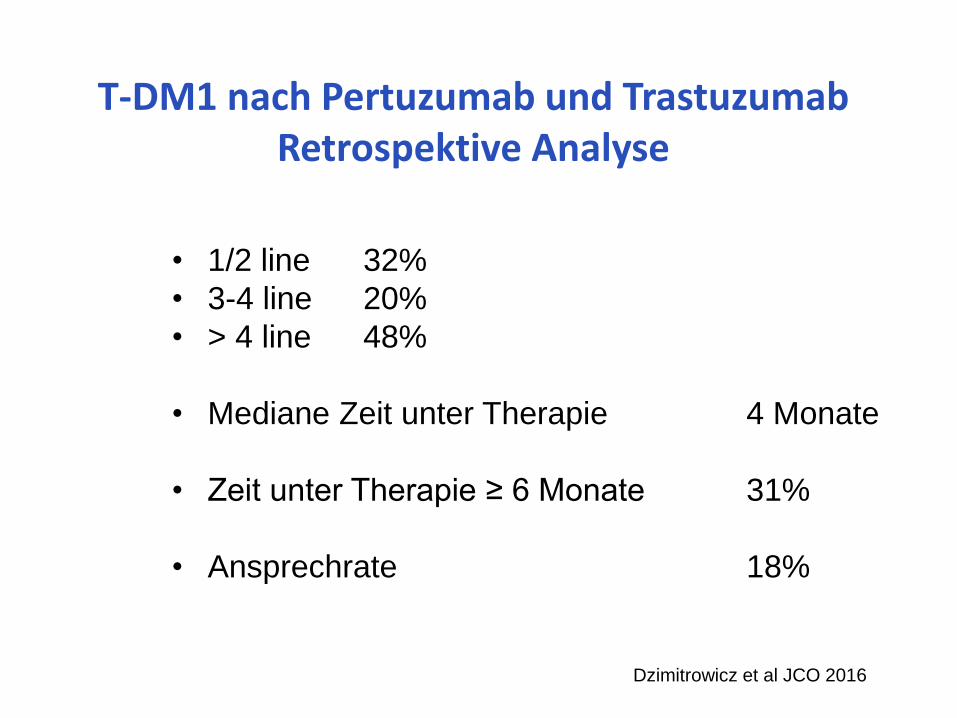
T-DM1 nach Pertuzumab und Trastuzumab Retrospektive Analyse
• 1/2 line 32%
• 3-4 line 20%
• > 4 line 48%
• Mediane Zeit unter Therapie 4 Monate
• Zeit unter Therapie ≥ 6 Monate 31%
• Ansprechrate 18%
Dzimitrowicz et al JCO 2016
Duale HER2
Blockade
Brauchen wir
noch
Chemotherapie?
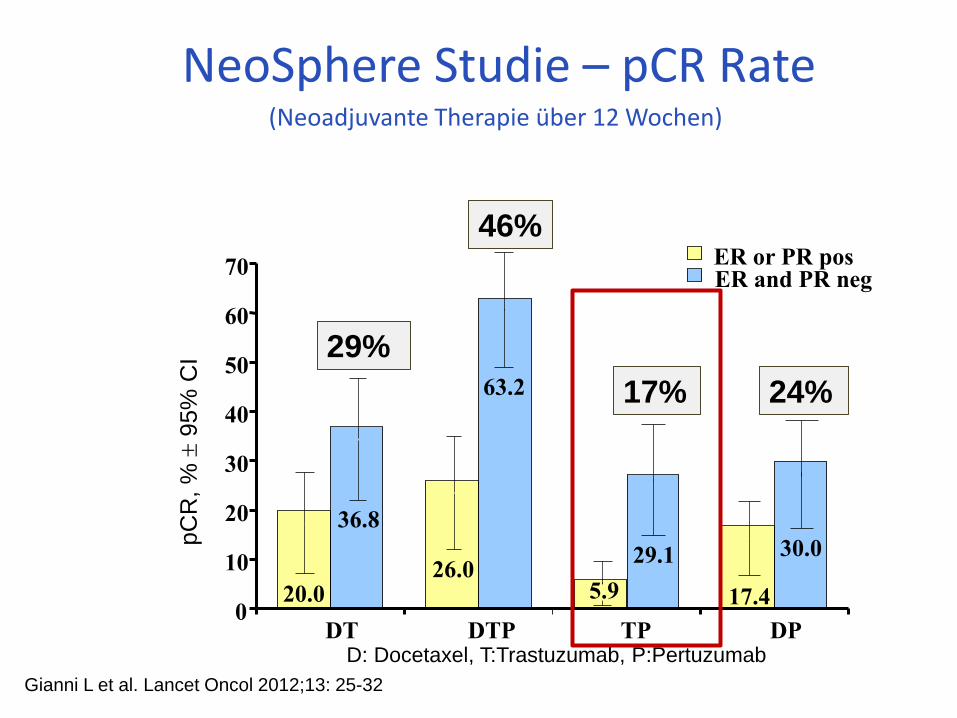
NeoSphere Studie – pCR Rate (Neoadjuvante Therapie über 12 Wochen)
0
10
20
30
40
50
60
70
DT DTP TP DP
ER or PR pos ER and PR neg
20.0 26.0
17.4
36.8
29.1 30.0
63.2
5.9
pC
R,
%
95%
CI 29%
46%
17% 24%
D: Docetaxel, T:Trastuzumab, P:Pertuzumab
Gianni L et al. Lancet Oncol 2012;13: 25-32
SABCS 2014
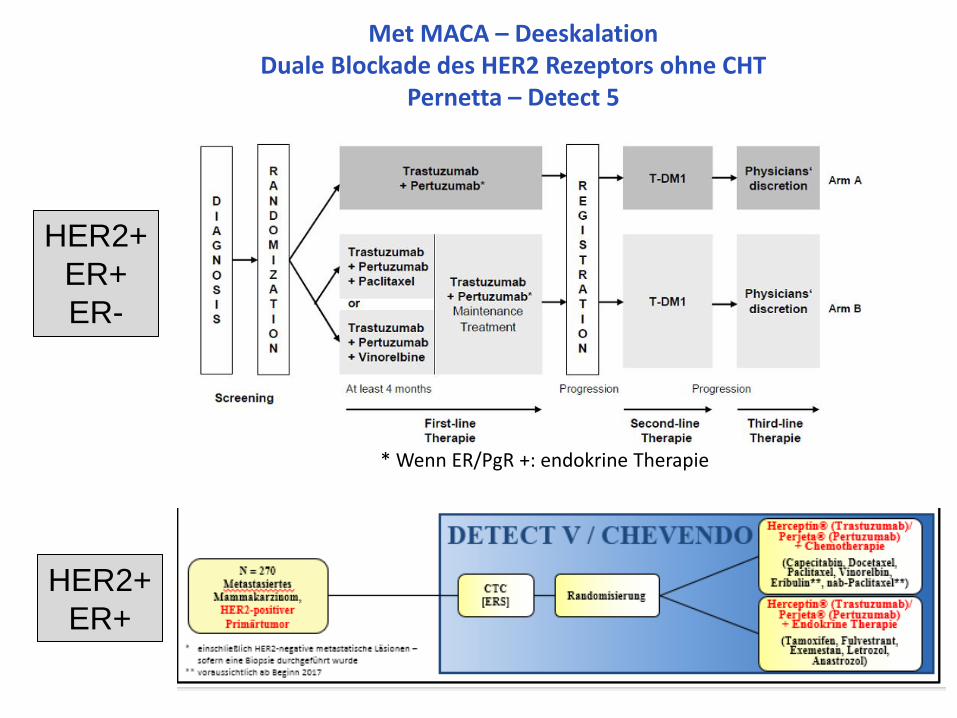
Met MACA – Deeskalation Duale Blockade des HER2 Rezeptors ohne CHT
Pernetta – Detect 5
* Wenn ER/PgR +: endokrine Therapie
HER2+
ER+
ER-
HER2+
ER+
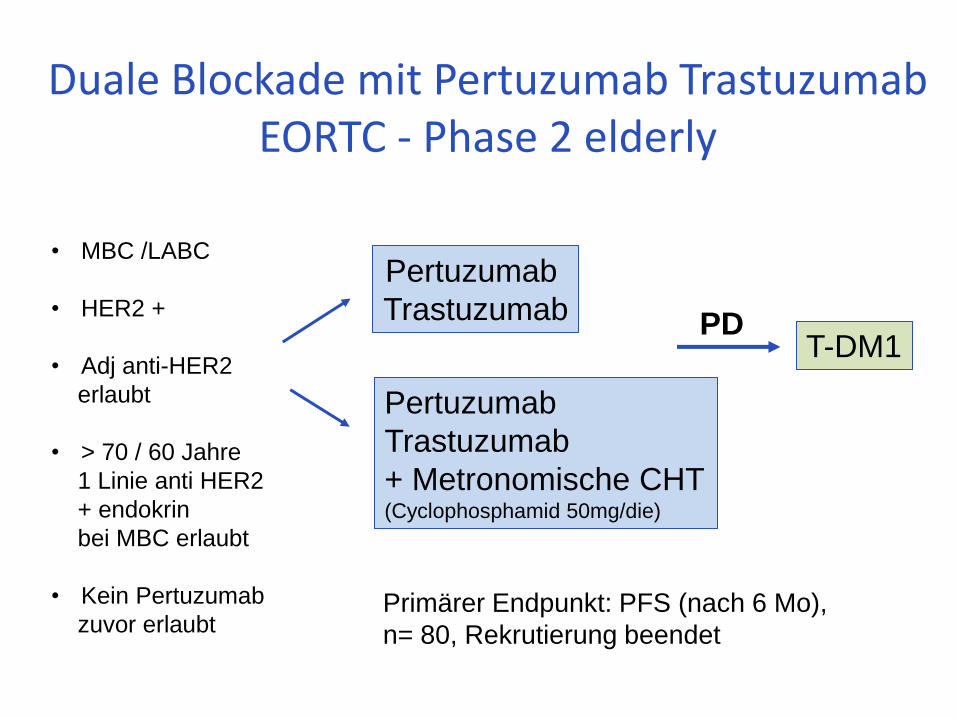
Duale Blockade mit Pertuzumab Trastuzumab EORTC - Phase 2 elderly
Pertuzumab
Trastuzumab
Pertuzumab
Trastuzumab
+ Metronomische CHT (Cyclophosphamid 50mg/die)
• MBC /LABC
• HER2 +
• Adj anti-HER2
erlaubt
• > 70 / 60 Jahre
1 Linie anti HER2
+ endokrin
bei MBC erlaubt
• Kein Pertuzumab
zuvor erlaubt
T-DM1 PD
Primärer Endpunkt: PFS (nach 6 Mo),
n= 80, Rekrutierung beendet
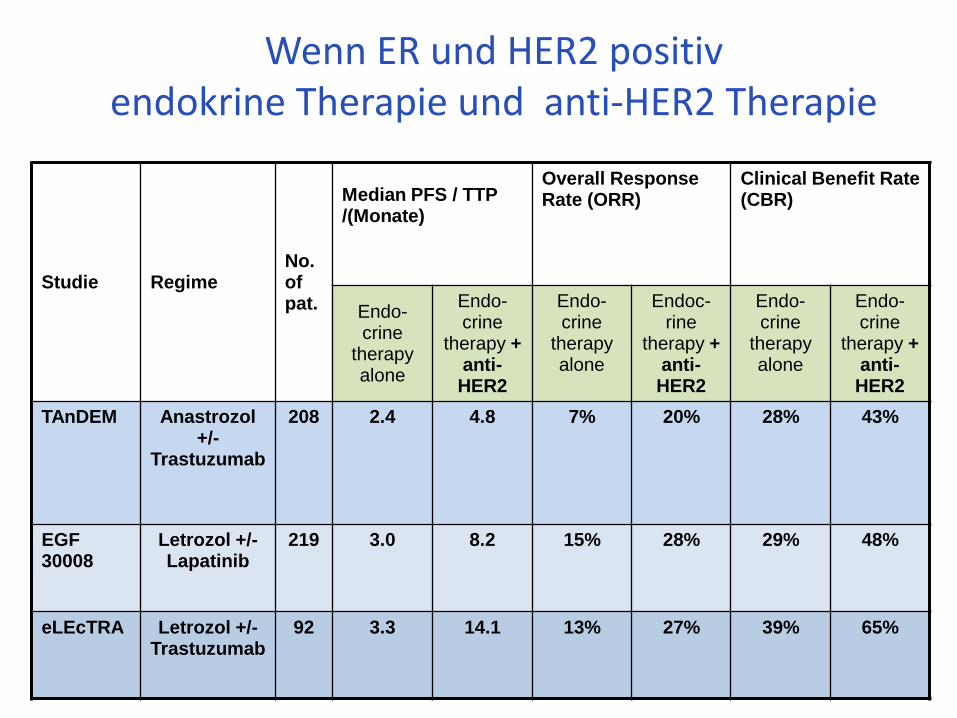
Wenn ER und HER2 positiv endokrine Therapie und anti-HER2 Therapie
Studie Regime No. of pat.
Median PFS / TTP /(Monate)
Overall Response Rate (ORR)
Clinical Benefit Rate (CBR)
Endo-crine
therapy alone
Endo-crine
therapy + anti-HER2
Endo-crine
therapy alone
Endoc-rine
therapy + anti-HER2
Endo-crine
therapy alone
Endo-crine
therapy + anti-HER2
TAnDEM Anastrozol +/-
Trastuzumab
208 2.4 4.8 7% 20% 28% 43%
EGF 30008
Letrozol +/- Lapatinib
219 3.0 8.2 15% 28% 29% 48%
eLEcTRA Letrozol +/- Trastuzumab
92 3.3 14.1 13% 27% 39% 65%
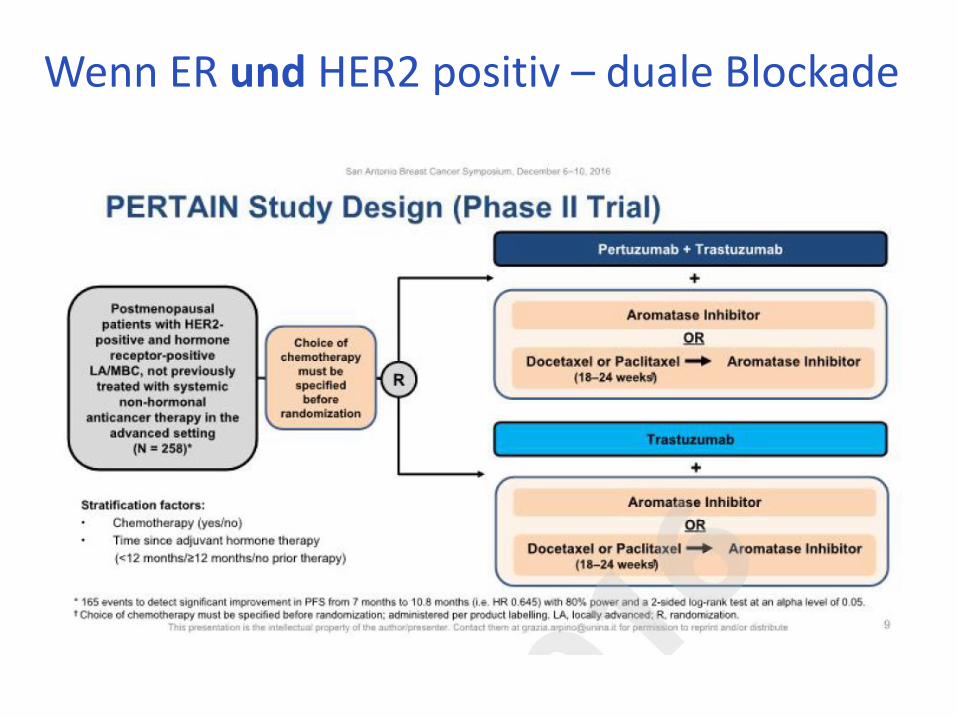
Wenn ER und HER2 positiv – duale Blockade

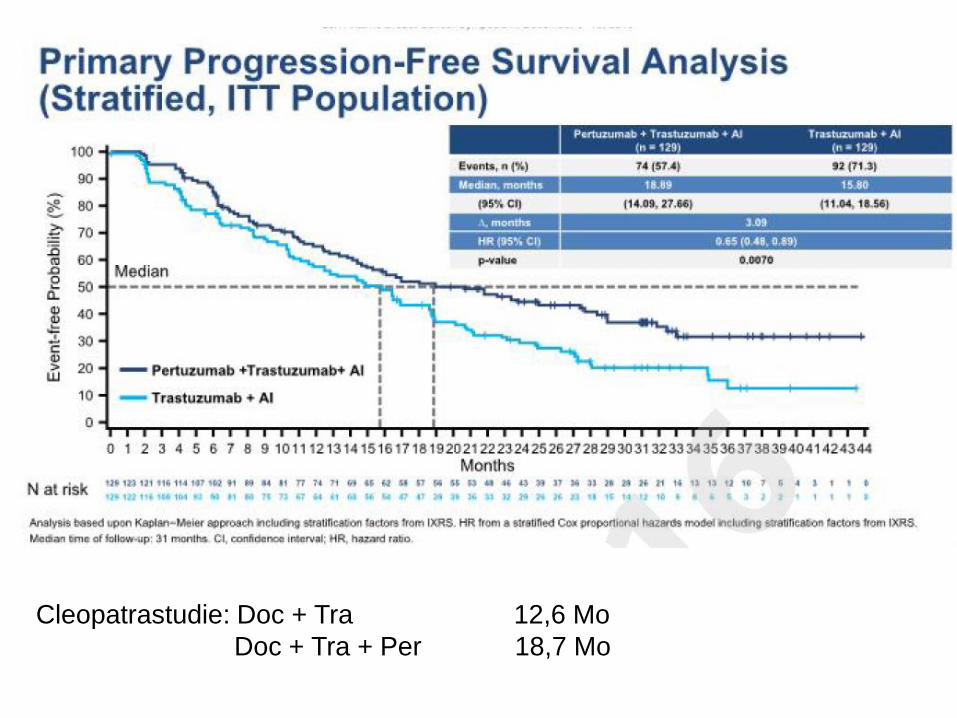
Cleopatrastudie: Doc + Tra 12,6 Mo
Doc + Tra + Per 18,7 Mo
0
100
200
300
400
500
600
700
800
900
1000
MB-175
ZR75
-30
CAMA-1
MB13
4
HCC20
2
UACC-893
EFM
19
SUM19
0
EFM
192A
MB-361
HCC15
00
HCC14
19
HCC38
MB-415
MCF-
10A
UACC-812
HCC22
18
ZR75
-1
MDAMB45
3
184A
1
T47D
MCF7
BT-
20
MDAMB43
5
BT4
74
SKBR3
KPL-
1
HCC11
43
MDAMB23
1
HCC13
95
SUM-225
HS57
8T
184B
5
UACC73
2
CAL-51
BT5
49
COLO
824
DU44
75
HCC11
87
HCC15
69
HCC18
06
HCC19
37
HCC19
54
HCC70
MB-436
MB15
7
MDAMB46
8
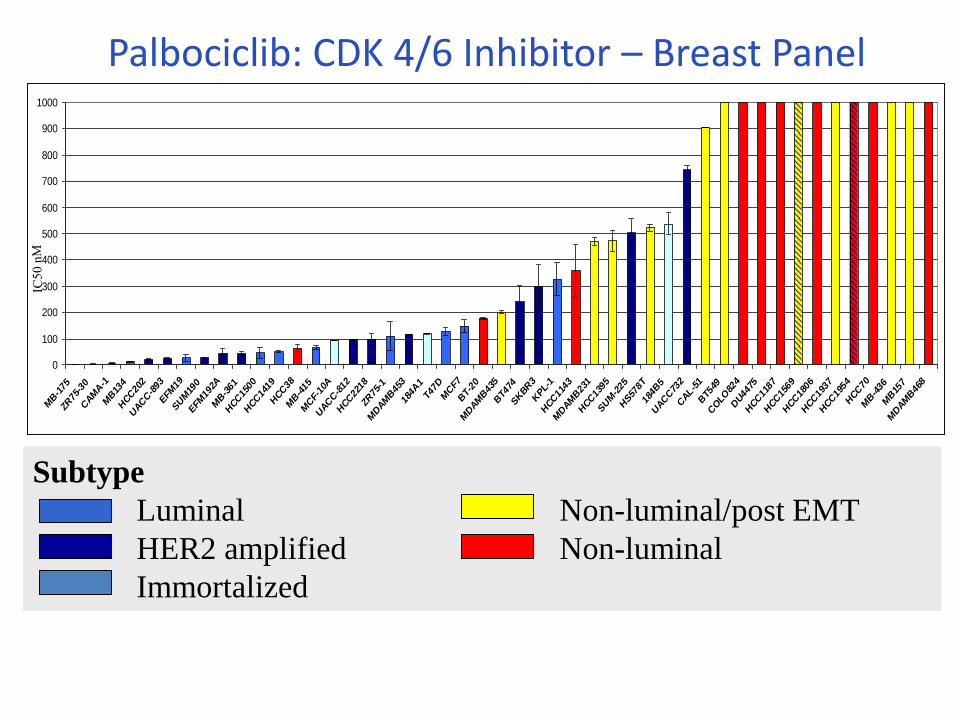
Subtype
Luminal Non-luminal/post EMT
HER2 amplified Non-luminal
Immortalized
Palbociclib: CDK 4/6 Inhibitor – Breast Panel
Finn RS, et al. Breast Cancer Res. 2009;11(5):R77.
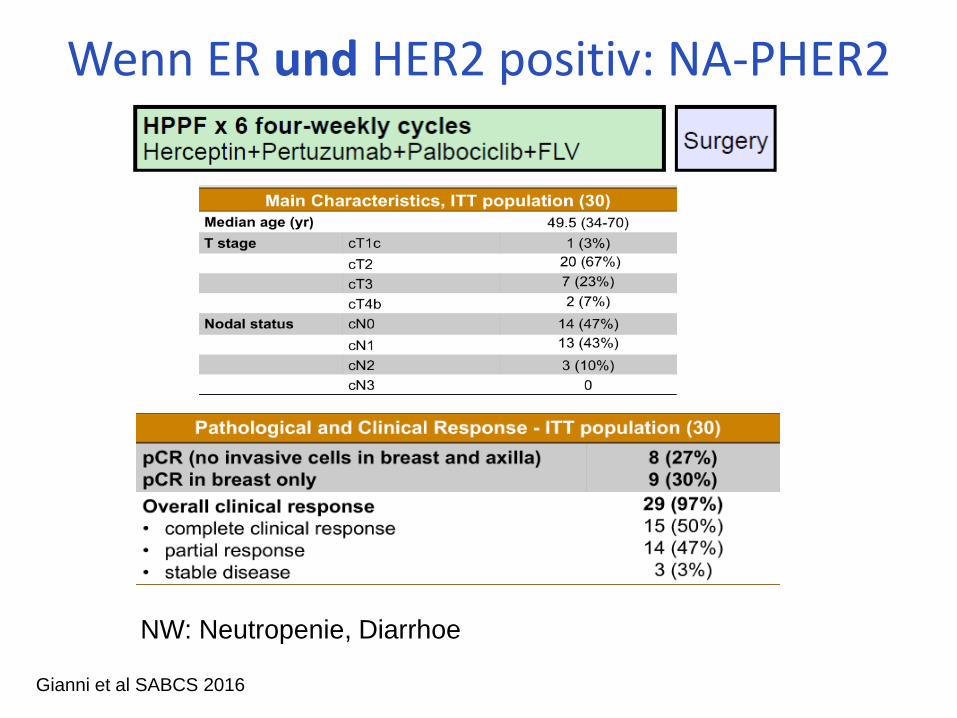
Wenn ER und HER2 positiv: NA-PHER2
Gianni et al SABCS 2016
NW: Neutropenie, Diarrhoe
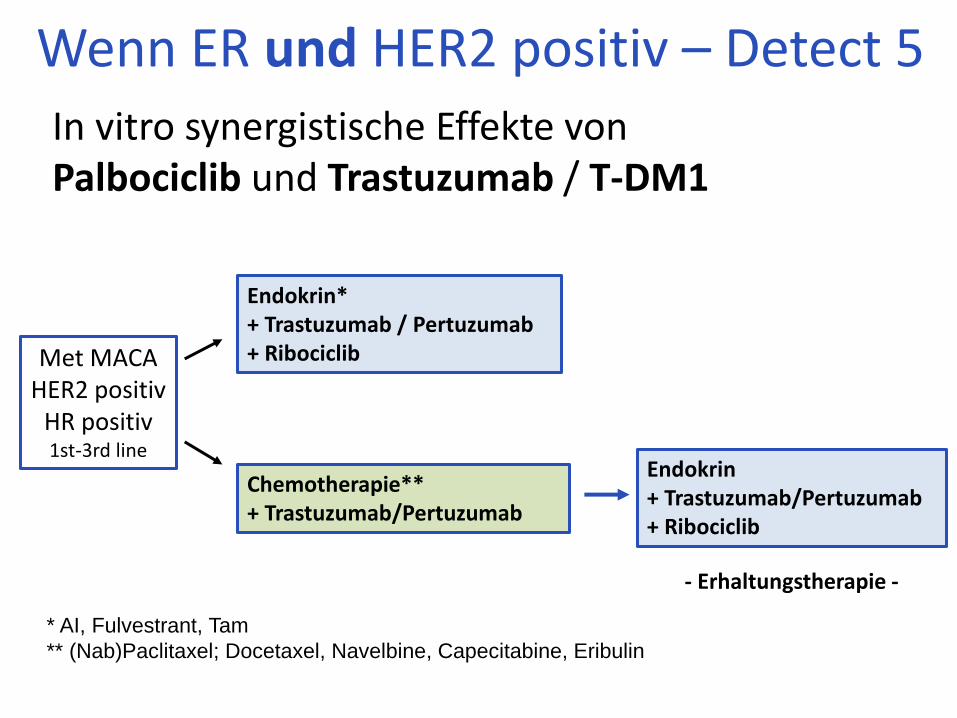
In vitro synergistische Effekte von Palbociclib und Trastuzumab / T-DM1
Met MACA HER2 positiv
HR positiv 1st-3rd line
Endokrin* + Trastuzumab / Pertuzumab + Ribociclib
Chemotherapie** + Trastuzumab/Pertuzumab
* AI, Fulvestrant, Tam
** (Nab)Paclitaxel; Docetaxel, Navelbine, Capecitabine, Eribulin
Wenn ER und HER2 positiv – Detect 5
Endokrin + Trastuzumab/Pertuzumab + Ribociclib
- Erhaltungstherapie -

HER2 Therapie
Neue
Substanzen
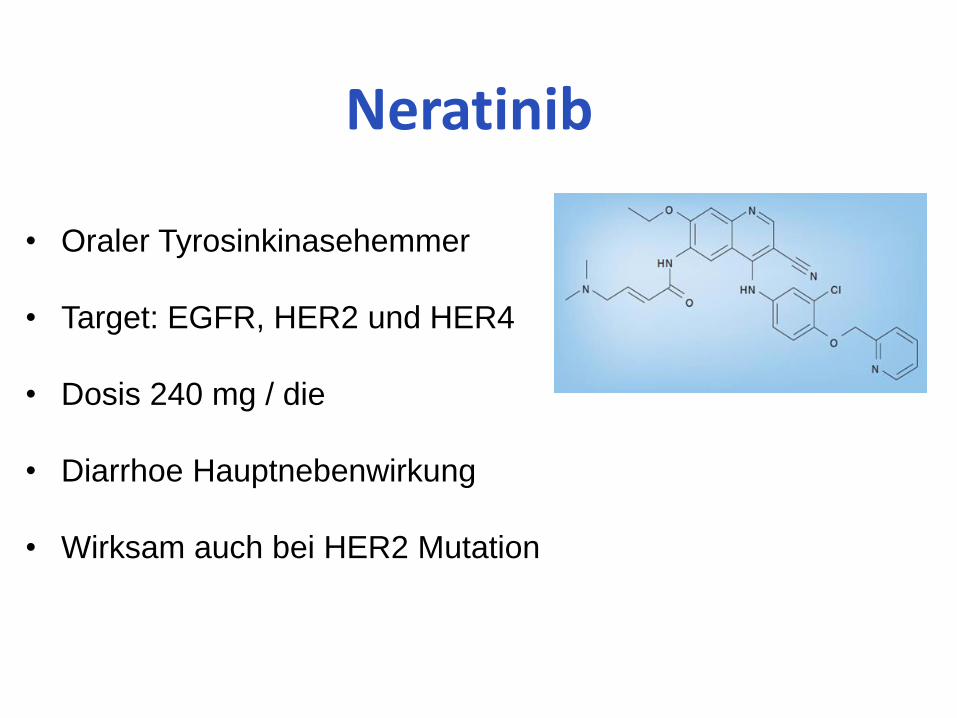
Neratinib
• Oraler Tyrosinkinasehemmer
• Target: EGFR, HER2 und HER4
• Dosis 240 mg / die
• Diarrhoe Hauptnebenwirkung
• Wirksam auch bei HER2 Mutation
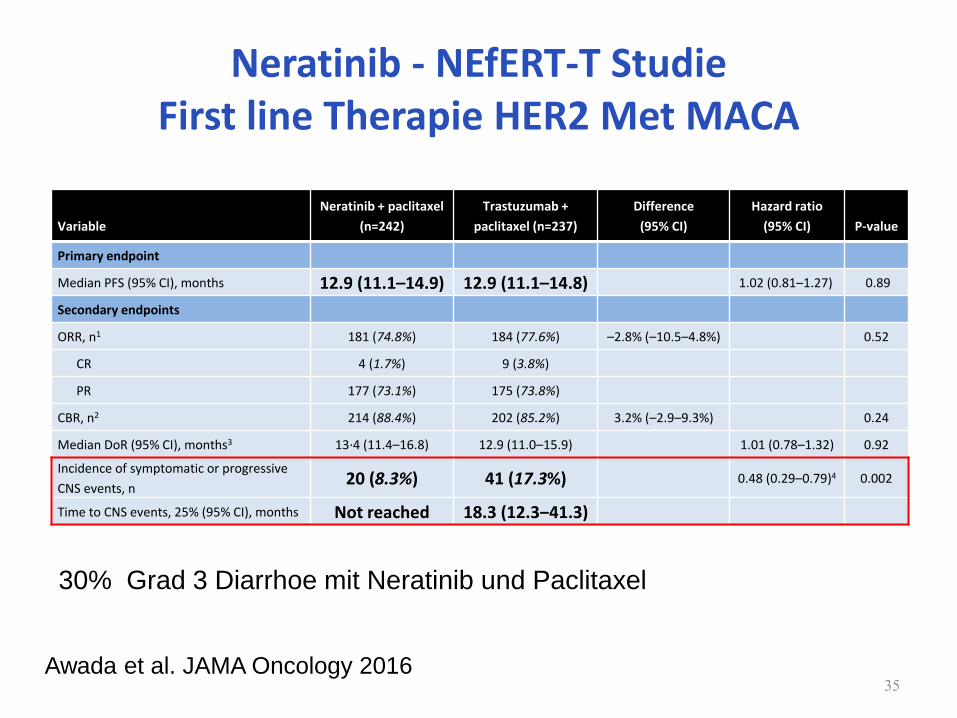
Neratinib - NEfERT-T Studie First line Therapie HER2 Met MACA
Variable
Neratinib + paclitaxel
(n=242)
Trastuzumab +
paclitaxel (n=237)
Difference
(95% CI)
Hazard ratio
(95% CI)
P-value
Primary endpoint
Median PFS (95% CI), months 12.9 (11.1–14.9) 12.9 (11.1–14.8) 1.02 (0.81–1.27) 0.89
Secondary endpoints
ORR, n1 181 (74.8%) 184 (77.6%) –2.8% (–10.5–4.8%) 0.52
CR 4 (1.7%) 9 (3.8%)
PR 177 (73.1%) 175 (73.8%)
CBR, n2 214 (88.4%) 202 (85.2%) 3.2% (–2.9–9.3%) 0.24
Median DoR (95% CI), months3 13·4 (11.4–16.8) 12.9 (11.0–15.9) 1.01 (0.78–1.32) 0.92
Incidence of symptomatic or progressive
CNS events, n 20 (8.3%) 41 (17.3%) 0.48 (0.29–0.79)4 0.002
Time to CNS events, 25% (95% CI), months Not reached 18.3 (12.3‒41.3)
35 Awada et al. JAMA Oncology 2016
30% Grad 3 Diarrhoe mit Neratinib und Paclitaxel
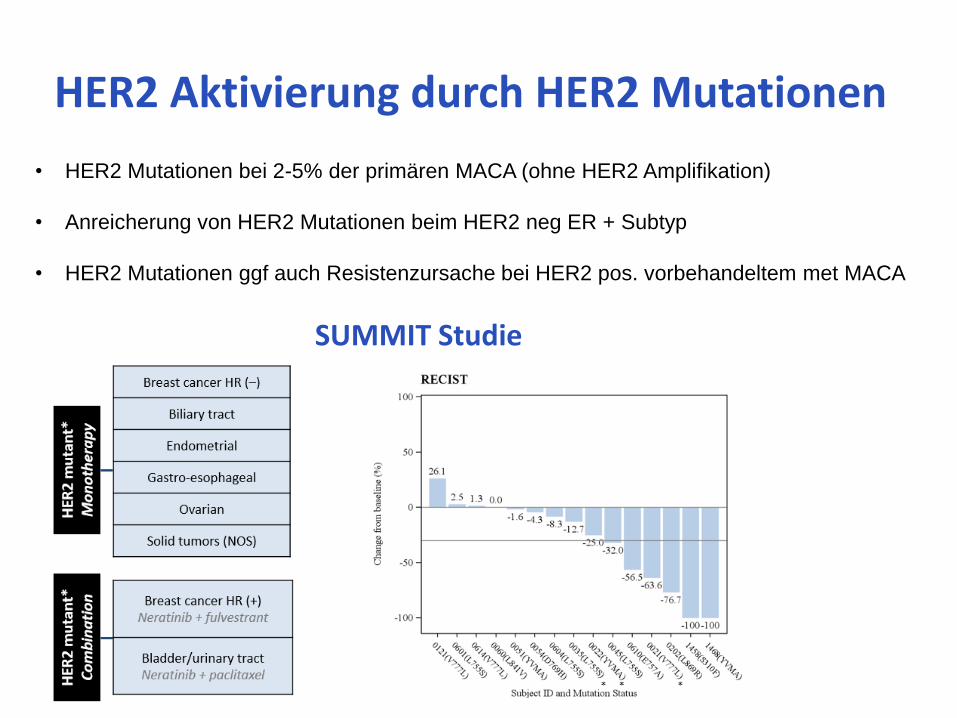
HER2 Aktivierung durch HER2 Mutationen
• HER2 Mutationen bei 2-5% der primären MACA (ohne HER2 Amplifikation)
• Anreicherung von HER2 Mutationen beim HER2 neg ER + Subtyp
• HER2 Mutationen ggf auch Resistenzursache bei HER2 pos. vorbehandeltem met MACA
SUMMIT Studie
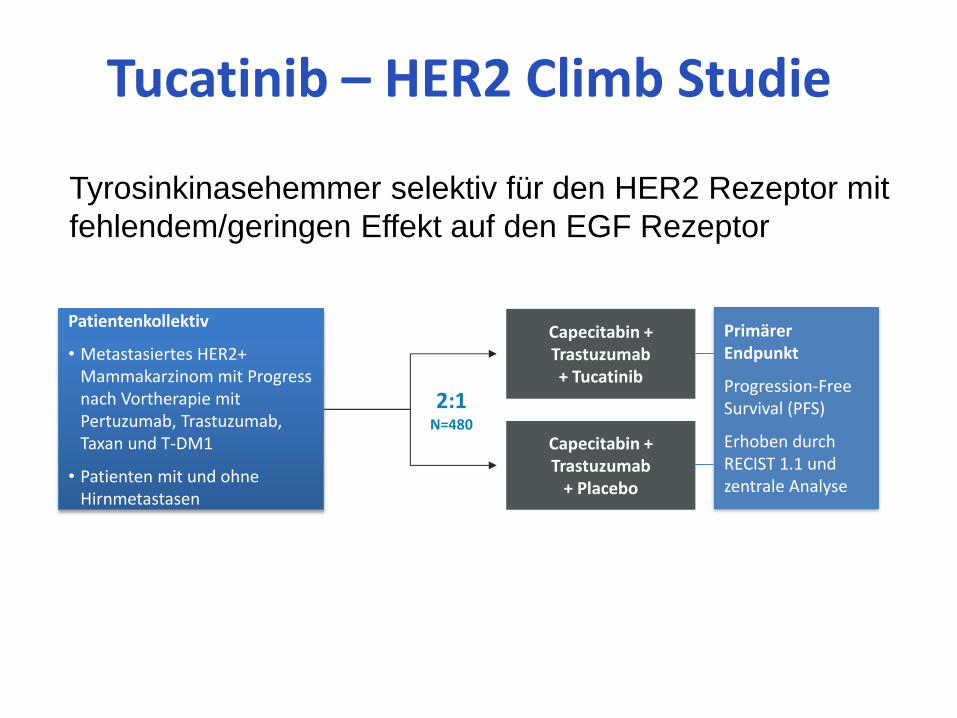
Tucatinib – HER2 Climb Studie
Tyrosinkinasehemmer selektiv für den HER2 Rezeptor mit
fehlendem/geringen Effekt auf den EGF Rezeptor
Patientenkollektiv
• Metastasiertes HER2+ Mammakarzinom mit Progress nach Vortherapie mit Pertuzumab, Trastuzumab, Taxan und T-DM1
• Patienten mit und ohne Hirnmetastasen
Capecitabin + Trastuzumab + Tucatinib
2:1 N=480
Capecitabin + Trastuzumab
+ Placebo
Primärer Endpunkt
Progression-Free Survival (PFS)
Erhoben durch RECIST 1.1 und zentrale Analyse
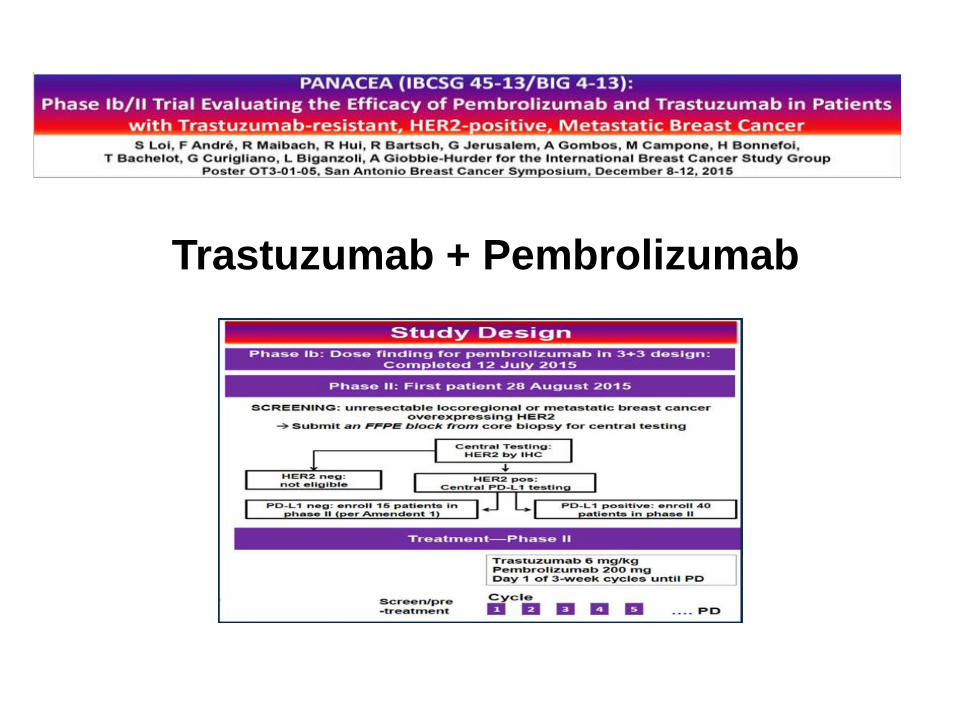
Trastuzumab + Pembrolizumab
• Der Nachweis des HER2 Rezeptors und die Entwicklung der
anti HER2 Therapie haben das HER2 positive MACA als
separaten Subtyp etabliert und die Therapie fundamental
geändert
• Eine Vielzahl neuer Substanzen und Kombinationen
(mit CDK4/6 Inhibitoren/Checkointinhibitoren) sind
vielversprechende Ansätze
• Deeskalation mit Verzicht auf CHT bei effektiver „targeted“ Therapie
• Ggf. mehr ZNS Kontrolle durch neue Substanzen?
Zusammenfassung

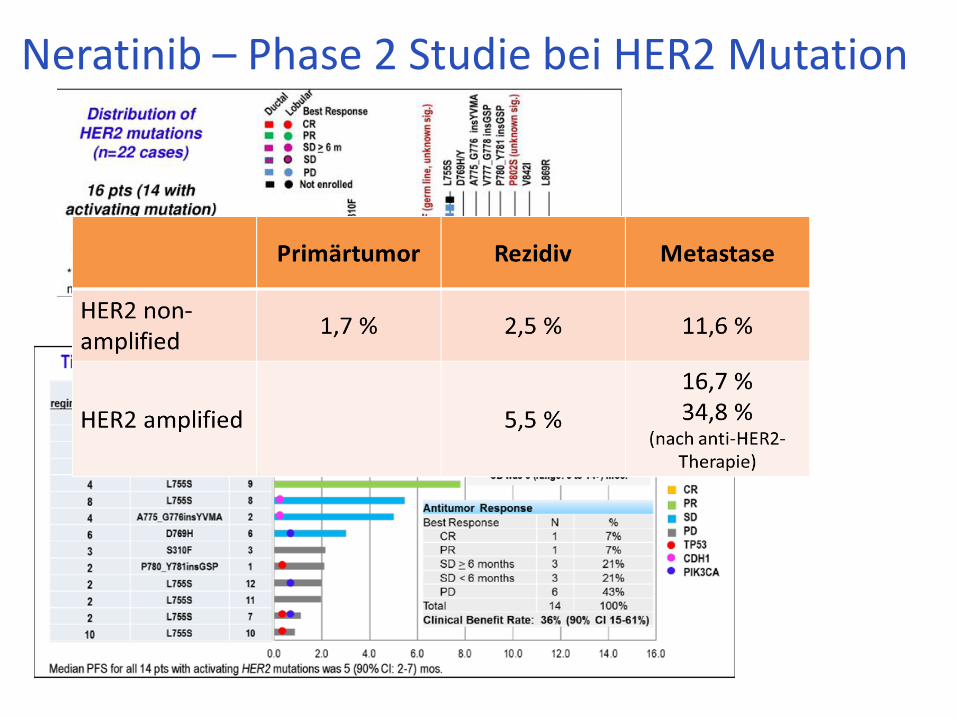
Neratinib – Phase 2 Studie bei HER2 Mutation
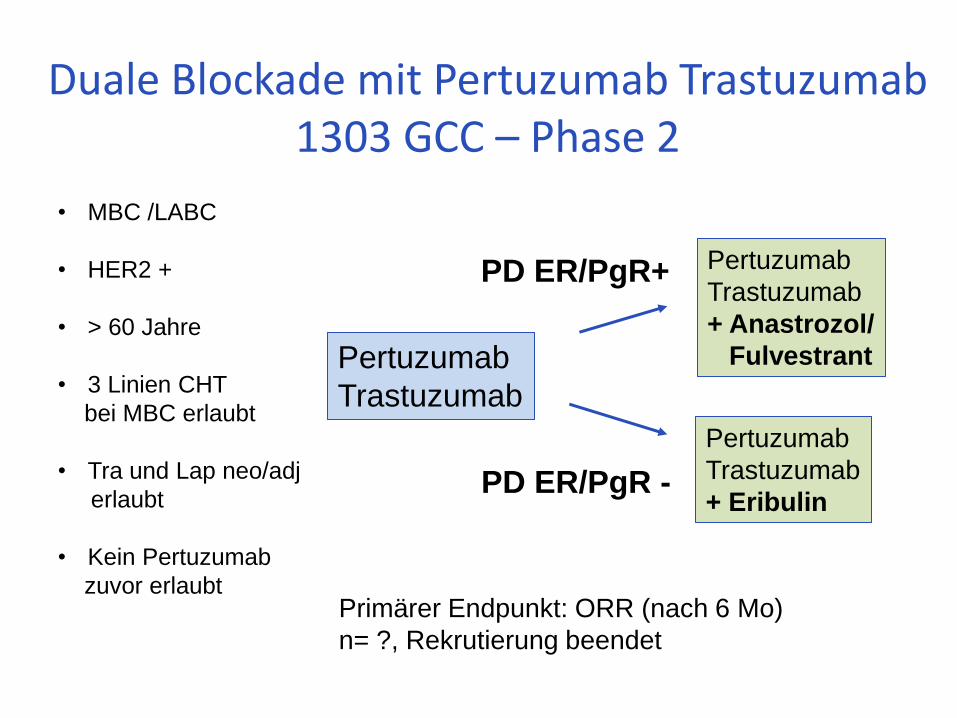
Duale Blockade mit Pertuzumab Trastuzumab 1303 GCC – Phase 2
Pertuzumab
Trastuzumab
• MBC /LABC
• HER2 +
• > 60 Jahre
• 3 Linien CHT
bei MBC erlaubt
• Tra und Lap neo/adj
erlaubt
• Kein Pertuzumab
zuvor erlaubt
PD ER/PgR+
Primärer Endpunkt: ORR (nach 6 Mo)
n= ?, Rekrutierung beendet
Pertuzumab
Trastuzumab
+ Anastrozol/
Fulvestrant
Pertuzumab
Trastuzumab
+ Eribulin PD ER/PgR -
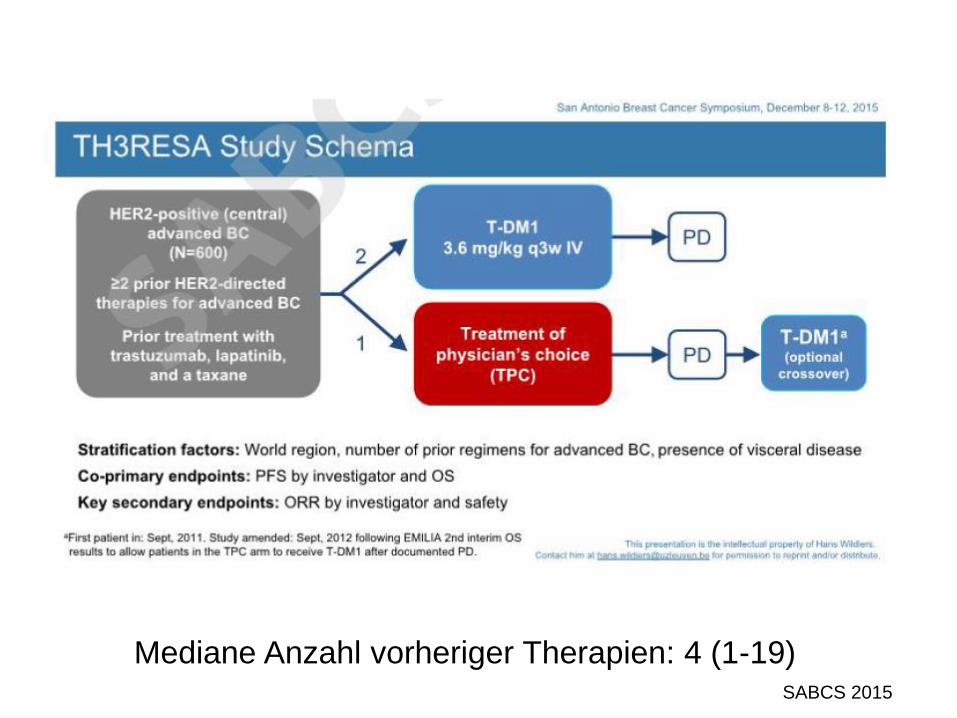
Mediane Anzahl vorheriger Therapien: 4 (1-19) SABCS 2015
*Hazard ratio adjusted for prognostic factors (p-values 1-sided by design at significance of 0.04)
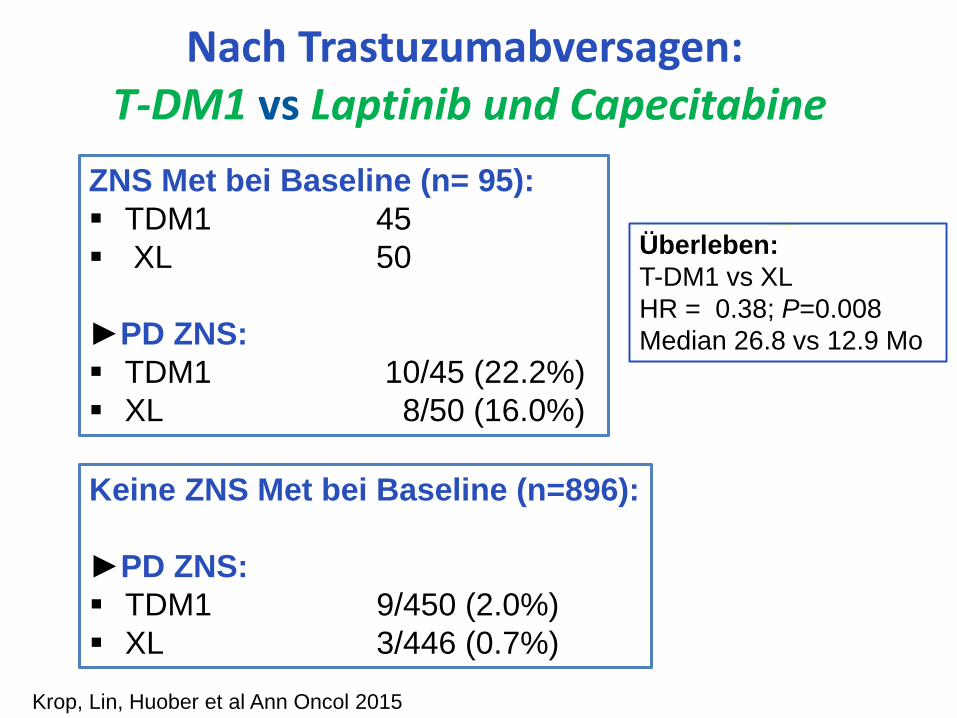
Nach Trastuzumabversagen: T-DM1 vs Laptinib und Capecitabine
ZNS Met bei Baseline (n= 95):
TDM1 45
XL 50
►PD ZNS:
TDM1 10/45 (22.2%)
XL 8/50 (16.0%)
Keine ZNS Met bei Baseline (n=896):
►PD ZNS:
TDM1 9/450 (2.0%)
XL 3/446 (0.7%)
Krop, Lin, Huober et al Ann Oncol 2015
Überleben:
T-DM1 vs XL
HR = 0.38; P=0.008
Median 26.8 vs 12.9 Mo
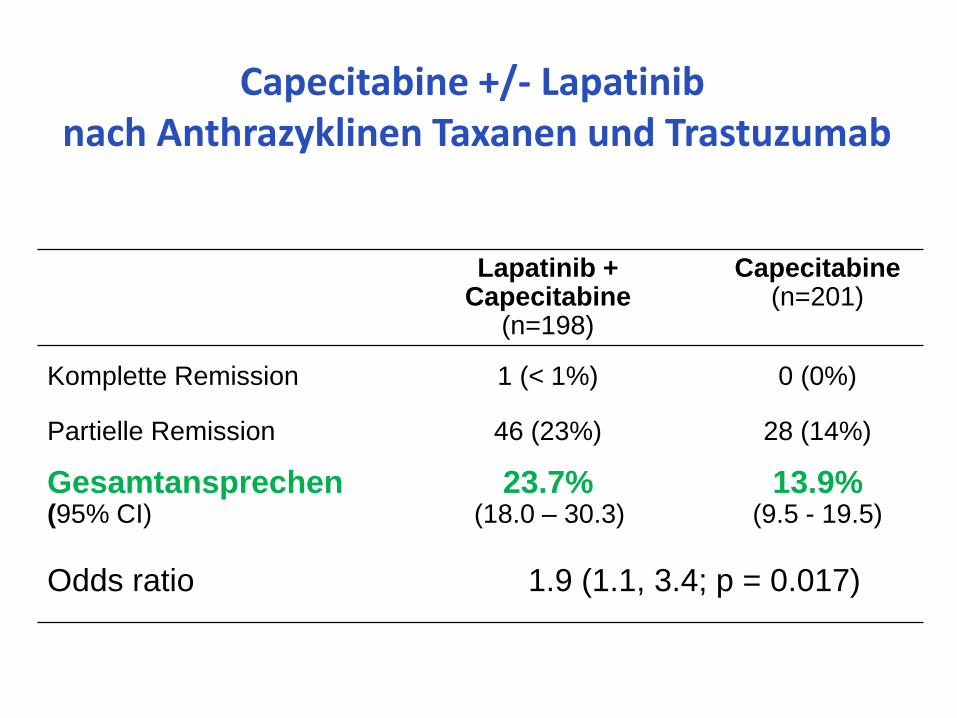
Lapatinib + Capecitabine
(n=198)
Capecitabine (n=201)
Komplette Remission 1 (< 1%) 0 (0%)
Partielle Remission 46 (23%) 28 (14%)
Gesamtansprechen (95% CI)
23.7% (18.0 – 30.3)
13.9% (9.5 - 19.5)
Odds ratio 1.9 (1.1, 3.4; p = 0.017)
Capecitabine +/- Lapatinib nach Anthrazyklinen Taxanen und Trastuzumab
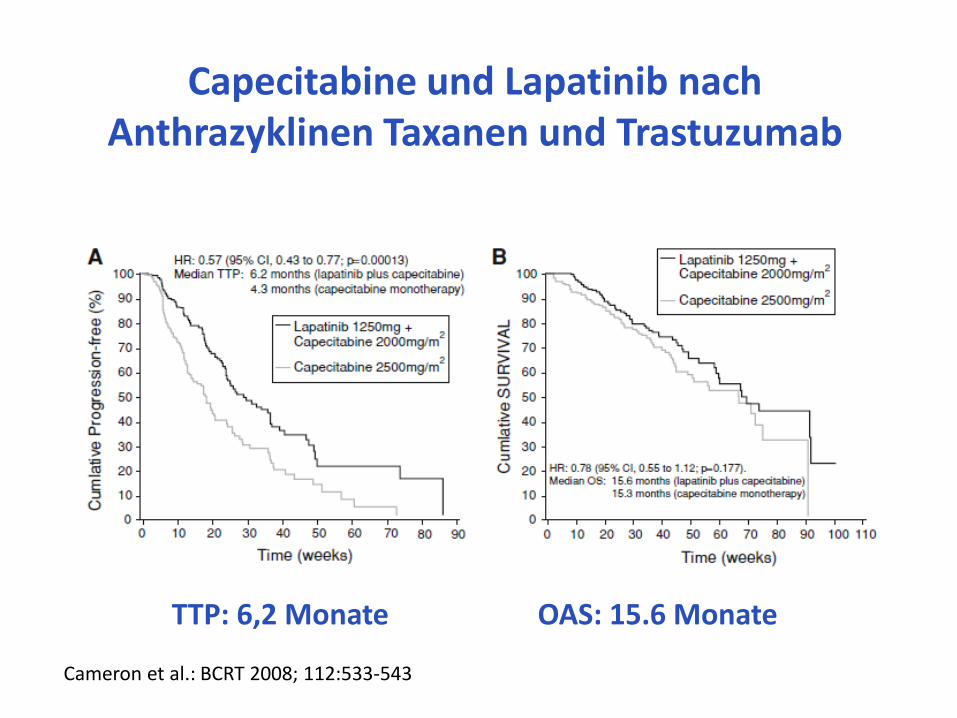
Capecitabine und Lapatinib nach Anthrazyklinen Taxanen und Trastuzumab
TTP: 6,2 Monate OAS: 15.6 Monate
Cameron et al.: BCRT 2008; 112:533-543












![Precision Medicine - 43. Deutscher Krankenhaustag€¦ · Progressionsfrei und Vemurafenib [Zelboraf ®] European Journal of Cancer 2017 Überleben in der metastasierten Situation](https://static.fdokument.com/doc/165x107/606235c6e19a5303fe2895ff/precision-medicine-43-deutscher-progressionsfrei-und-vemurafenib-zelboraf-.jpg)