
![Nekrotisierende Enterokolitis des Frühgeborenen und Cholestase · der NEC-Patienten Frühgeborene[21], und zudem wurde festgestellt, dass das Auftreten der Darmaffektion invers mit](https://static.fdokument.com/doc/165x107/5d55841488c993af098b937c/nekrotisierende-enterokolitis-des-fruehgeborenen-und-cholestase-der-nec-patienten.jpg)






Sprachen
Seiten
Rechtliche

PathophysiologieBilirubin, PorphyrienCholestase, Ikterus
Hepatitis, Karzinome
Privatdozent Dr. Ulrich TreichelZentrum für Innere Medizin
Klinik für Gastroenterologie und Hepatologie
Leber
Funktionen:
�Proteinsynthese
�Fett- und Zuckerstoffwechselregulation
�Metabolismus und Stoffelimination
Pathophysiologie: Cholestase
Begriffe• Cholestase = Gallestau
• Ikterus = klinisches Symptom
• Labormarker („Leberwerte“) der Cholestase = – gamma-GT
– Alkalische Phosphatase
– Bilirubin
Funktionsdiagnostik der Leber
Laborindikatoren der Funktion:
�Blutzucker / Cholesterin = Metabolismus
�Albumin / Gerinnungsfaktoren = Synthese
�Bilirubin / gamma-Globulin = Elimination
�Bilirubin = Exkretion
Bilirubin - Metabolismus
�Bilirubin = 90 % Hämoglobin, 250 mg/d
�Bilirubin = konjugiert/unkonjugiert
(= direkt/indirekt)
�Bilirubin = „enterohepatischer Kreislauf“
�Bilirubin = Albuminbindung
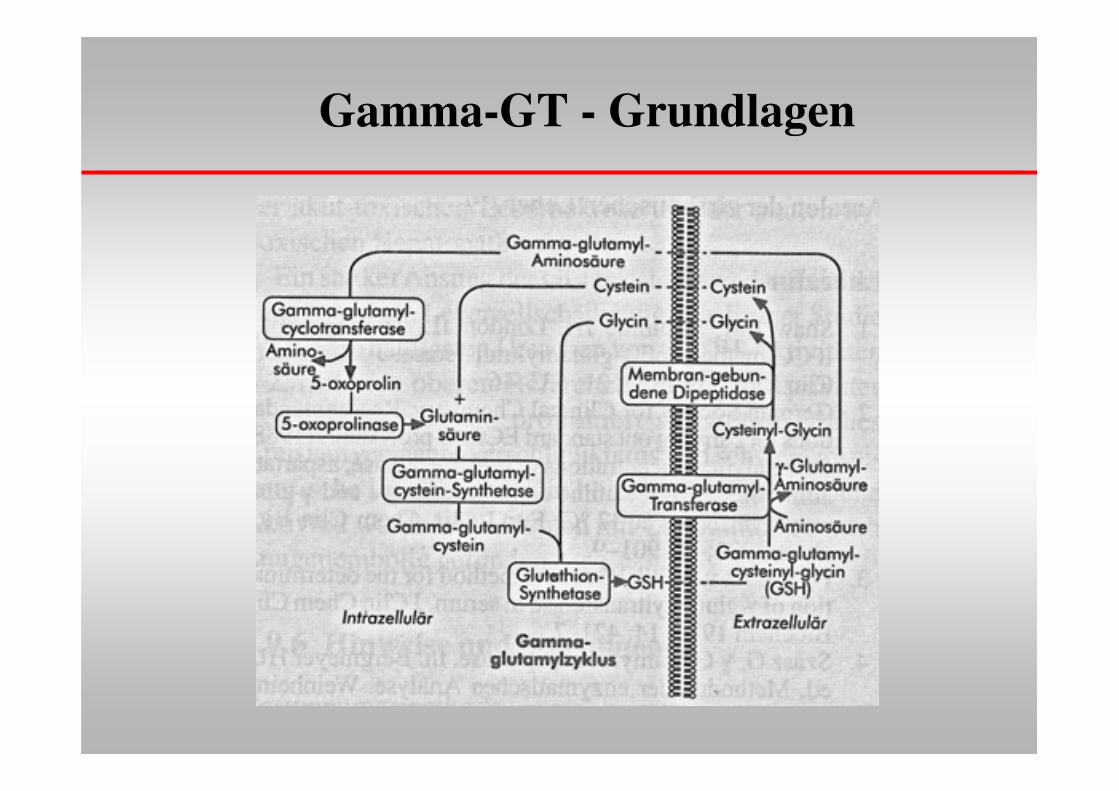
Gamma-GT - Grundlagen
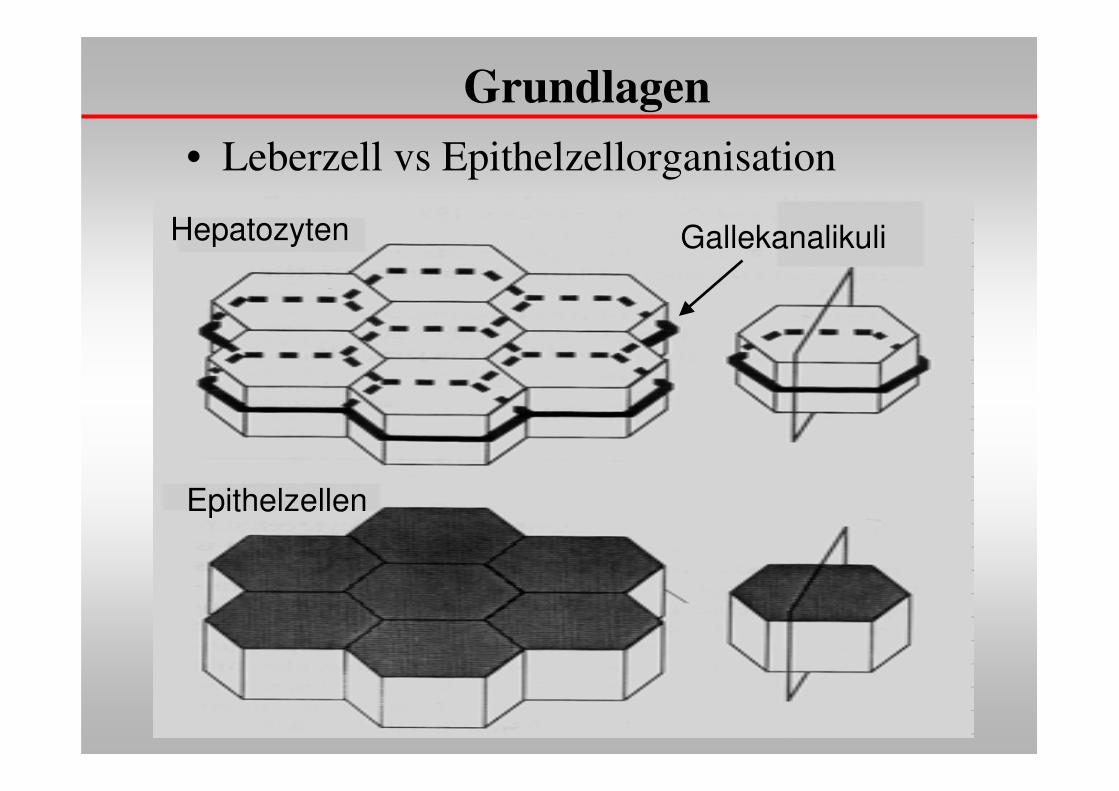
Grundlagen• Leberzell vs Epithelzellorganisation
Hepatozyten
Epithelzellen
Gallekanalikuli
Cholestase
�Ursachen
1. Fehlende Konjugation (Medikamente)
2. Fehlender Metabolismus (Zirrhose)
3. Abflußbehinderung (Gallensteine, Tumor)
Bilirubinerhöhung = Hyperbilirubinämie
�Prähepatisch• unkonjugiert
�Intrahepatisch• konjugiert
• unkonjugiert
�posthepatisch
Sichtbarer Ikterus ab ca 2,5 mg/dl Serum
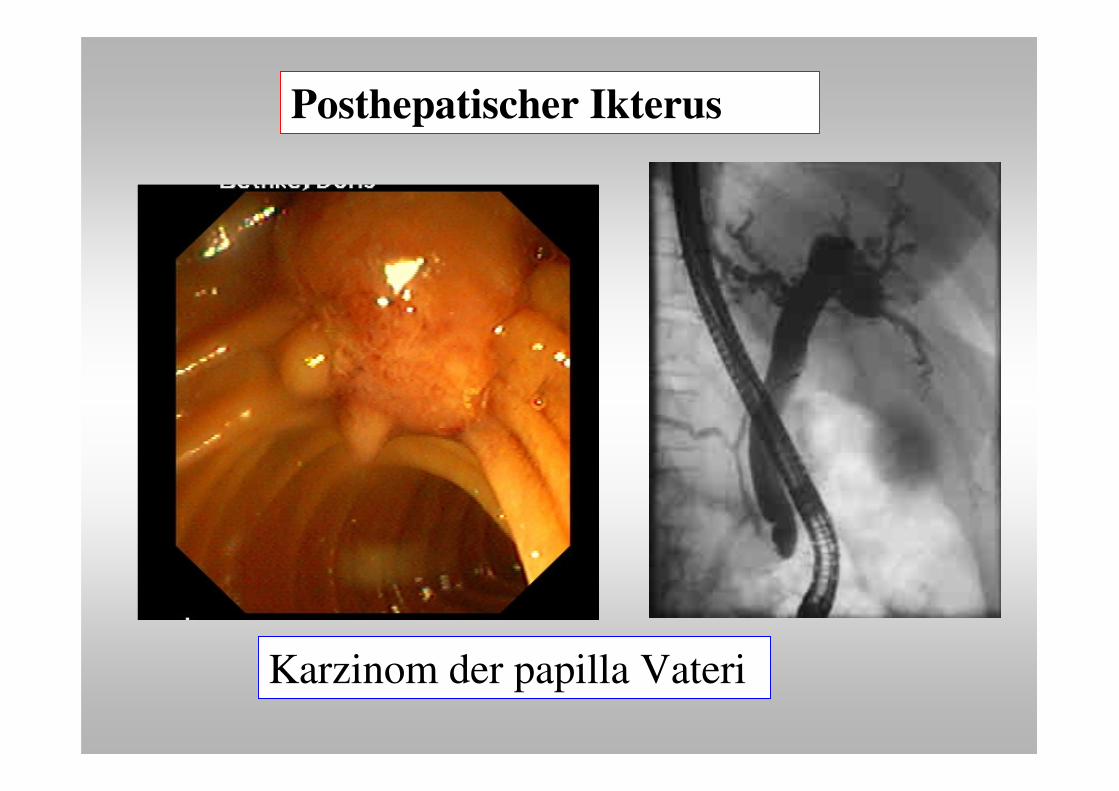
Karzinom der papilla Vateri
Posthepatischer Ikterus
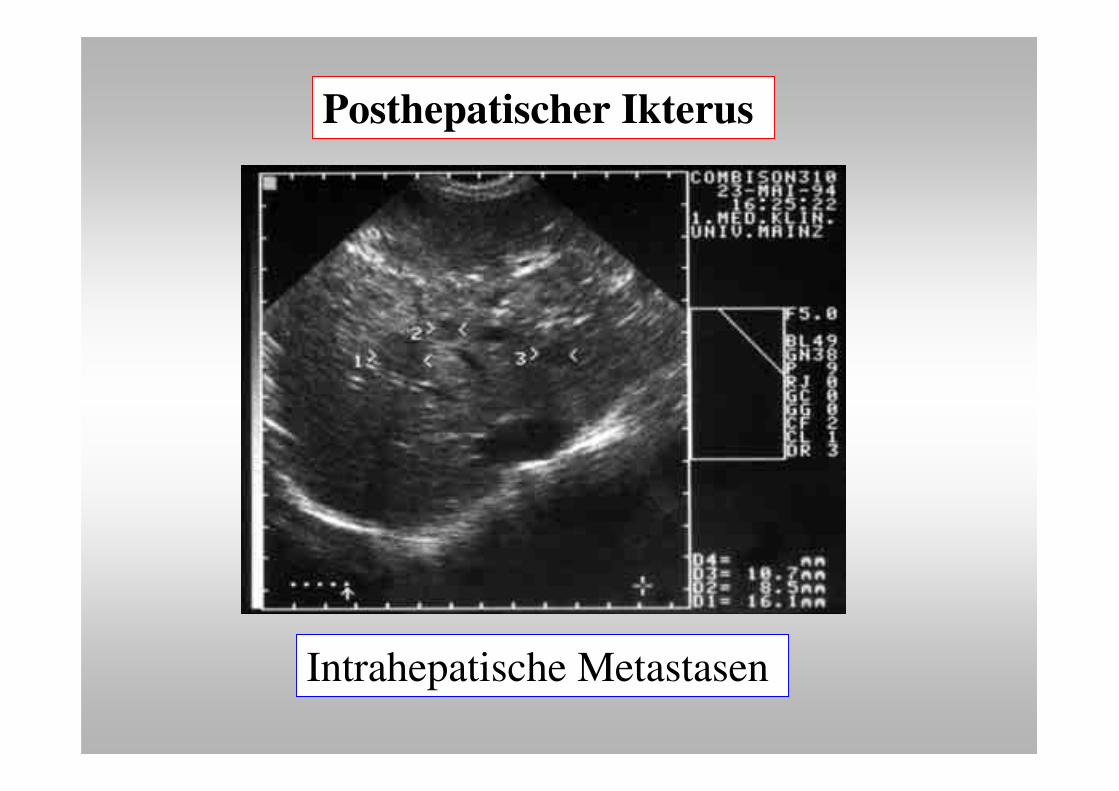
Intrahepatische Metastasen
Posthepatischer Ikterus
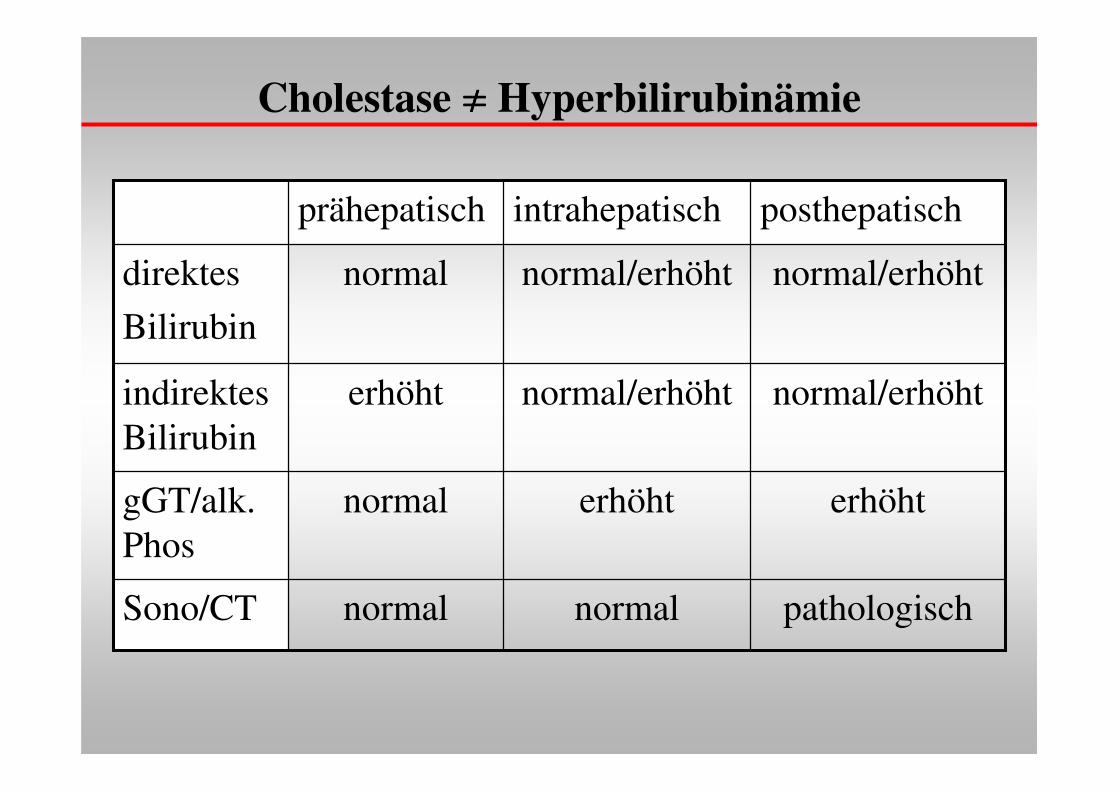
Cholestase ���� Hyperbilirubinämie
posthepatischintrahepatischprähepatisch
pathologischnormalnormalSono/CT
erhöhterhöhtnormalgGT/alk. Phos
normal/erhöhtnormal/erhöhterhöhtindirektes Bilirubin
normal/erhöhtnormal/erhöhtnormaldirektes
Bilirubin
Bilirubinerhöhung
�prähepatisch = Hämolyse
�intrahepatisch�konjugiert = Aufnahme (Meulengracht), Zirrhose
�unkonjugiert = genetisch (Crigler-Najjar), Medikamente
�posthepatisch = Abflußstörung
merke:
Cholestase (Bilirubin + gamma-GT) vs Gallenwegserweiterung
Erhöhte Gamma-GT Aktivität mit Bezug zur Leber
• Akute Hepatitis (Chronifizierung ?)
• Chronische Hepatitis (additive Faktoren/Zirrhose?)
• Alkoholhepatitis
• Zirrhose
• Fettleber
• Extrahepatische Cholestase (besser als AlkPhos !)
• intrahepatische Cholestase (Enzyminduktion)
• Lebermetastasen
• Vaskuläre Lebererkrankungen

Stoffwechsel, Porphyrien
• Stoffwechsel– Lipide
– Kohlenhydrate
– Eiweiß
– Porphyrine
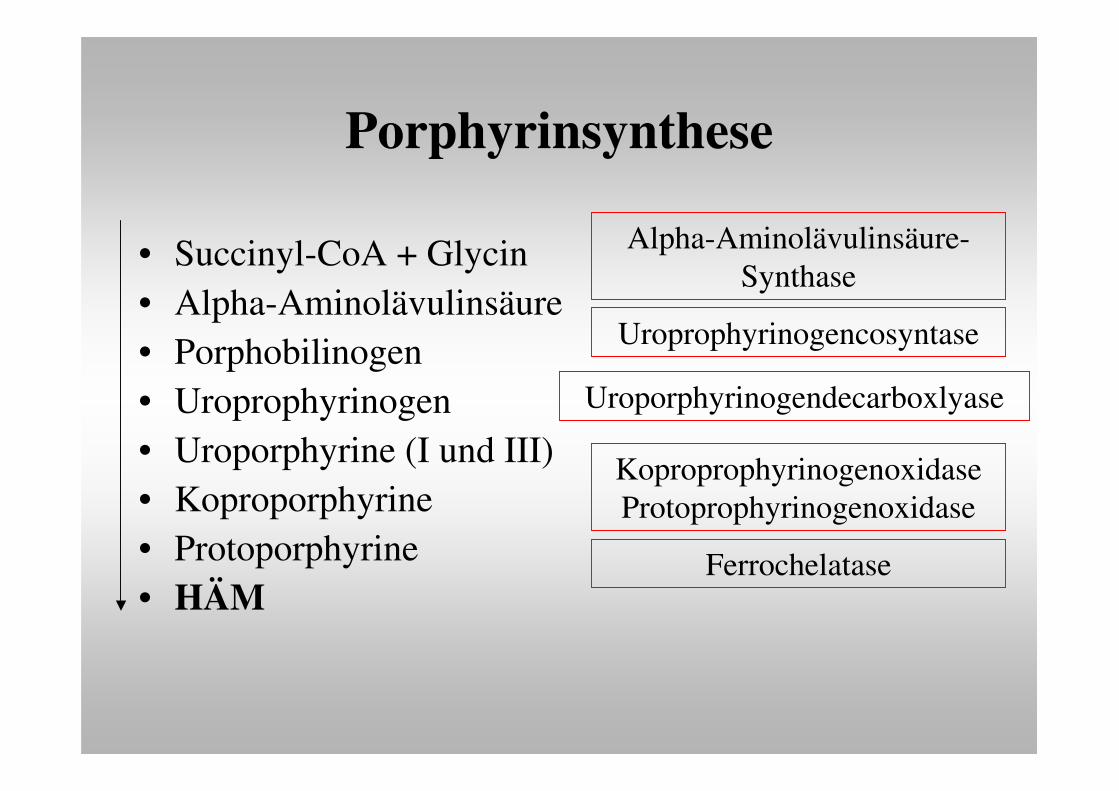
Porphyrinsynthese
• Succinyl-CoA + Glycin• Alpha-Aminolävulinsäure• Porphobilinogen• Uroprophyrinogen• Uroporphyrine (I und III)• Koproporphyrine• Protoporphyrine• HÄM
Alpha-Aminolävulinsäure-Synthase
Uroprophyrinogencosyntase
Uroporphyrinogendecarboxlyase
KoproprophyrinogenoxidaseProtoprophyrinogenoxidase
Ferrochelatase
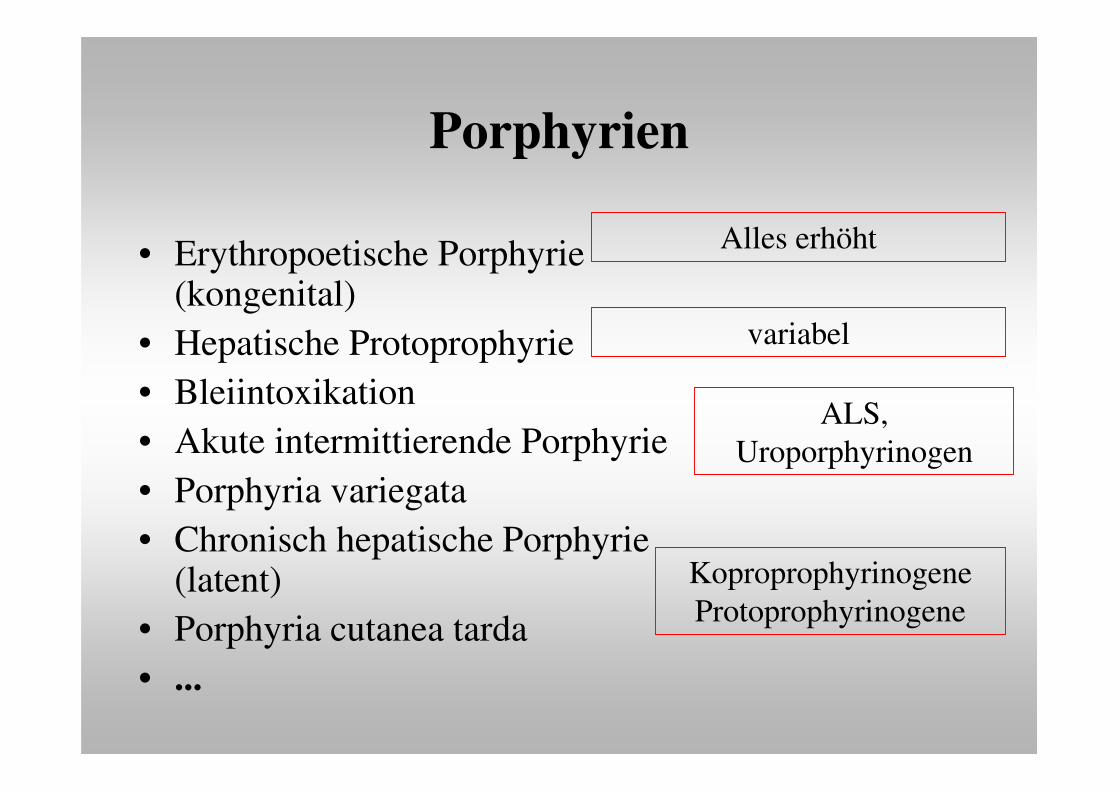
Porphyrien
• Erythropoetische Porphyrie(kongenital)
• Hepatische Protoprophyrie• Bleiintoxikation• Akute intermittierende Porphyrie• Porphyria variegata• Chronisch hepatische Porphyrie
(latent)• Porphyria cutanea tarda• ...
Alles erhöht
variabel
ALS, Uroporphyrinogen
KoproprophyrinogeneProtoprophyrinogene
Porphyrien = Störungen der Hämsynthese
• Erythropoetische Porphyrien(genetisch, auf die Erythrozyten bezogen)
• Hepatische Porporphyrien(erworben, auf die Leberzelle bezogen, p450 abhängig)
Porphyrien - Photodermatose
• Erythropoetische Porphyrien– Kongenitale erythropoetische Porphyrie– Erythropoetische Protoporphyrie
• Hepatische Porporphyrien– akute intermittierende Porphyrie– Porphyria variegata– Hereditäre Koproporphyrie– Prophyria cutanea tarda
ja
nein
ja
ja
ja
nein
Porphyrien - Diagnostik
• delta-Aminolävulinsäure
• Gesamt-Porphyrine
• Bestimmung im 24h- Urin (Stuhl)
PathophysiologieBilirubin, ProphyrienCholestase, Ikterus
Hepatitis, Karzinome
Privatdozent Dr. Ulrich TreichelZentrum für Innere Medizin
Klinik für Gastroenterologie und Hepatologie
����
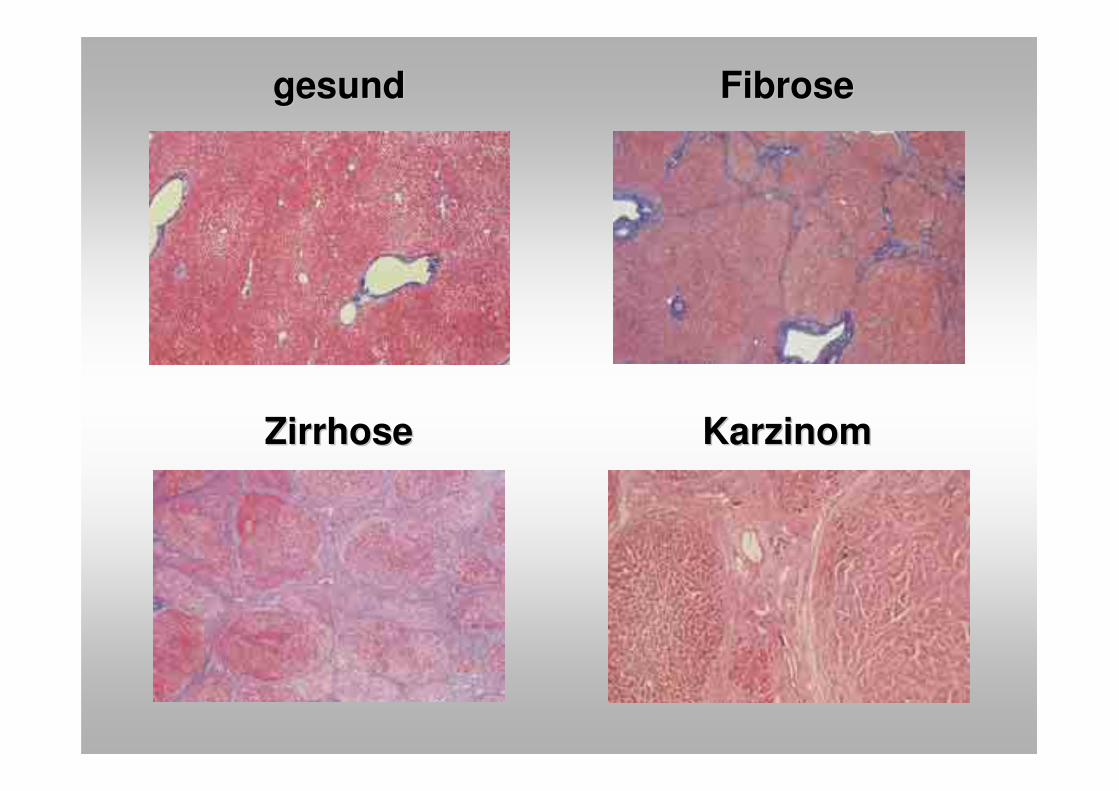
FibroseFibrose
ZirrhoseZirrhose KarzinomKarzinom
gesundgesund
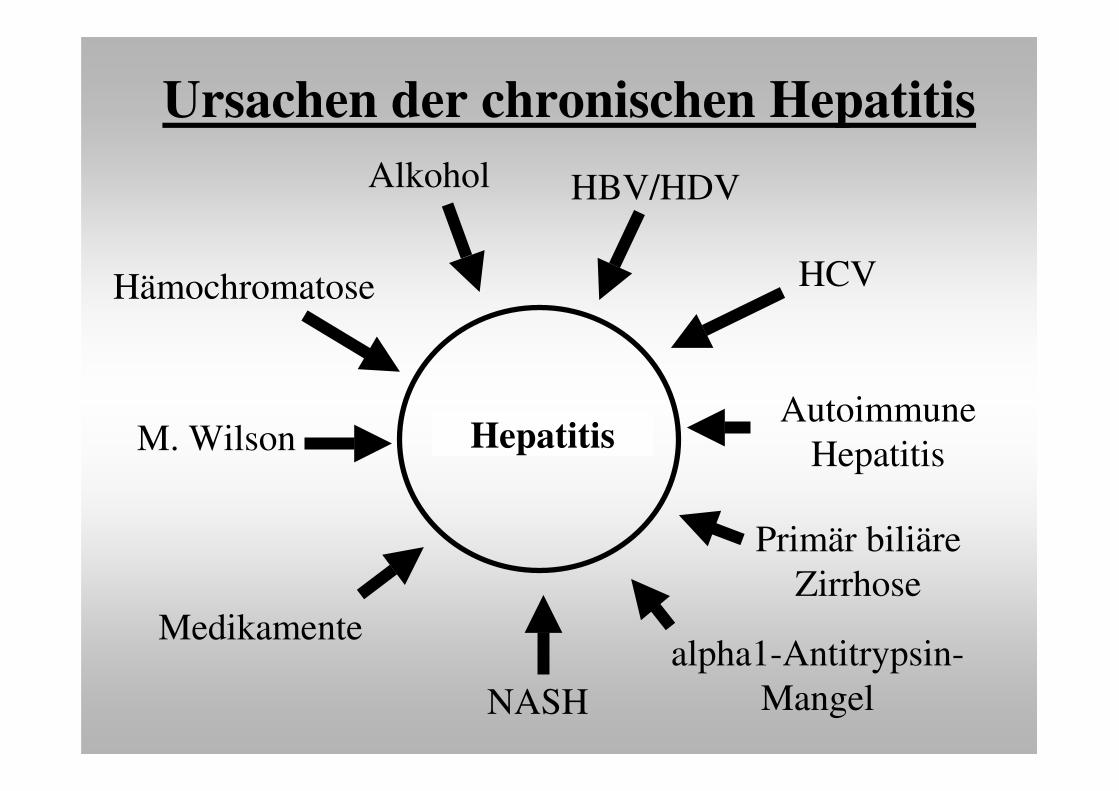
Hepatitis
HBV/HDV
alpha1-Antitrypsin-Mangel
AutoimmuneHepatitis
Medikamente
Alkohol
HCV
M. Wilson
NASH
Hämochromatose
Primär biliäreZirrhose
Ursachen der chronischen Hepatitis
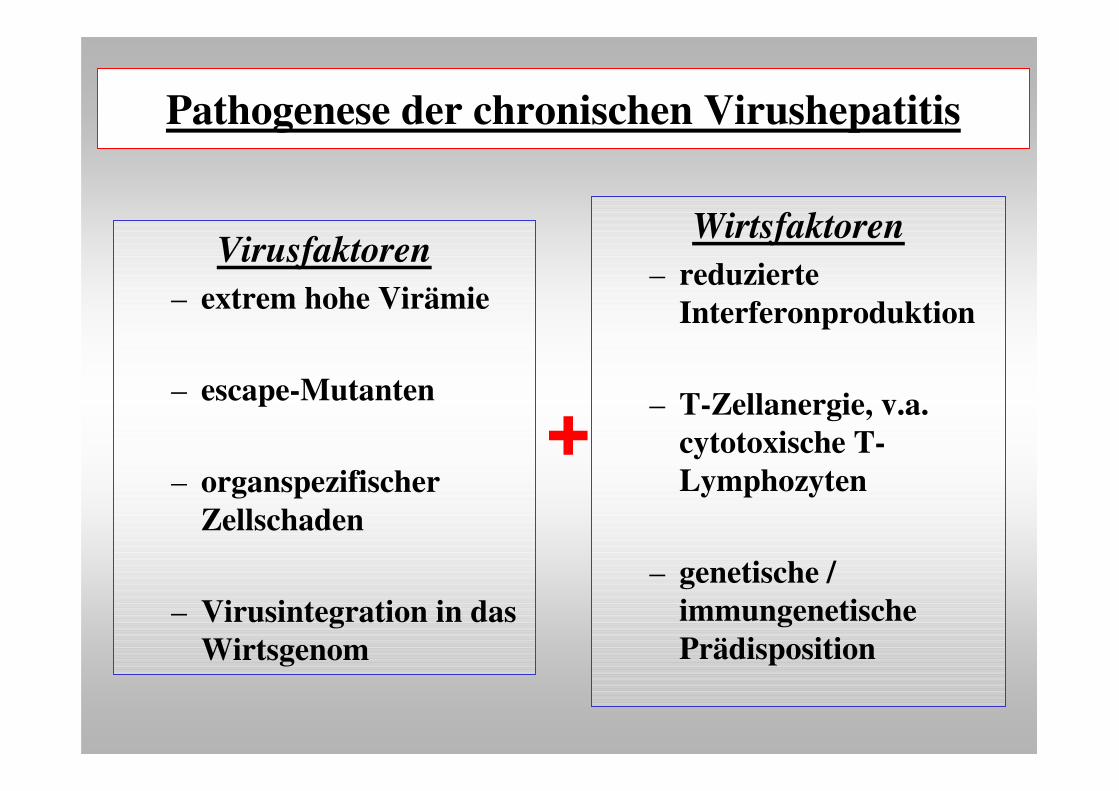
Pathogenese der chronischen Virushepatitis
Virusfaktoren– extrem hohe Virämie
– escape-Mutanten
– organspezifischer Zellschaden
– Virusintegration in das Wirtsgenom
Wirtsfaktoren– reduzierte
Interferonproduktion
– T-Zellanergie, v.a. cytotoxische T-Lymphozyten
– genetische / immungenetische Prädisposition
+
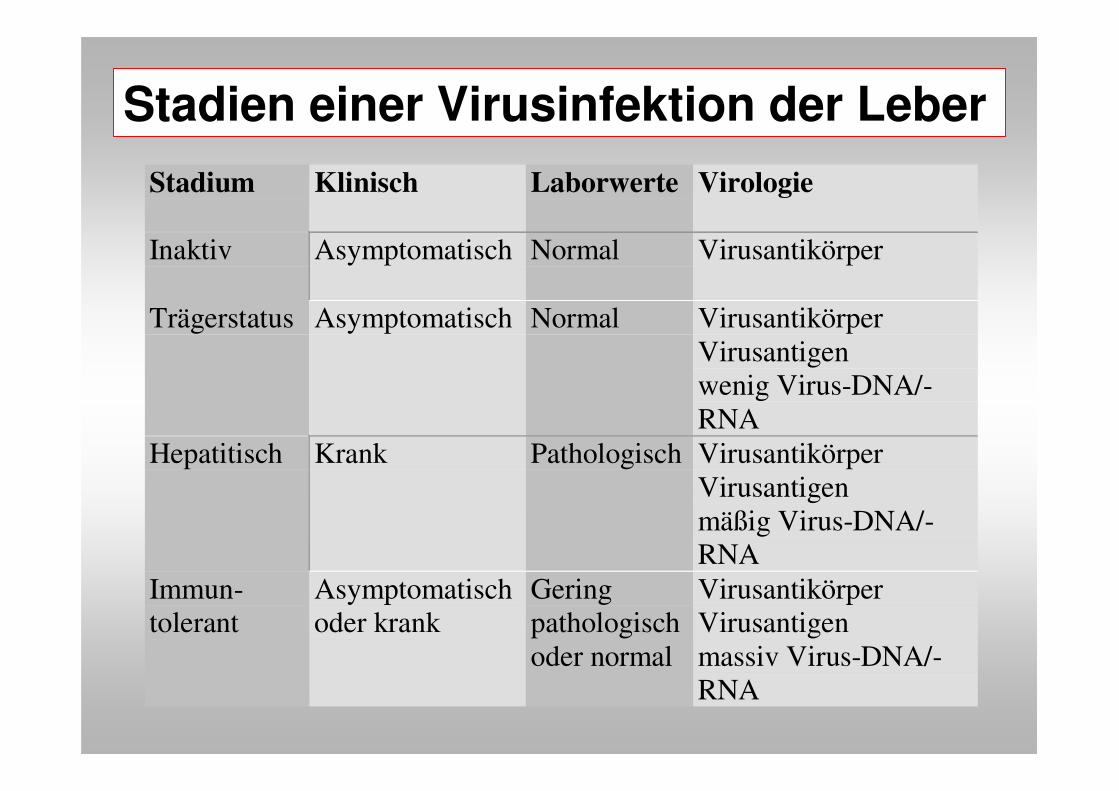
Stadium Klinisch Laborwerte Virologie
Inaktiv Asymptomatisch Normal Virusantikörper
Trägerstatus Asymptomatisch Normal VirusantikörperVirusantigenwenig Virus-DNA/-RNA
Hepatitisch Krank Pathologisch VirusantikörperVirusantigenmäßig Virus-DNA/-RNA
Immun-tolerant
Asymptomatischoder krank
Geringpathologischoder normal
VirusantikörperVirusantigenmassiv Virus-DNA/-RNA
Stadien einer Virusinfektion der Leber
Autoimmune Hepatitis und Begleiterkrankungen
• Überlappungssyndrome mit– primär biliäre Zirrhose
– primär sklerosierender Cholangitis
• Assoziationen mit anderen Autoimmunerkrankungen– Rheuma, LE, Sharp
– Endokrinopathien (Schilddrüse)
– Enteropathien (IBD, Sprue)
– etc.
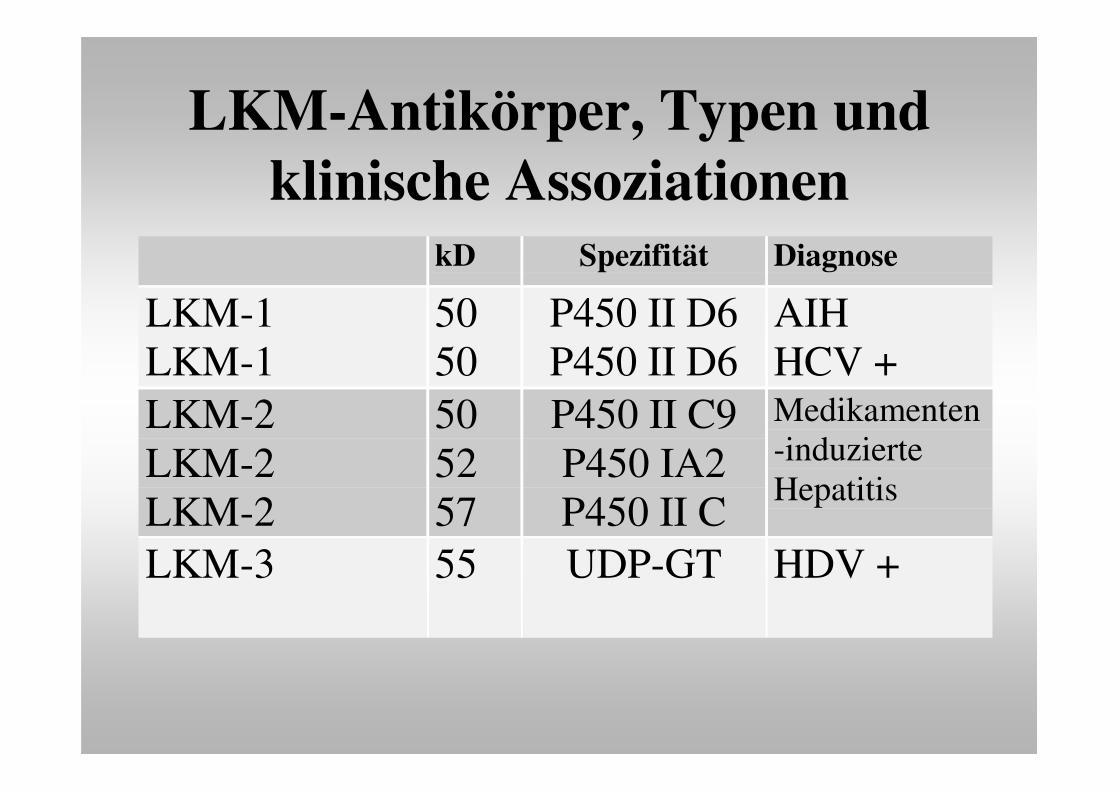
LKM-Antikörper, Typen und klinische Assoziationen
kD Spezifität Diagnose
LKM-1LKM-1
5050
P450 II D6P450 II D6
AIHHCV +
LKM-2LKM-2LKM-2
505257
P450 II C9P450 IA2P450 II C
Medikamenten-induzierteHepatitis
LKM-3 55 UDP-GT HDV +
AutoimmunkrankheitenLektionen von Phänomenen
• Autoantikörper = Autoantigene• Genetik = Immungenetik• Zellbiologie = zelluläre Mechanismen• Tiermodelle = z.B. Zytokininteraktionen
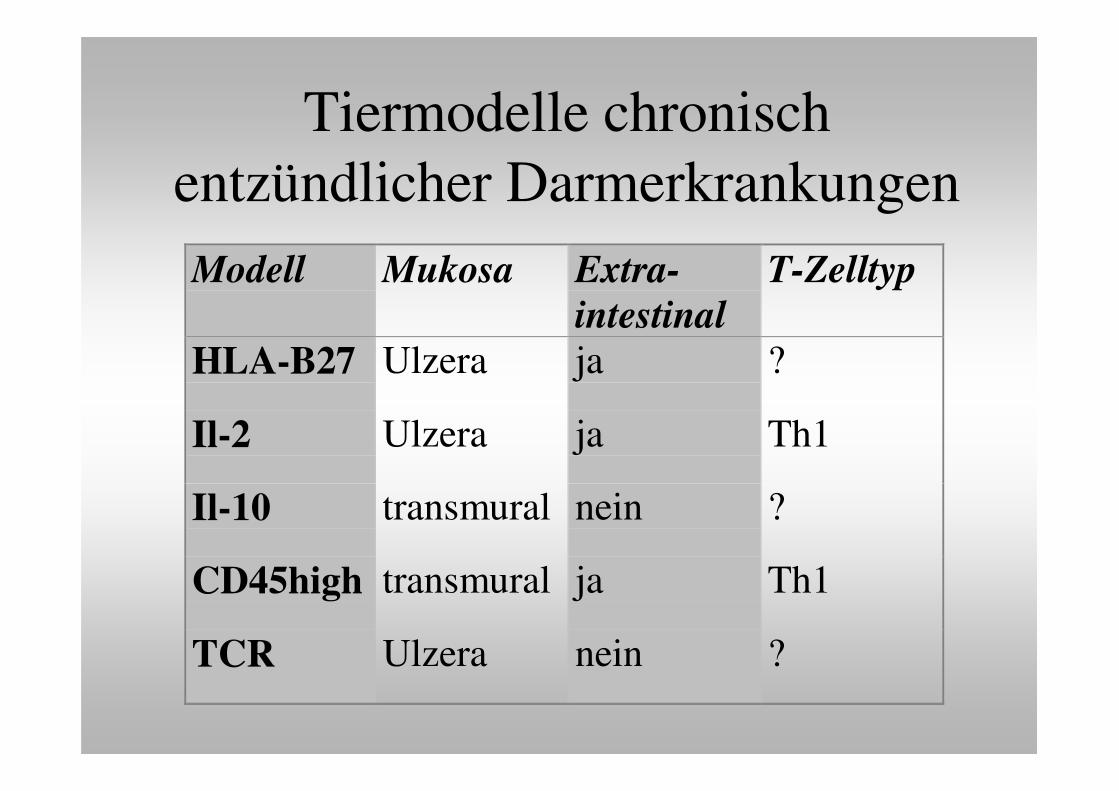
Tiermodelle chronisch entzündlicher DarmerkrankungenModell Mukosa Extra-
intestinalT-Zelltyp
HLA-B27 Ulzera ja ?
Il-2 Ulzera ja Th1
Il-10 transmural nein ?
CD45high transmural ja Th1
TCR Ulzera nein ?
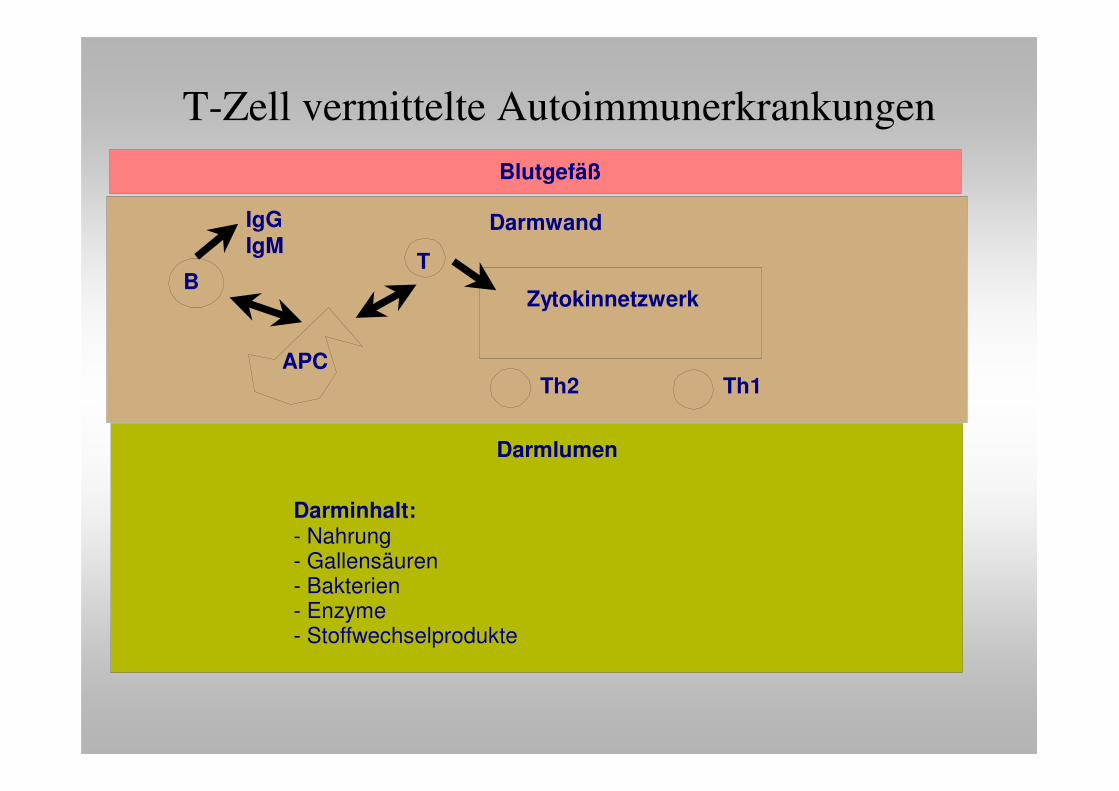
T-Zell vermittelte AutoimmunerkrankungenBlutgefäß
Darmwand
Darmlumen
B
APC
IgGIgM
T
Darminhalt:- Nahrung- Gallensäuren- Bakterien- Enzyme- Stoffwechselprodukte
Zytokinnetzwerk
Th2 Th1
AutoimmunkrankheitenLektionen von Phänomenen
• Empirische Therapie– Immunsuppressiva
• spezifische Therapie – anti-Zytokin Antikörper
Nicht-alkoholische Steatohepatitis
• möglicherweise häufiger als derzeit diagnostiziert
• Progression zur Leberzirrhose !
• Pathogenese:– Genetik (Insulinresistenz, HFE-Gen ?)
– mikrosomale Aktivität: p-450 Defizienz, 520 bp-Deletion ?
– bakterielle Fehlbesiedlung des Darmes ?
– TNF-alpha durch Endotoxikämie?
– multiple, additive Faktoren ?
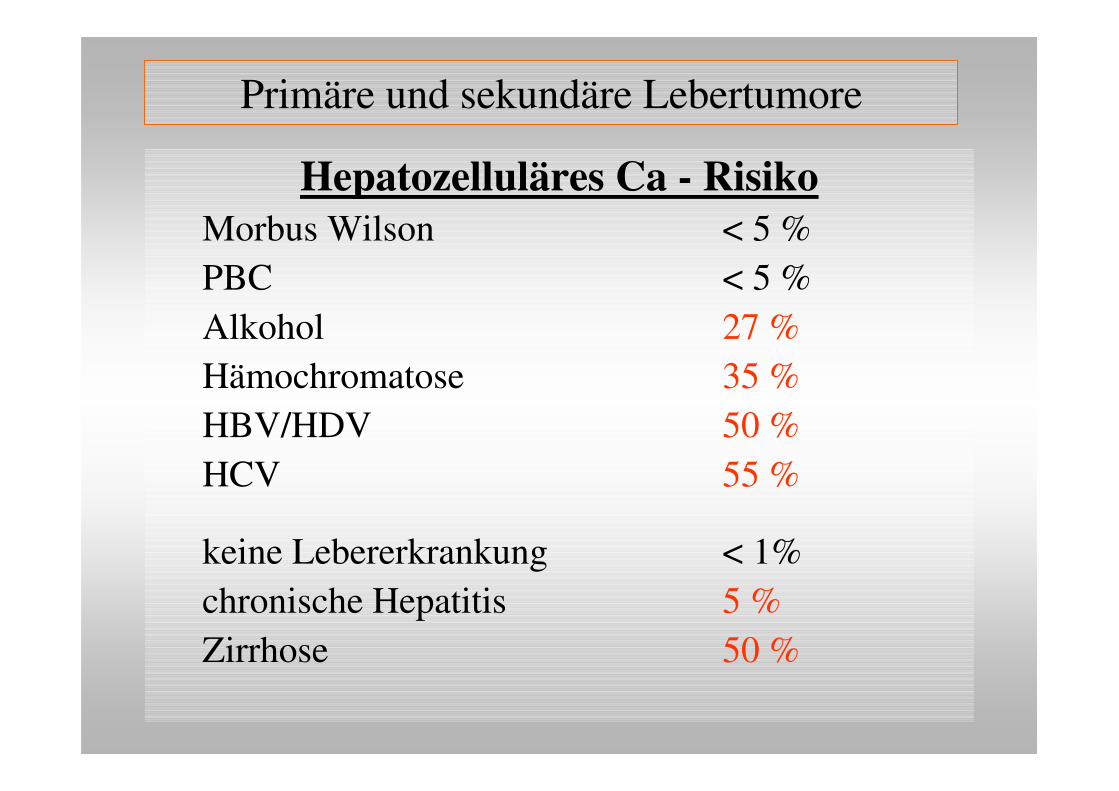
Primäre und sekundäre Lebertumore
Hepatozelluläres Ca - RisikoMorbus Wilson < 5 %PBC < 5 %Alkohol 27 %Hämochromatose 35 %HBV/HDV 50 %HCV 55 %
keine Lebererkrankung < 1%chronische Hepatitis 5 %Zirrhose 50 %
Hepatozelluläres CaChronische Lebererkrankung
Risikofaktoren:Nekrose, Entzündung, Regeneration, Mitose, DNA-repairKofaktoren:Alkohol, Aflatoxine, AndrogeneVirusinfektion:Replikation, GenexpressionGenetik:Onkogene, Tumorsuppressorgene,
Mutationsreparaturgene
Rationelle allgemeine und spezielle Labordiagnostik
• Tumormarker:AFP (alpha1-Fetoprotein)
• im Serum (plus 1/2-jährliche US-Untersuchung) bei Risikopatienten
• reduziert HCC-Morbidität um 80 %• Ohne Tumornachweis bei akutem Leberversagen erhöht
Ca19/9• Marker des cholangiozellulären Karzinoms• ohne Tumornachweis bei Cholestase erhöht
Top Related