Akutes Leberversagen 20.5 - Praxis für Magen-Darm-Leber ... · Symptom-Beginn (Ikterus) 8 Wochen...
34
Akutes Leberversagen
Transcript of Akutes Leberversagen 20.5 - Praxis für Magen-Darm-Leber ... · Symptom-Beginn (Ikterus) 8 Wochen...
Akutes Leberversagen
Definition
Klinisches Syndrom mit folgenden Charakteristika:
• Rasche hepatozelluläre Dysfunktion (Koagulopathie, Ikterus)
• Enzephalopathie• Keine Leber-Vorerkrankung bekannt
1 Lee W.M., N Engl J Med 1993;329:1862-72
Akutes Leberversagen1
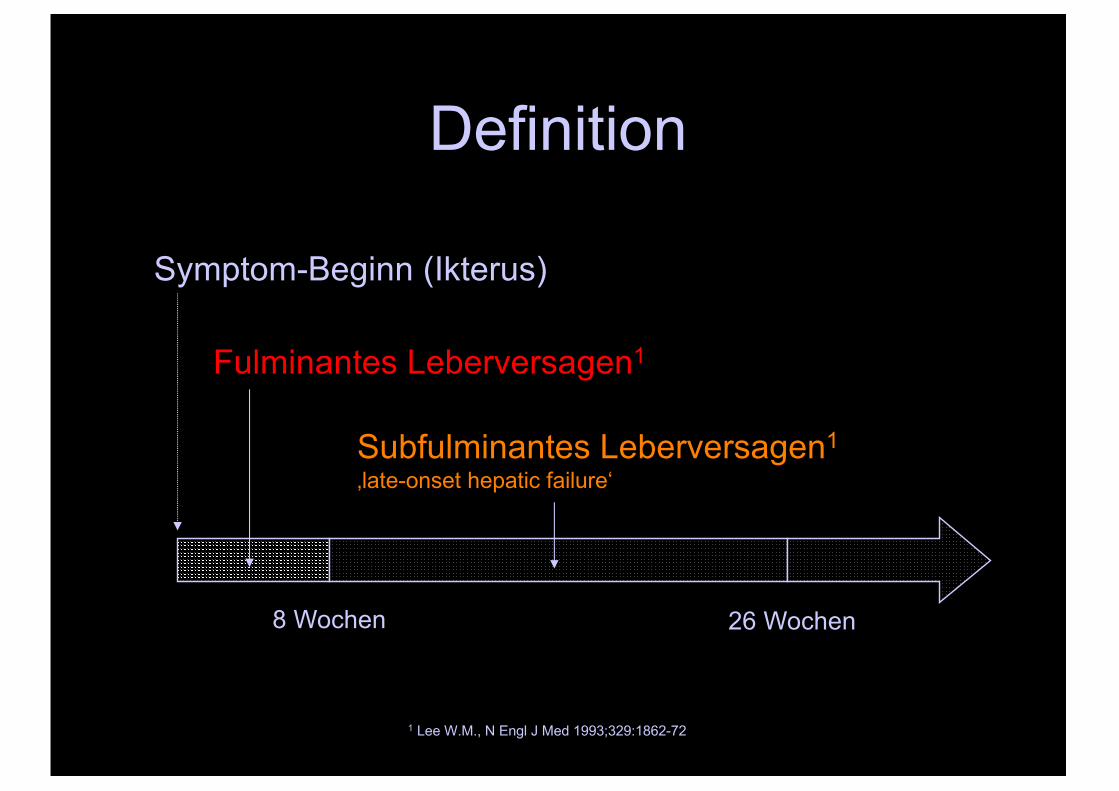
Definition
Symptom-Beginn (Ikterus)
8 Wochen 26 Wochen
Fulminantes Leberversagen1
Subfulminantes Leberversagen1
‚late-onset hepatic failure‘
1 Lee W.M., N Engl J Med 1993;329:1862-72
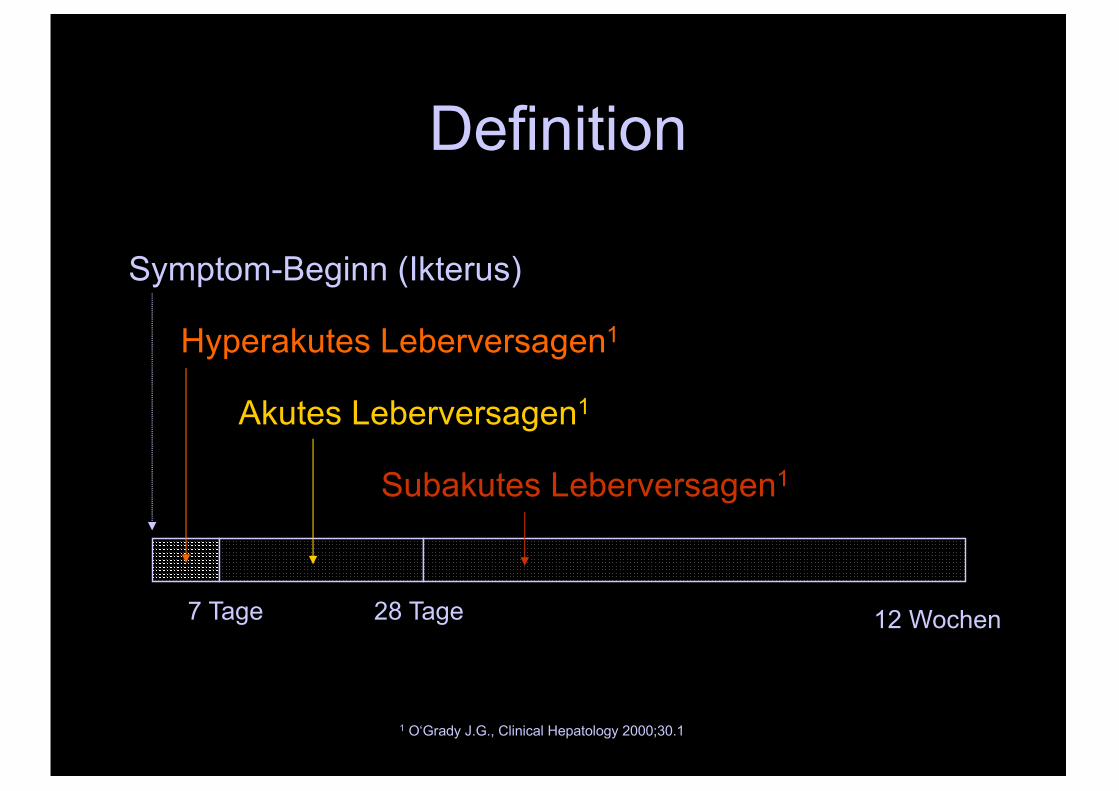
Definition
Symptom-Beginn (Ikterus)
7 Tage 28 Tage
Hyperakutes Leberversagen1
1 O‘Grady J.G., Clinical Hepatology 2000;30.1
12 Wochen
Akutes Leberversagen1
Subakutes Leberversagen1
Definition
1 O‘Grady J.G., Clinical Hepatology 2000;30.1
0
20
40
60
80
100
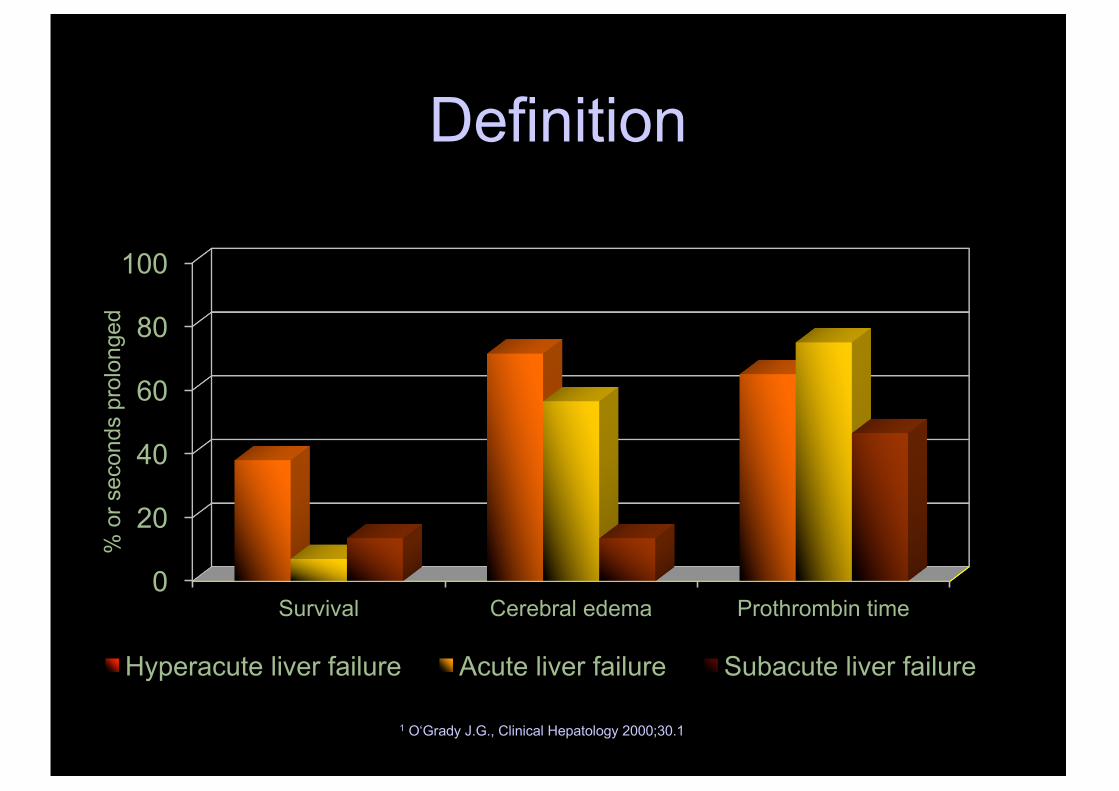
Survival Cerebral edema Prothrombin time
% o
r sec
onds
pro
long
ed
Categories of acute liver failure1
Hyperacute liver failure Acute liver failure Subacute liver failure
Aetiologie
• Virale Hepatitis
• Medikamente
• Toxine
• Vaskulär
• Varia
Aetiologie
• Virale Hepatitis
• Medikamente
• Toxine
• Vaskulär
• Varia
• Hepatitis B>D>A>E• Herpes, Varizellen,
EBV, CMV• Seronegative
Hepatitis
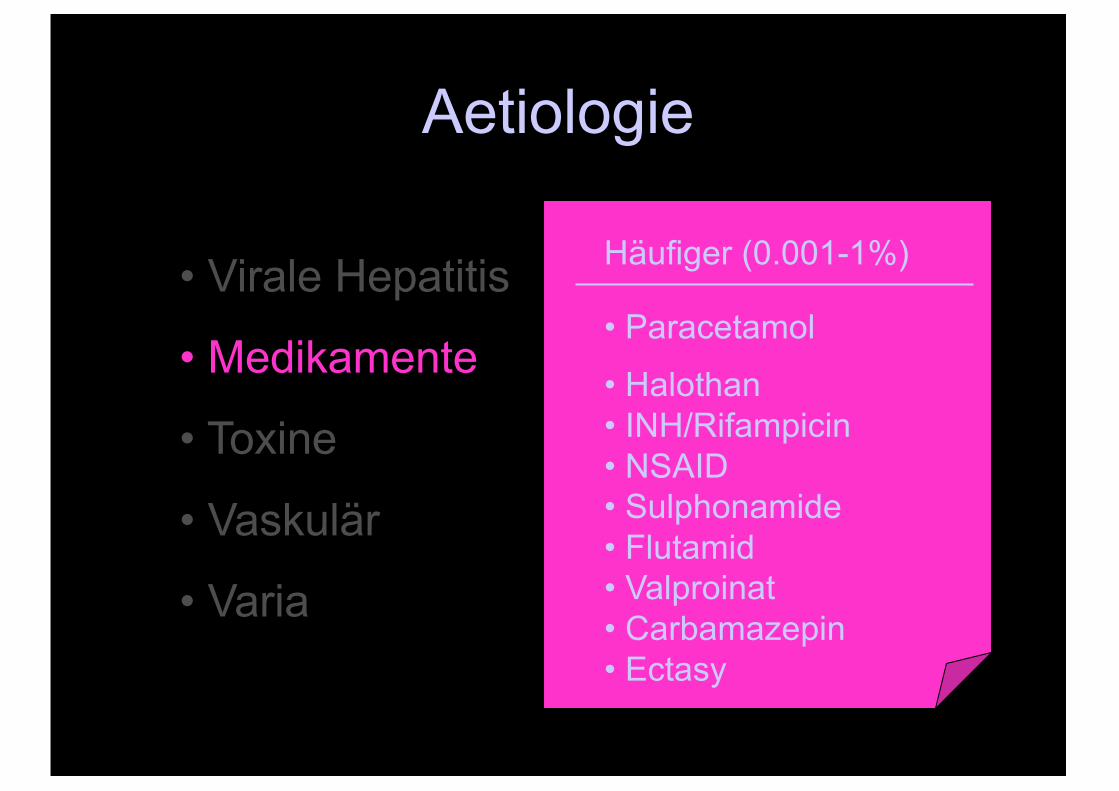
Aetiologie
• Virale Hepatitis
• Medikamente
• Toxine
• Vaskulär
• Varia
Häufiger (0.001-1%)
• Paracetamol
• Halothan• INH/Rifampicin• NSAID• Sulphonamide• Flutamid• Valproinat• Carbamazepin• Ectasy
Aetiologie
• Virale Hepatitis
• Medikamente
• Toxine
• Vaskulär
• Varia
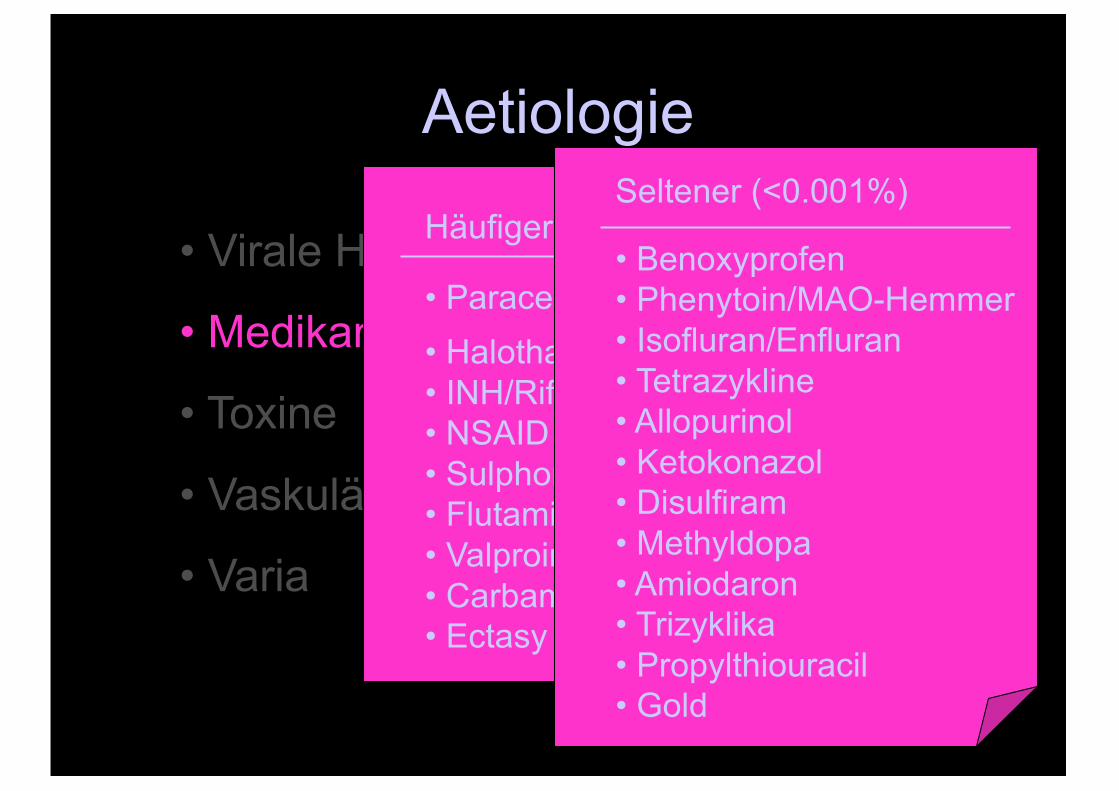
Häufiger (0.001-1%)
• Paracetamol• Halothan• INH/Rifampicin• NSAID• Sulphonamide• Flutamid• Valproinat• Carbamazepin• Ectasy
Seltener (<0.001%)
• Benoxyprofen• Phenytoin/MAO-Hemmer• Isofluran/Enfluran• Tetrazykline• Allopurinol• Ketokonazol• Disulfiram• Methyldopa• Amiodaron• Trizyklika• Propylthiouracil• Gold
Aetiologie
• Virale Hepatitis
• Medikamente
• Toxine
• Vaskulär
• Varia
• Ischämie• Budd-Chiari-Syndrom• Hitzschlag• Maligne Infiltration (Lymphome u.a.)
• Sepsis
Aetiologie
• Virale Hepatitis
• Medikamente
• Toxine
• Vaskulär
• Varia
• M. Wilson• Akute Schwangerschafts-
Fettleber• HELLP-Syndrom• Autoimmune Hepatitis• Reye-Syndrom
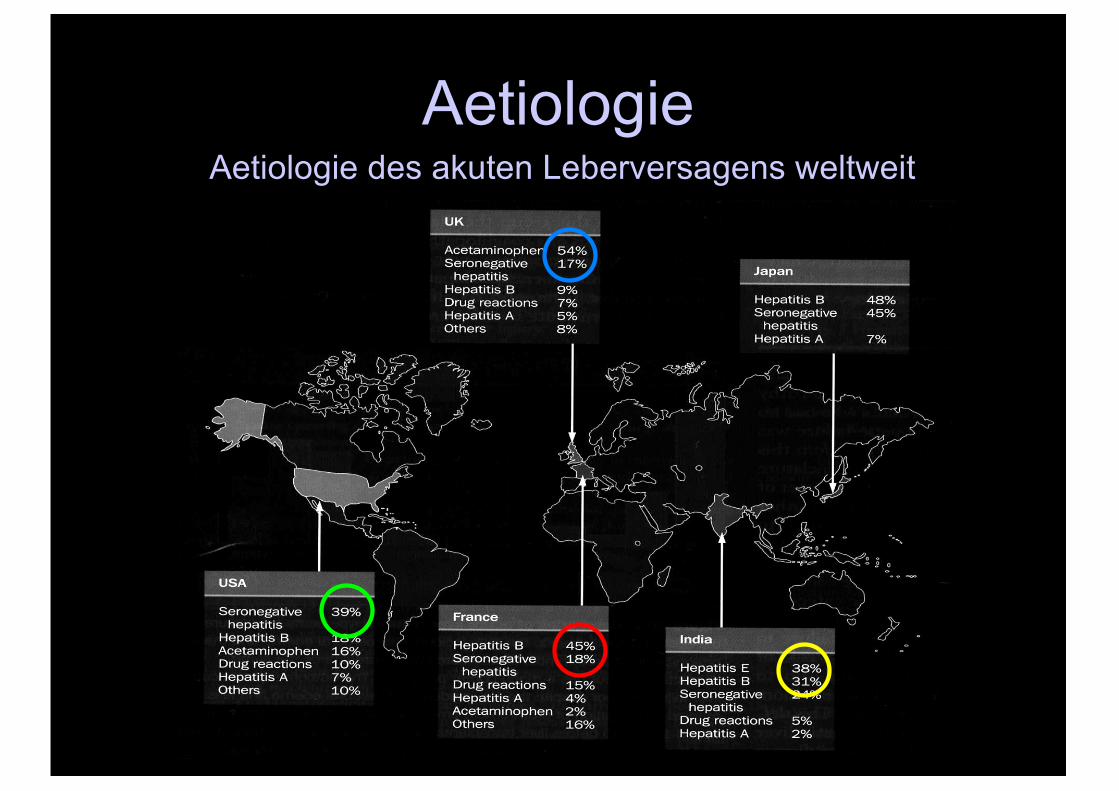
AetiologieAetiologie des akuten Leberversagens weltweit
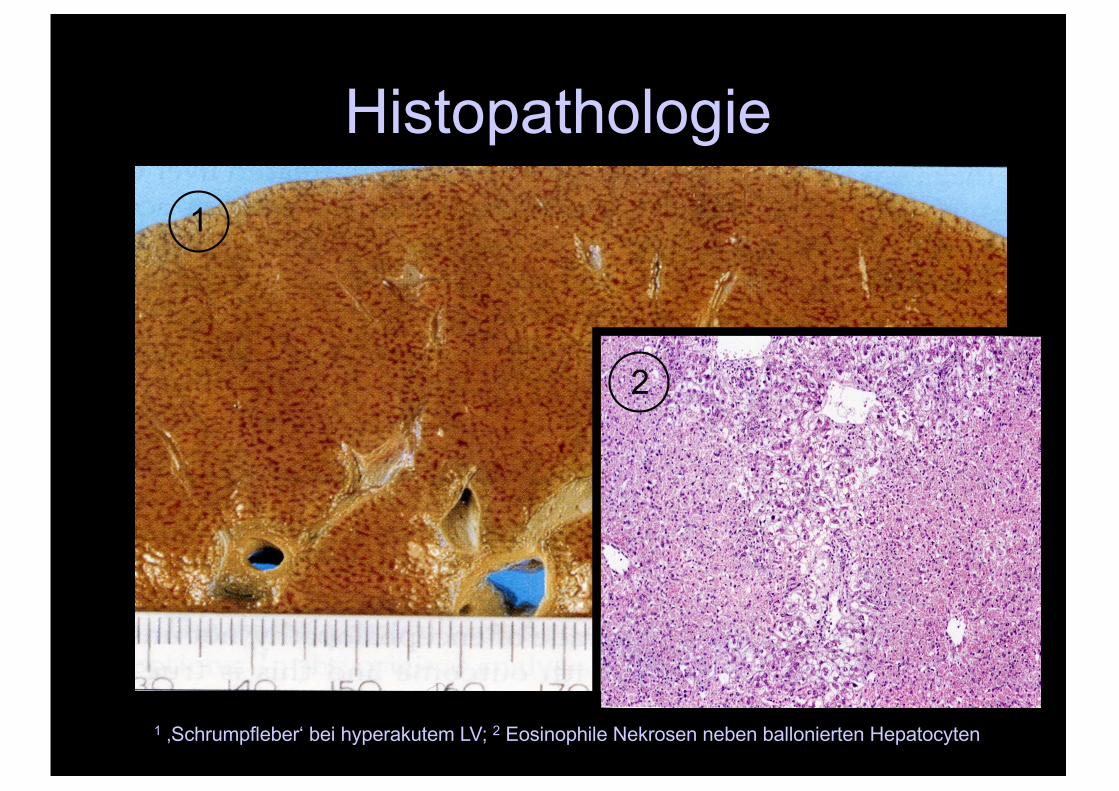
Histopathologie
1 ‚Schrumpfleber‘ bei hyperakutem LV; 2 Eosinophile Nekrosen neben ballonierten Hepatocyten
1
2
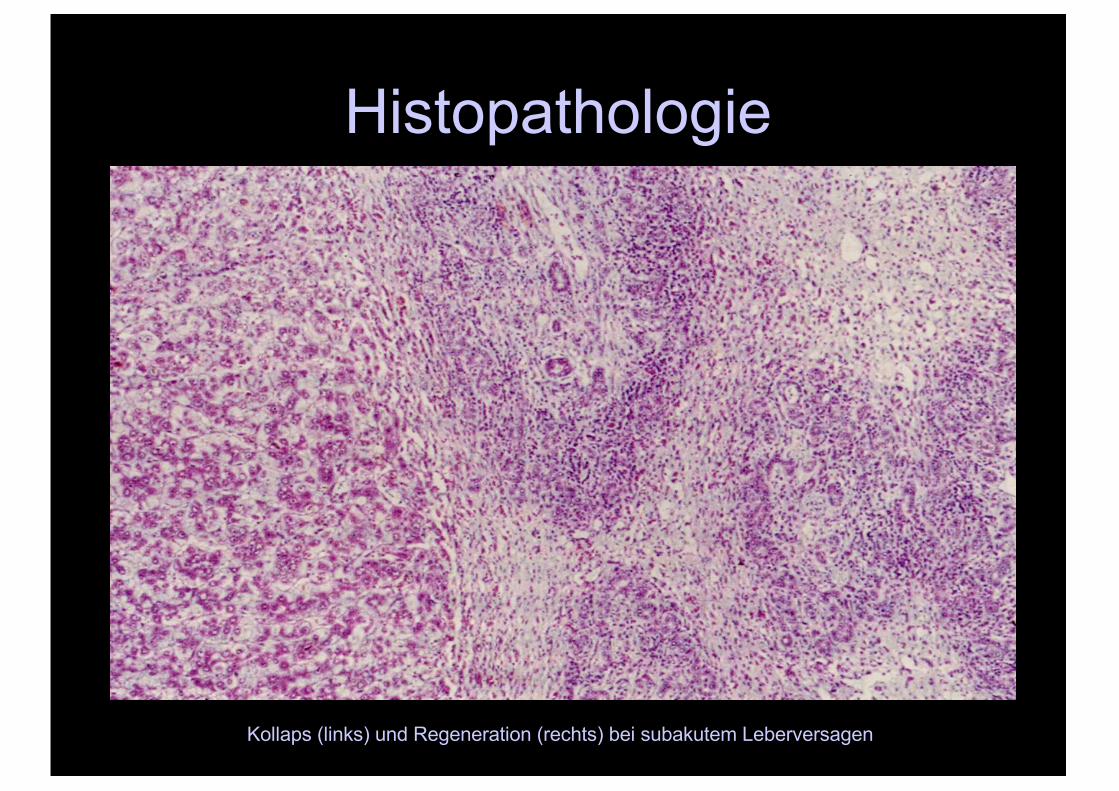
Histopathologie
Kollaps (links) und Regeneration (rechts) bei subakutem Leberversagen
Histopathologie
„Liver histology does not predict outcome“1
1 Hanau et al., Hepatology 1995;21: 345
SymptomatikI. Unspezifische Prodromal-Symptome
(Malaise, Nausea)
II. Symptom-Trias (2-10 Tage)• Ikterus• Bewusstseinsstörung (Enzephalopathie)• Plasmatische GerinnungsstörungTransaminasen-ErhöhungRespiratorische Alkalose
III.Multisystem-Versagen
SymptomatikEnzephalopathie• Zeitpunkt:
Häufig abrupt, gelegentlich vor Ikterus (Transporte!)
• Pathophysiologische Hypothesen:• Funktionsstörung
- Portosystemischer Shunt (‚Leberausfall-Koma)• Verminderte hepatische Detoxifikation• Enterotoxine• Ammonium-Hypothese
- Systemische Intoxikation durch hepatische Nekrose bzw. Apoptose (‚Leberzerfalls-Koma‘)
- Toxische Störung der Blut-Hirnschranke - Falsche Neurotransmitter (Benzodiazepin-like substances)
• Hirnödem (Hyperakutes LV: 70% , subakutes LV: 15%) - Vasogenes Oedem - Cytoxisches Oedem
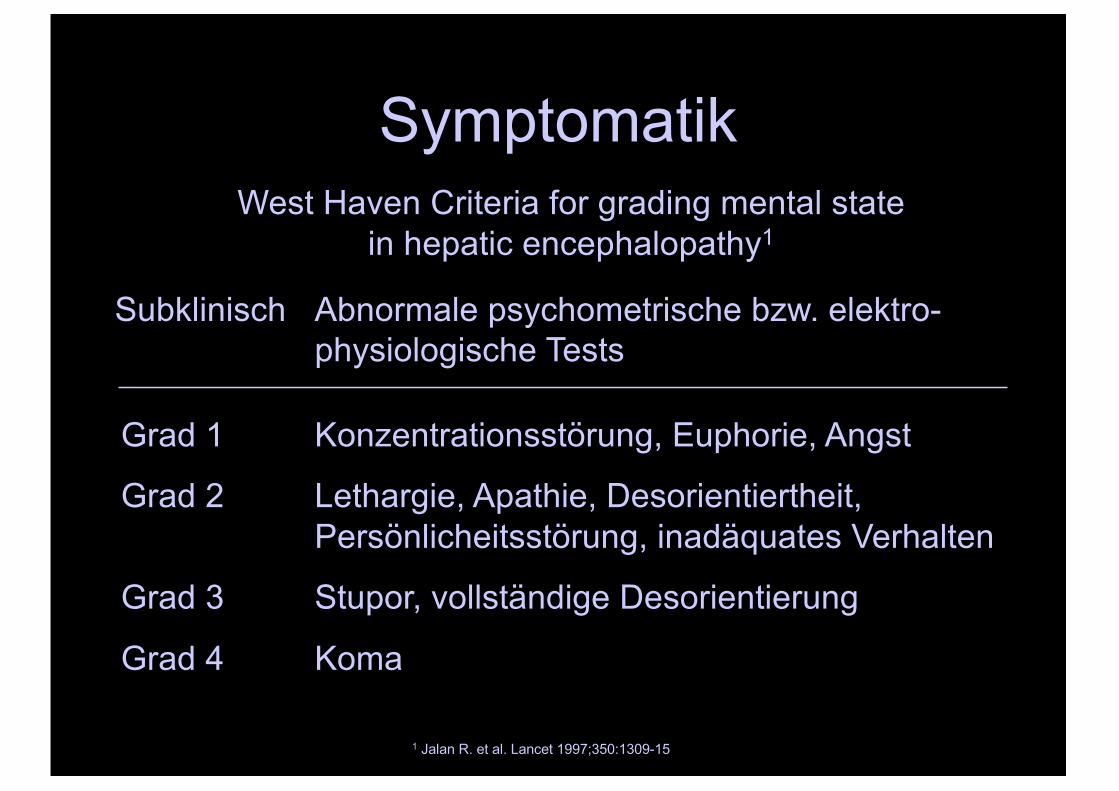
SymptomatikWest Haven Criteria for grading mental state
in hepatic encephalopathy1
Subklinisch Abnormale psychometrische bzw. elektro-physiologische Tests
Grad 1 Konzentrationsstörung, Euphorie, Angst
Grad 2 Lethargie, Apathie, Desorientiertheit,Persönlicheitsstörung, inadäquates Verhalten
Grad 3 Stupor, vollständige Desorientierung
Grad 4 Koma
1 Jalan R. et al. Lancet 1997;350:1309-15
Symptomatik
„Encephalopathy is a diagnosis of exclusion“1
1 Blei A.T. et al. Am J Gastro 2001;96 (7):1968-1976.
Komplikationen• Koagulopathie
- Synthesestörung vs. Sepsis/Hämolyse
• Sepsis-like-shock-Syndrom, ARDS- DD Sepsis (Faktor VIII)
• Hypoglykämie- Glukoneogenese ¯ , hepatischer Insulin-uptake ¯
• Hypokaliämie- Resp. Alkalose (renaler K+/H+-Exchange)
• Hyponatriämie• Metabolische Azidose• HPS/HRS• Infekte
- V.a. Gram+-Septikämie + Pilze (Candida/Aspergillus)
Therapie
• Keine spezifische Therapie möglich(Ausnahme: Antidots bei Intoxikationen)
• Supportive Therapie zur Erhaltung derOrganfunktionen und Behandlung der Komplikationen

Therapie
• Keine spezifische Therapie möglich(Ausnahme: Antidots bei Intoxikationen)
• Supportive Therapie zur Erhaltung derOrganfunktionen und Behandlung der Komplikationen
TherapieLebertransplantation (LTX)
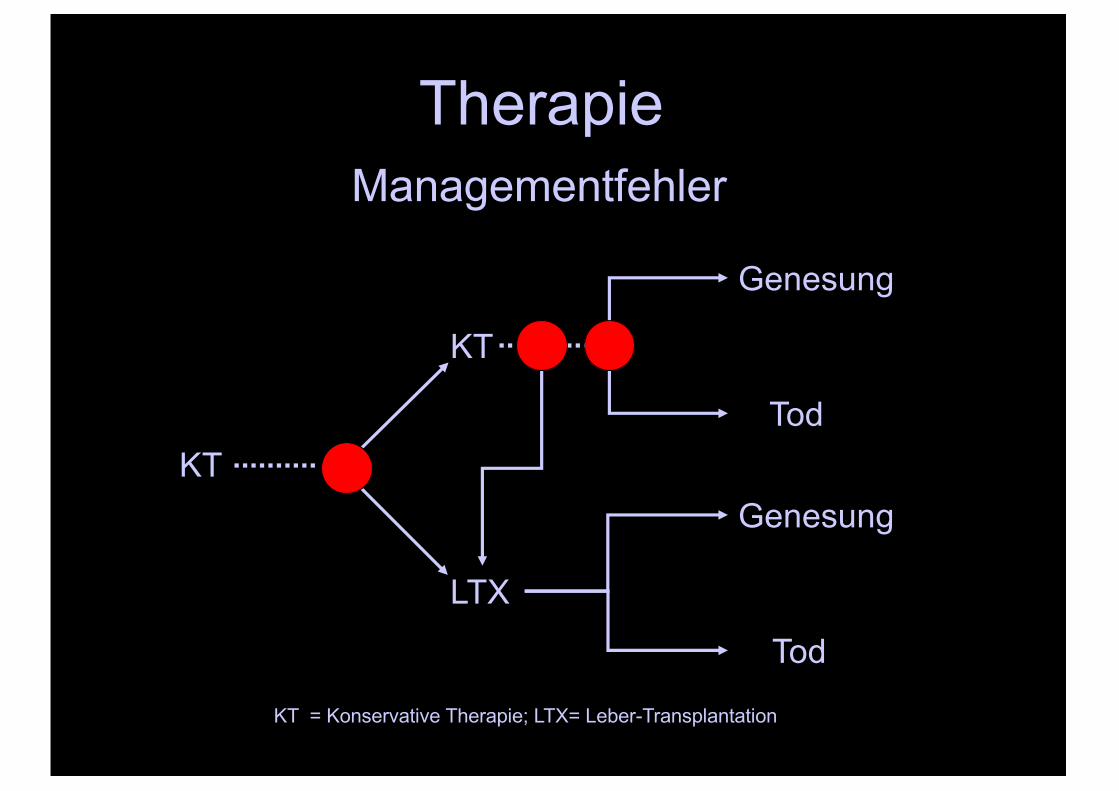
KT = Konservative Therapie; LTX= Leber-Transplantation
Therapie
KT
LTX
KT
Genesung
Tod
Genesung
Tod
Managementfehler
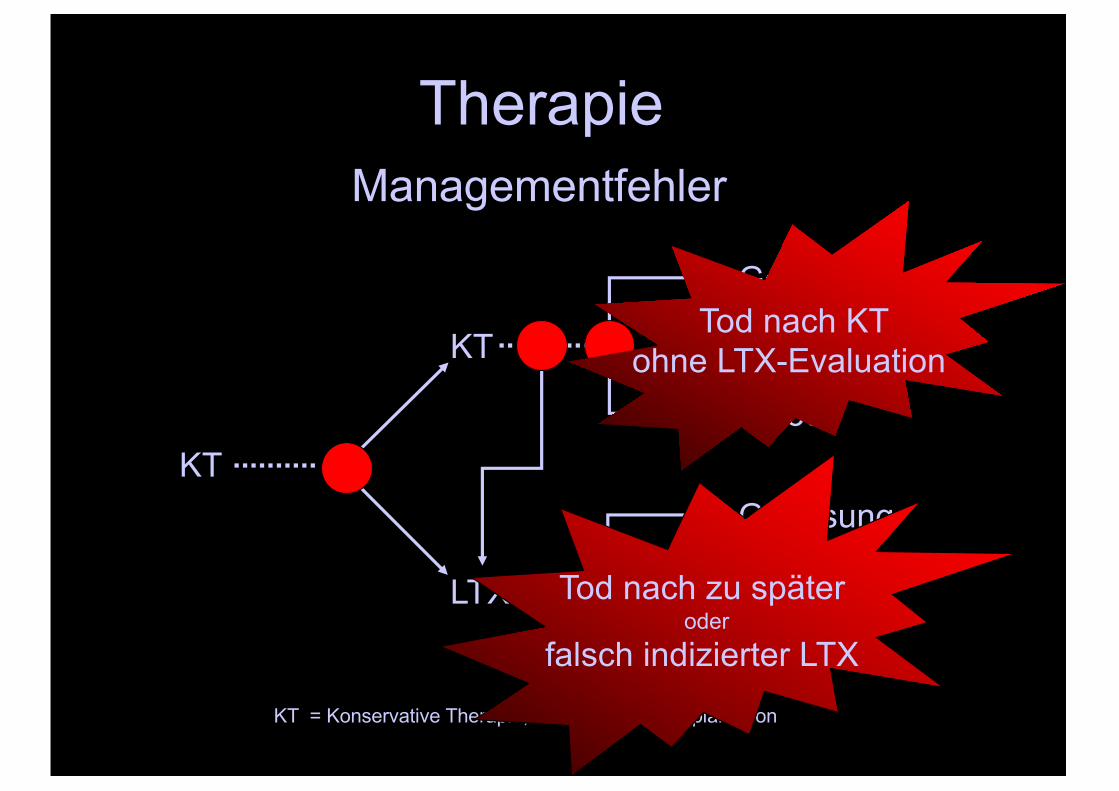
KT = Konservative Therapie; LTX= Leber-Transplantation
Therapie
KT
LTX
KT
Genesung
Tod
Genesung
Tod
Managementfehler
Tod nach KT ohne LTX-Evaluation
Tod nach zu später oder
falsch indizierter LTX
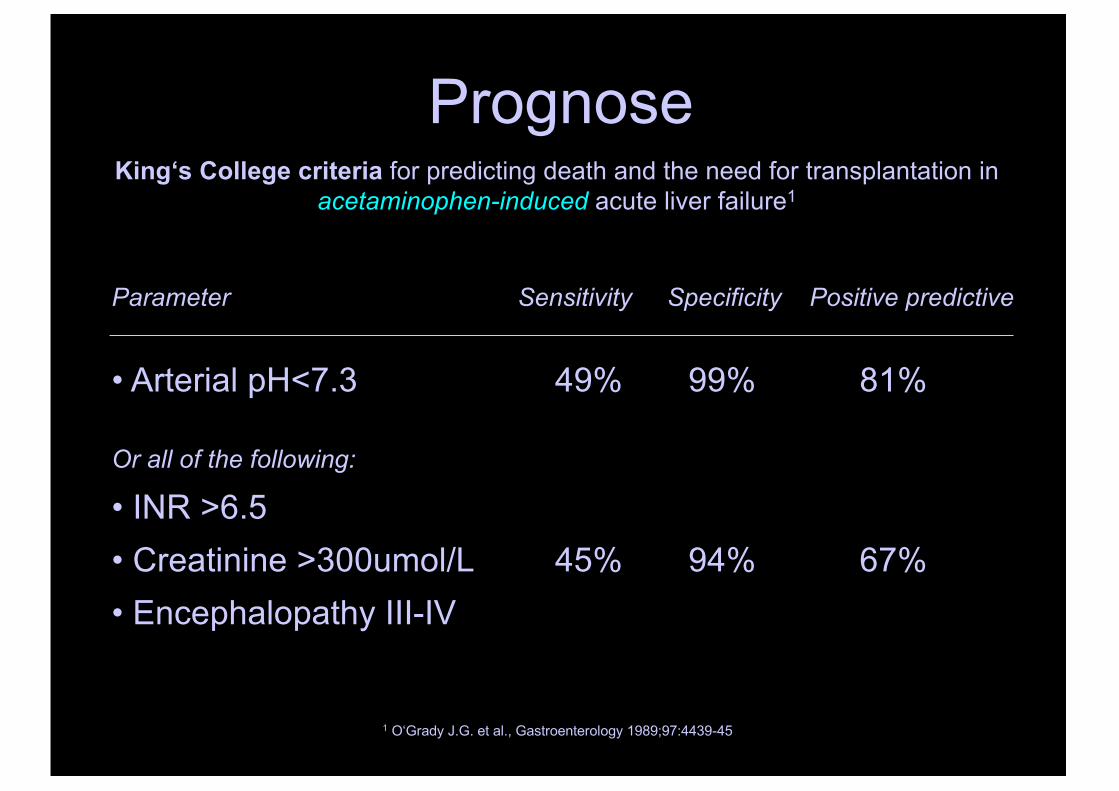
PrognoseKing‘s College criteria for predicting death and the need for transplantation in
acetaminophen-induced acute liver failure1
1 O‘Grady J.G. et al., Gastroenterology 1989;97:4439-45
Parameter Sensitivity Specificity Positive predictive
• Arterial pH<7.3 49% 99% 81%
Or all of the following:
• INR >6.5• Creatinine >300umol/L 45% 94% 67%• Encephalopathy III-IV
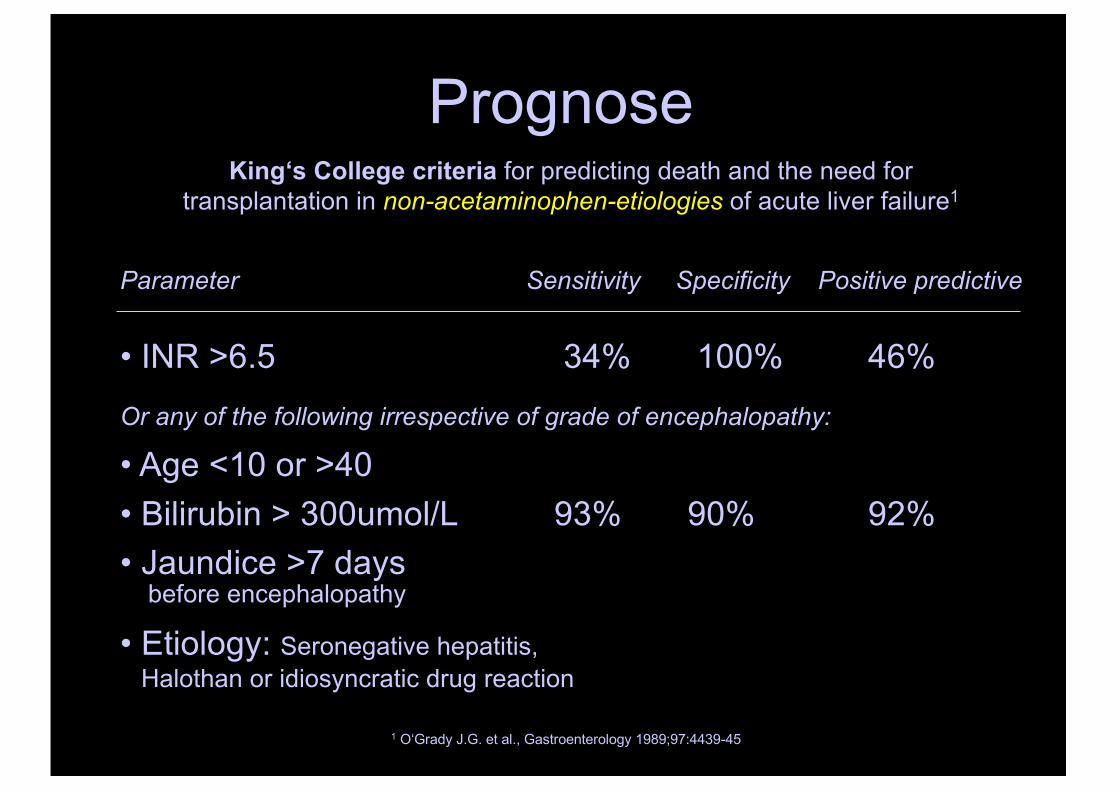
PrognoseKing‘s College criteria for predicting death and the need for
transplantation in non-acetaminophen-etiologies of acute liver failure1
1 O‘Grady J.G. et al., Gastroenterology 1989;97:4439-45
Parameter Sensitivity Specificity Positive predictive
• INR >6.5 34% 100% 46%Or any of the following irrespective of grade of encephalopathy:
• Age <10 or >40• Bilirubin > 300umol/L 93% 90% 92%• Jaundice >7 days
before encephalopathy
• Etiology: Seronegative hepatitis, Halothan or idiosyncratic drug reaction
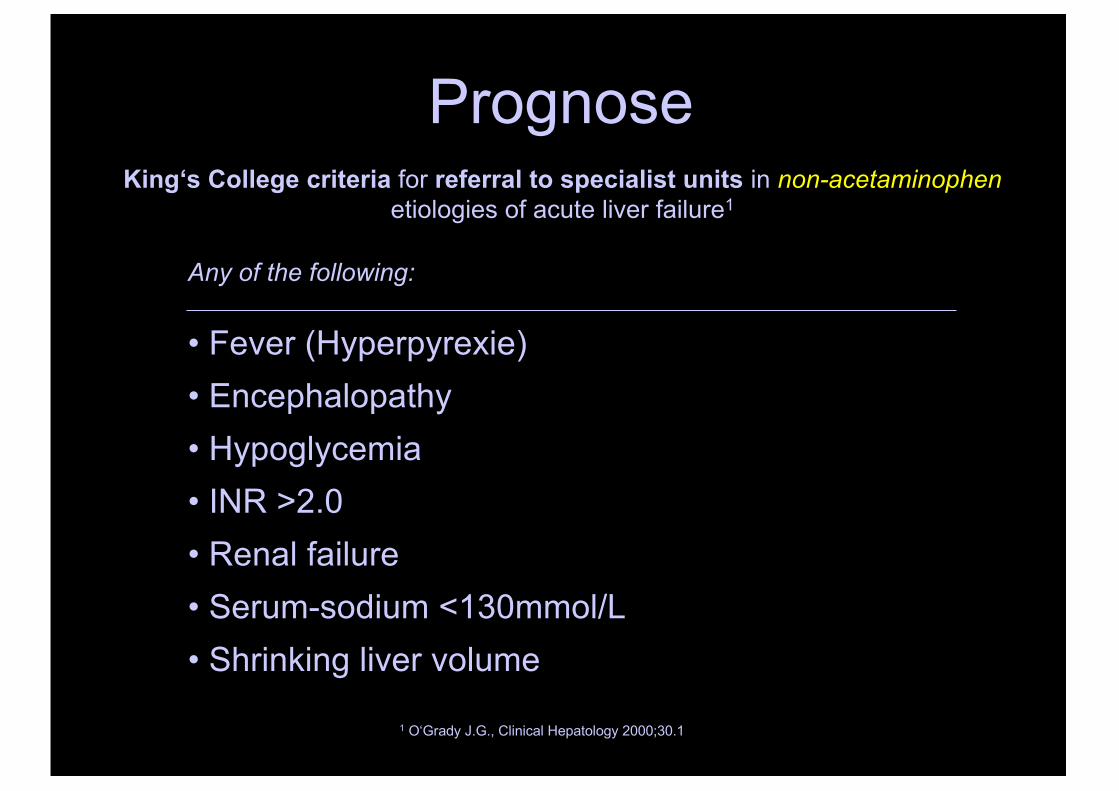
PrognoseKing‘s College criteria for referral to specialist units in non-acetaminophen
etiologies of acute liver failure1
Any of the following:
• Fever (Hyperpyrexie)• Encephalopathy• Hypoglycemia• INR >2.0• Renal failure• Serum-sodium <130mmol/L• Shrinking liver volume
1 O‘Grady J.G., Clinical Hepatology 2000;30.1
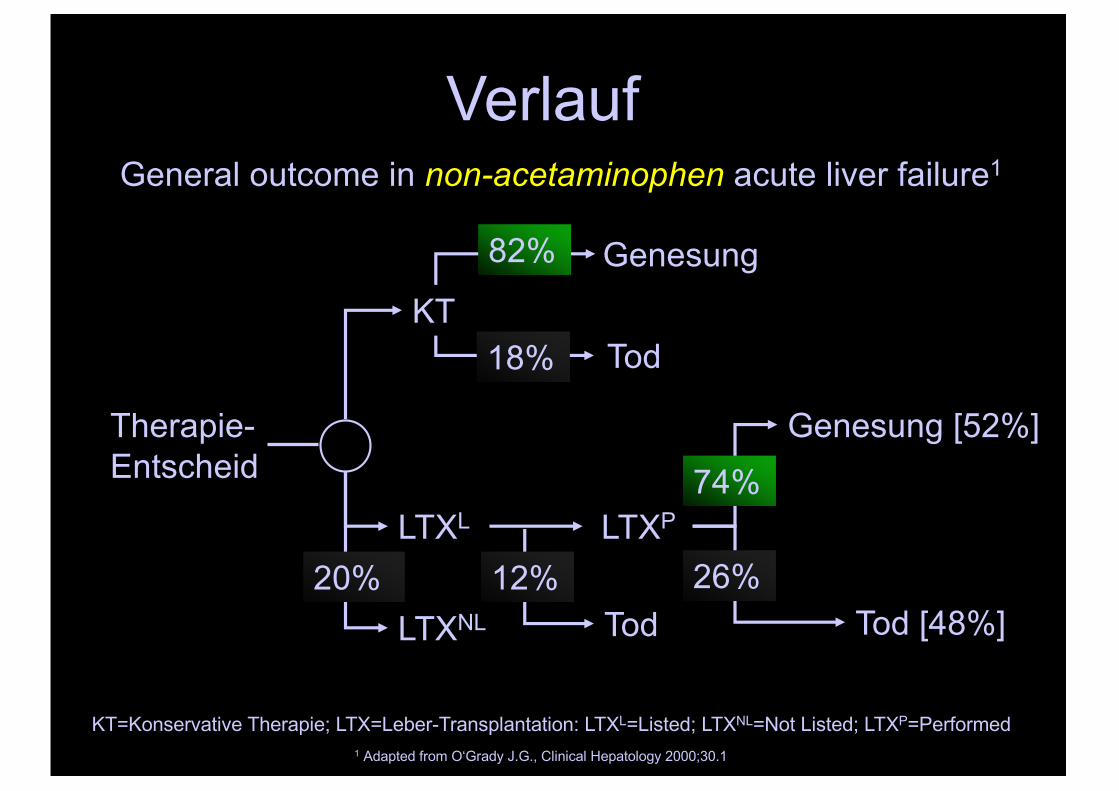
Verlauf
Therapie-Entscheid
LTXL
KTGenesung
Tod
Genesung [52%]
Tod
General outcome in non-acetaminophen acute liver failure1
1 Adapted from O‘Grady J.G., Clinical Hepatology 2000;30.1
LTXP
LTXNL
20% 12%Tod [48%]
26%
74%
18%
82%
KT=Konservative Therapie; LTX=Leber-Transplantation: LTXL=Listed; LTXNL=Not Listed; LTXP=Performed
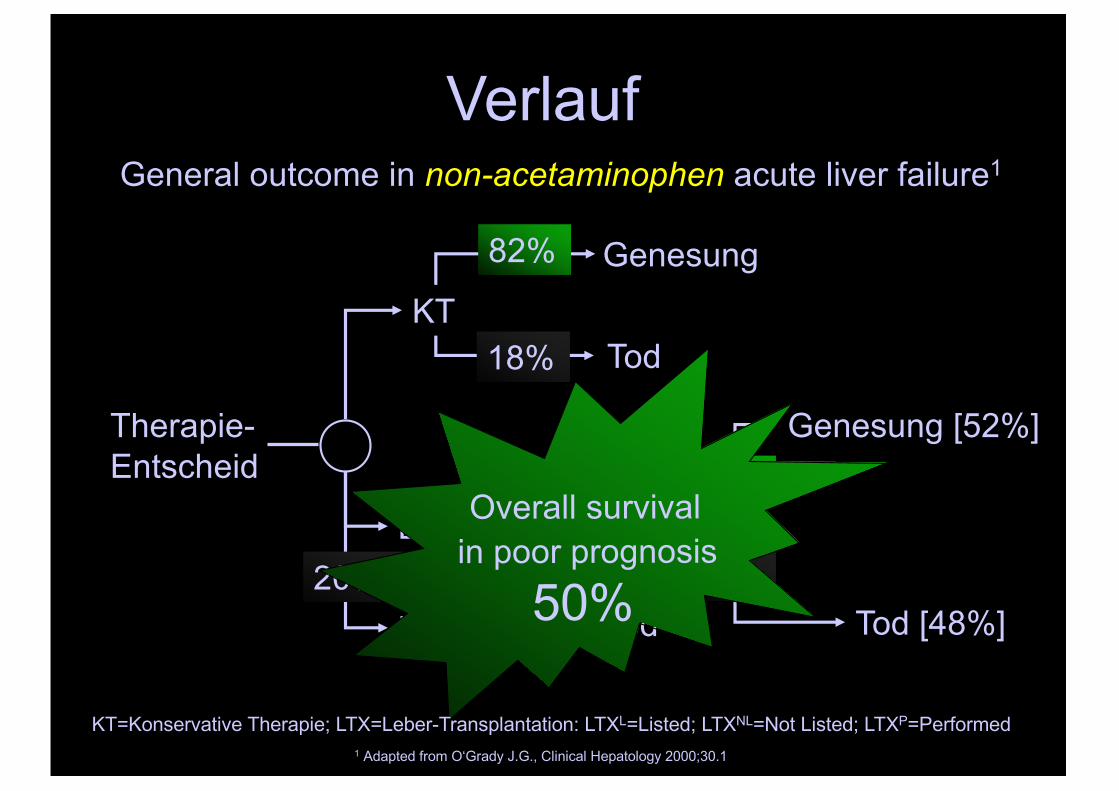
Verlauf
Therapie-Entscheid
LTXL
KTGenesung
Tod
Genesung [52%]
Tod
General outcome in non-acetaminophen acute liver failure1
1 Adapted from O‘Grady J.G., Clinical Hepatology 2000;30.1
LTXP
LTXNL
20% 12%Tod [48%]
26%
74%
18%
82%
KT=Konservative Therapie; LTX=Leber-Transplantation: LTXL=Listed; LTXNL=Not Listed; LTXP=Performed
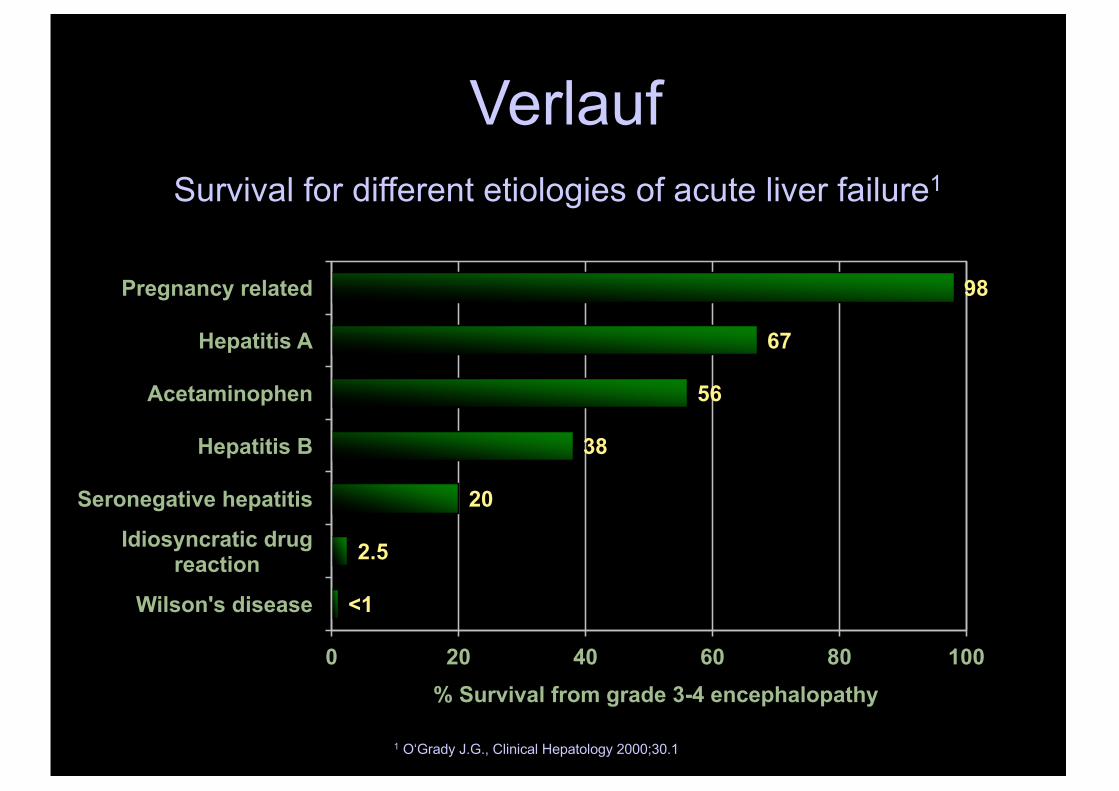
Verlauf
<1
2.5
20
38
56
67
98
0 20 40 60 80 100
Wilson's disease
Idiosyncratic drug reaction
Seronegative hepatitis
Hepatitis B
Acetaminophen
Hepatitis A
Pregnancy related
% Survival from grade 3-4 encephalopathy
1 O‘Grady J.G., Clinical Hepatology 2000;30.1
Survival for different etiologies of acute liver failure1
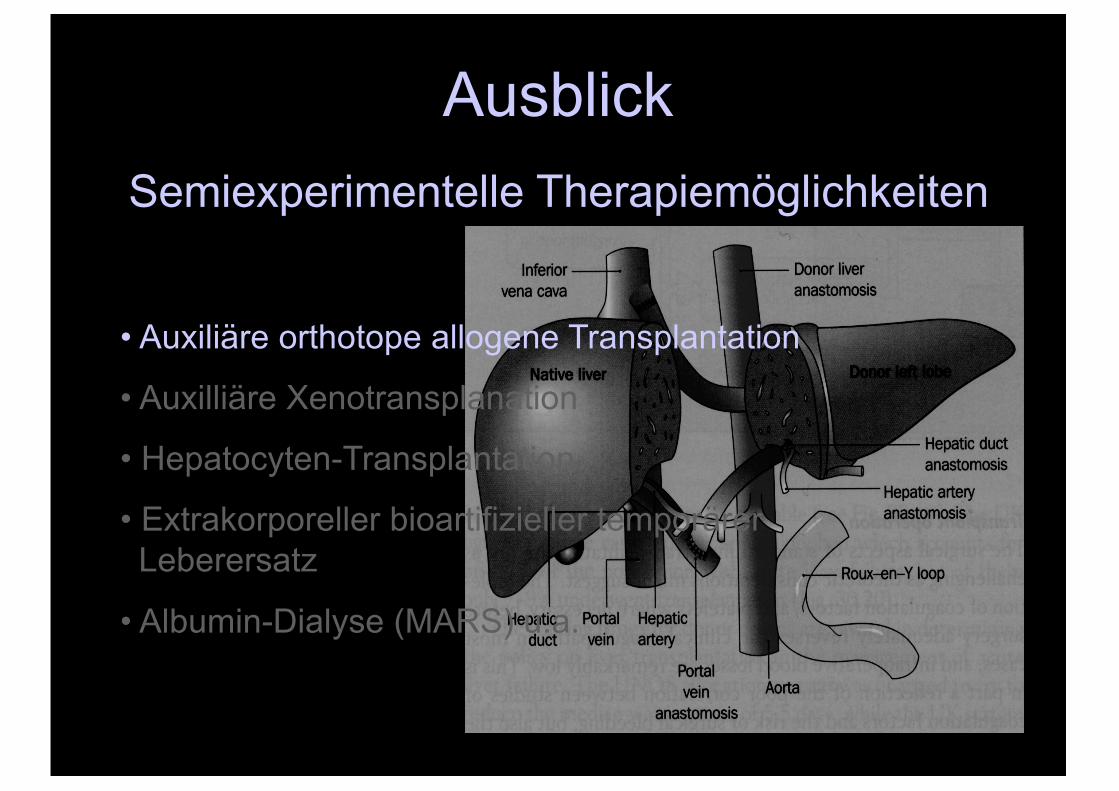
AusblickSemiexperimentelle Therapiemöglichkeiten
• Auxiliäre orthotope allogene Transplantation
• Auxilliäre Xenotransplanation
• Hepatocyten-Transplantation
• Extrakorporeller bioartifizieller temporärerLeberersatz
• Albumin-Dialyse (MARS) u.a.
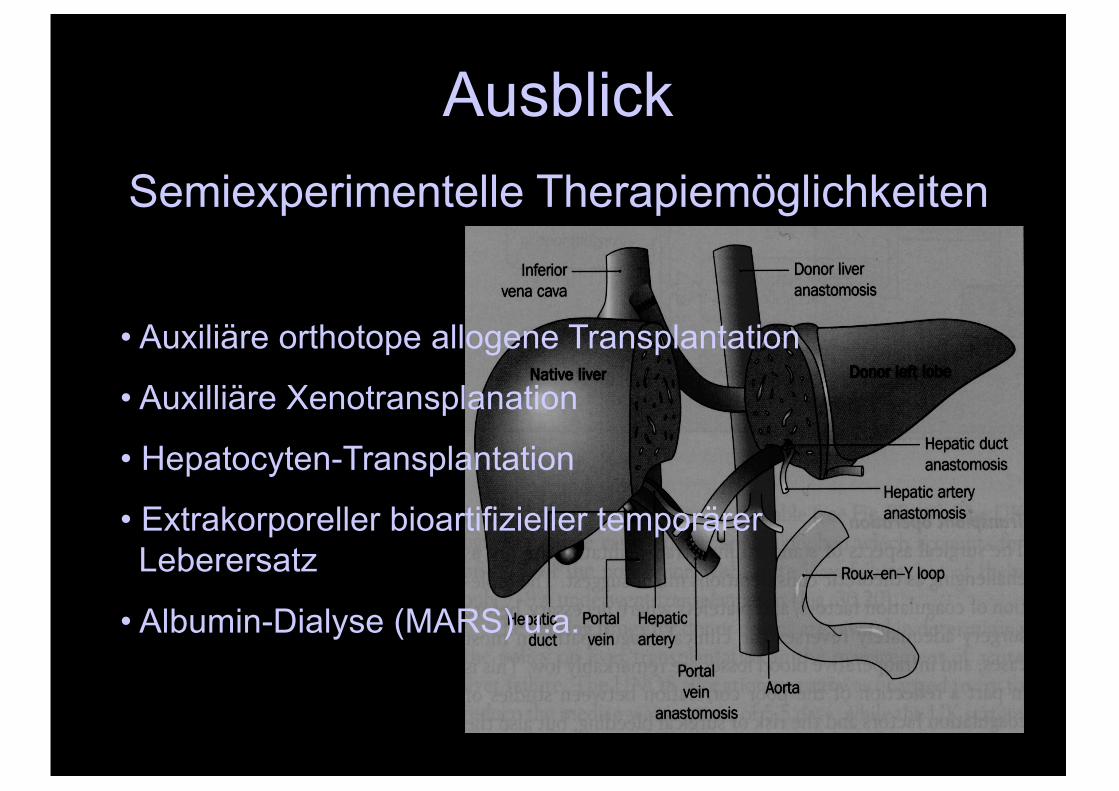
AusblickSemiexperimentelle Therapiemöglichkeiten
• Auxiliäre orthotope allogene Transplantation
• Auxilliäre Xenotransplanation
• Hepatocyten-Transplantation
• Extrakorporeller bioartifizieller temporärerLeberersatz
• Albumin-Dialyse (MARS) u.a.
Akutes Leberversagen