Chirurgische Optionen der terminalen Herzinsuffizienz … · ca. eine Million Menschen leiden in...
54
Chirurgische Optionen der terminalen Herzinsuffizienz Dr. U. Herold Dr. P. Libera Prof. Dr. R. Lange
Transcript of Chirurgische Optionen der terminalen Herzinsuffizienz … · ca. eine Million Menschen leiden in...
Chirurgische Optionen der terminalen Herzinsuffizienz
Dr. U. Herold
Dr. P. Libera
Prof. Dr. R. Lange
Chirurgische Optionen der terminalen Herzinsuffizienz

ca. eine Million Menschen leiden in der Bundesrepublik an Herzinsuffizienz
davon versterben ca. 200.000 Personen in jedem Jahr
ca. 2.500 von diesen könnten durch eine Herztransplantationgerettet werden
für diese stehen allerdings nur ca. 500 Spenderherzen pro Jahr zur Verfügung
Chirurgische Optionen der terminalen Herzinsuffizienz Morbidität und Mortalität bei Herzinsuffizienz

HTX / MCSHerztransplantationHerzunterstützung
i.v. TherapieIntravenöse Katecholamintherapie
Dilatation / Bypassnur bei ischämischer Kardiomyopathie
zusätzlich ß-Blocker
Diuretika, Glykoside, ACE-Hemmer
Diät, Veränderung der Lebensweise
Chirurgische Optionen der terminalen Herzinsuffizienz Herzinsuffizienz – Hierarchie der Behandlungsverfahren

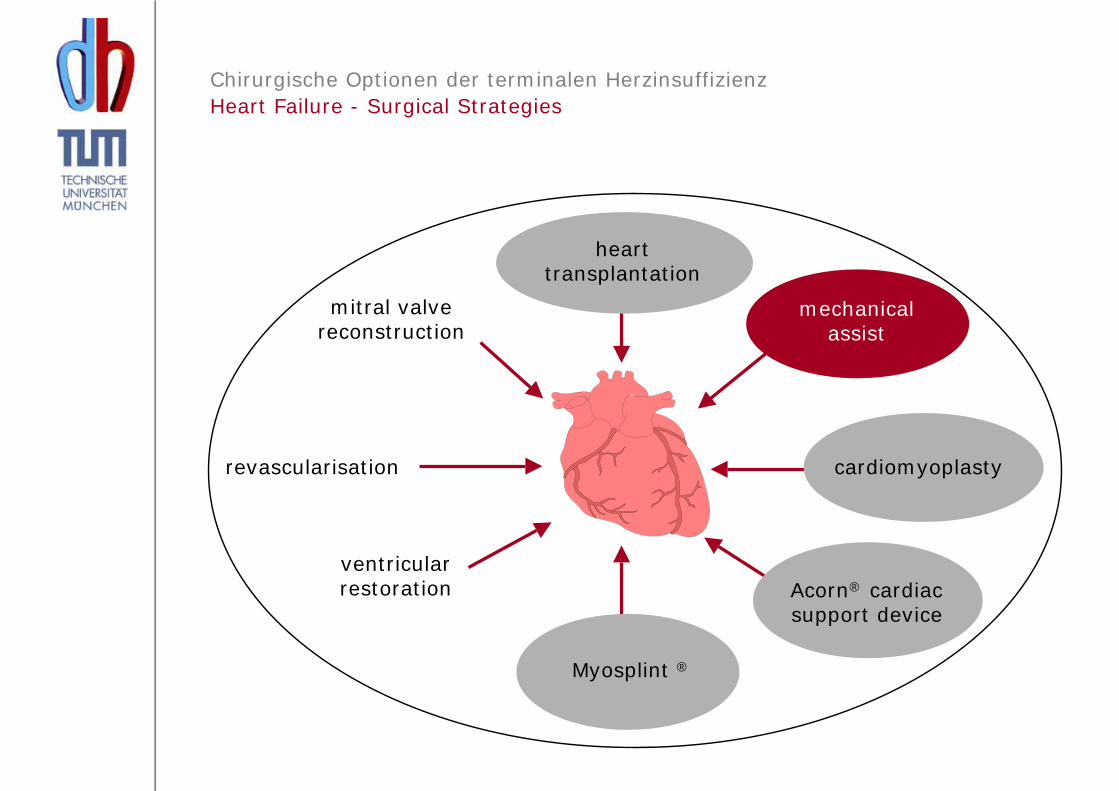
revascularisation
mitral valvereconstruction
hearttransplantation
mechanicalassist
cardiomyoplasty
Acorn® cardiacsupport device
Myosplint ®
ventricularrestoration
Chirurgische Optionen der terminalen HerzinsuffizienzHeart Failure - Surgical Strategies
Chirurgische Optionen der terminalen HerzinsuffizienzHistorie
Barnard, C.N. (1967) A human cardiac transplant: an interim report of a successful operation performed at Groote Schuur Hospital, Capetown. S. Afr. Med. J. 41, 1271 - 1274.
Erste erfolgreiche Herztransplantation am 3. Dezember 1967.
C.N. Barnard N.E. Shumway
HistorieErste erfolgreiche Herztransplantation am 3. Dezember 1967

Lower und Shumway 1960
HistorieTechnik der orthotopen Herztransplantation

03.12.1967 Kapstadt 1. Klinische Herztransplantation (18 Tage)
12.12.1967 New York USA ( 6 Tage)
27.04.1968 Paris Europa (53 Std.)
13.02.1969 München Deutschland (22 Std.)
1969 # 52 HTx weltweit, 24 Pat .lebend(1-Jahres ÜL: 20 %)
1974 # 260 HTx weltweit, 43 Pat. lebend(1-Jahres ÜL: 35 %)
HistorieFortschritte der Klinischen Herztransplantation

• 1972Endomyokardbiopsie zur Abstoßungsdiagnostik
• 1974Antithymocytenglobulin (ATG) zur Abstoßungsbehandlung (München)
• 1978"Hirntod" als Todeszeitpunkt
• 1979Erster Langstreckentransport eines Spenderorgans
• 1980Einführung von Cyclosporin A
HistorieMeilensteine der Klinischen Herztransplantation

Yacoub et al. 1990
Dreyfus et al. 1991
Hypothetische Vorteile:
- bessere atriale Transportfunktion
- verminderte Arrhythmogenität
- verminderte AV-Klappenunsuffizienz
- geringere Thrombogenität der Nahtreihen
HistorieBicavale, bipulmonalvenöse Anstomosierung

Standard Technik(Lower and Shumway)
Bicavale Anastomosen Totale Orthotope Transplantation
Technische Modifikationen
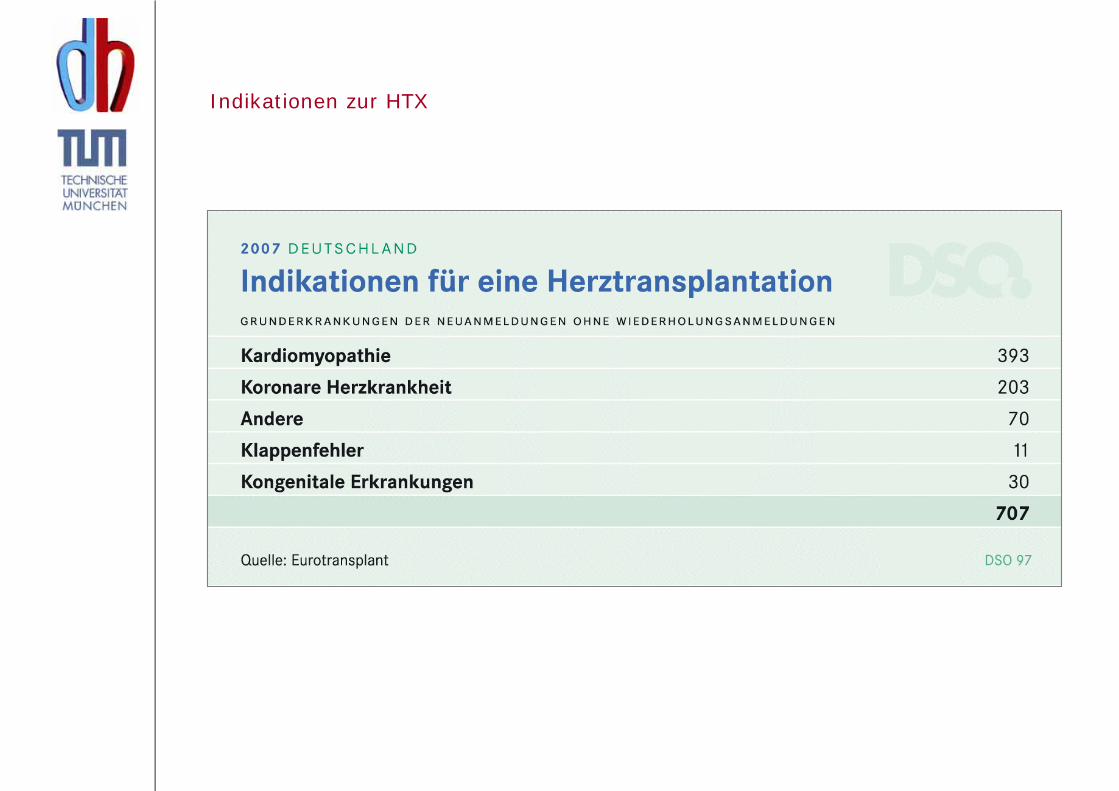
Indikationen zur HTX

HTX Bedarf

Pulmonaler Gefäßwiderstand >5 Wood E
transpulmonaler Gradient > 15 mmHg
Infektion Nierenversagen ?
Malignome Leberversagen ?
Drogenabhängigkeit Arteriopathie ?
Präformierte AK Non-Compliance ?Alter ?
HerztransplantationKontraindikationen

Empfängerherz (dil. CMP) Spenderherz
Orthotope Herztransplantation

HTX – Spender
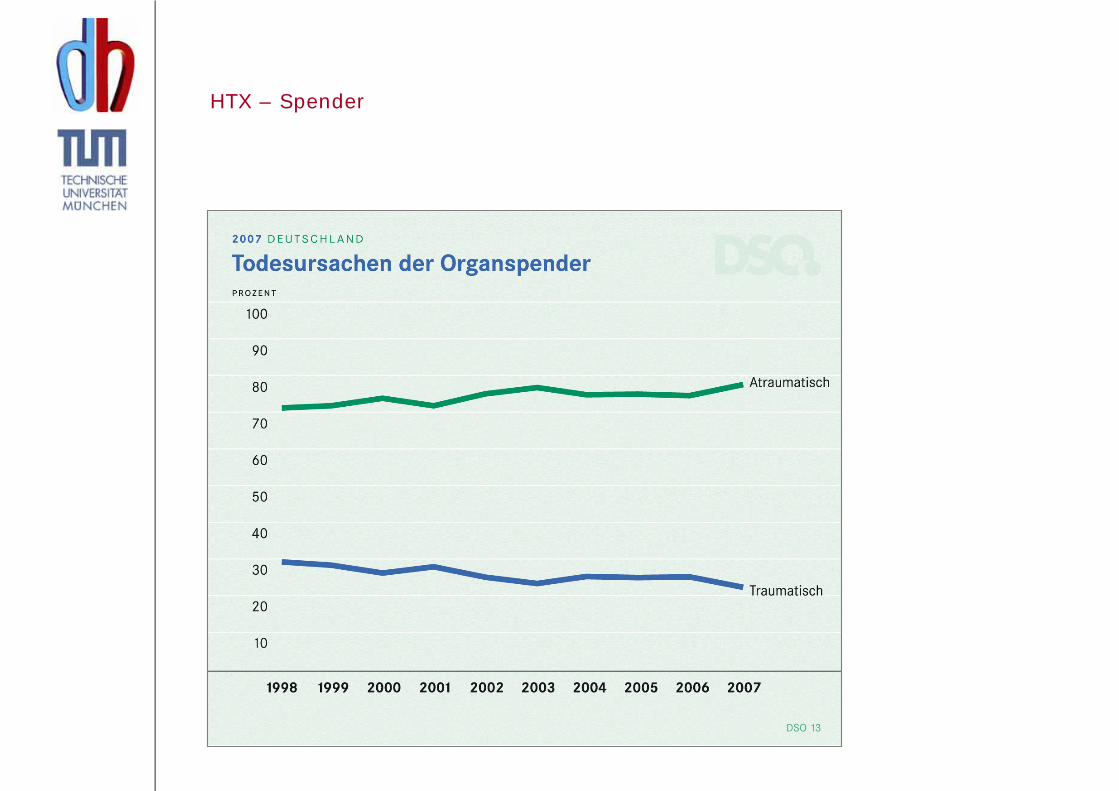
HTX – Spender
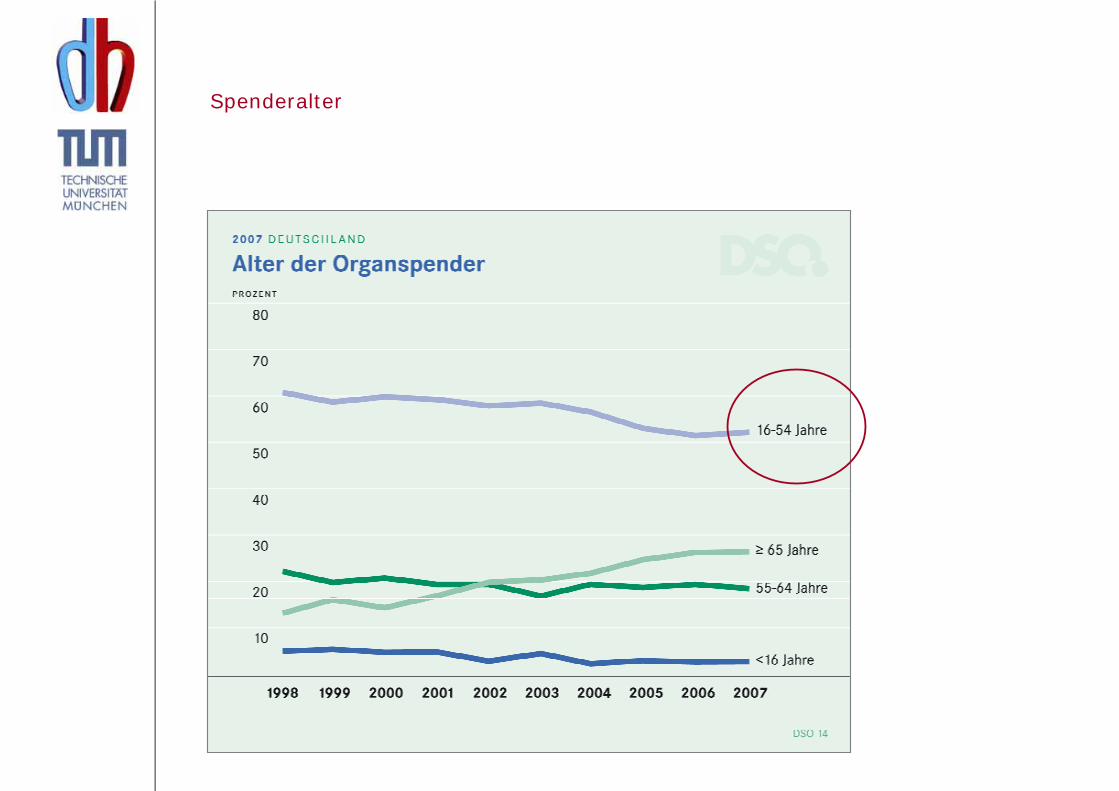
Spenderalter

HTX – Operation
Postoperativ Immunsuppression
Immunsuppressionschema
• Kortikosteroide (Cortison)
• Calcineurin-Phosphatase-Inhibitoren (Cyclosporin)
• Antiproliferative Substanzen (Azathioprin)
Fakultativ: Antikörperpräparate
Neuere Substanzen: - Tacrolimus (Fk506)- Mycophenolat mofetil (MMF)
Postoperativ Immunsuppression

Herzmuskelbiopsie
Durchführung:in wöchentlichen Abständen ab 7. postoperativen Tag
HerztransplantationPostoperative Therapie
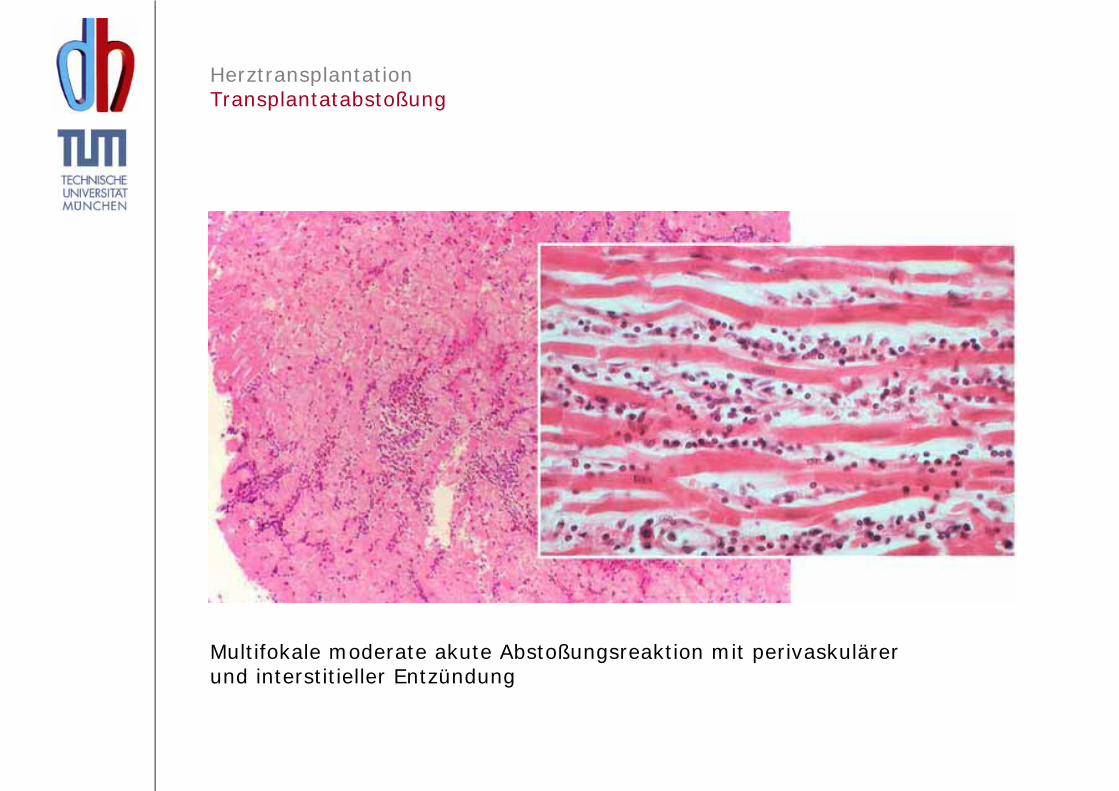
Multifokale moderate akute Abstoßungsreaktion mit perivaskulärer und interstitieller Entzündung
HerztransplantationTransplantatabstoßung
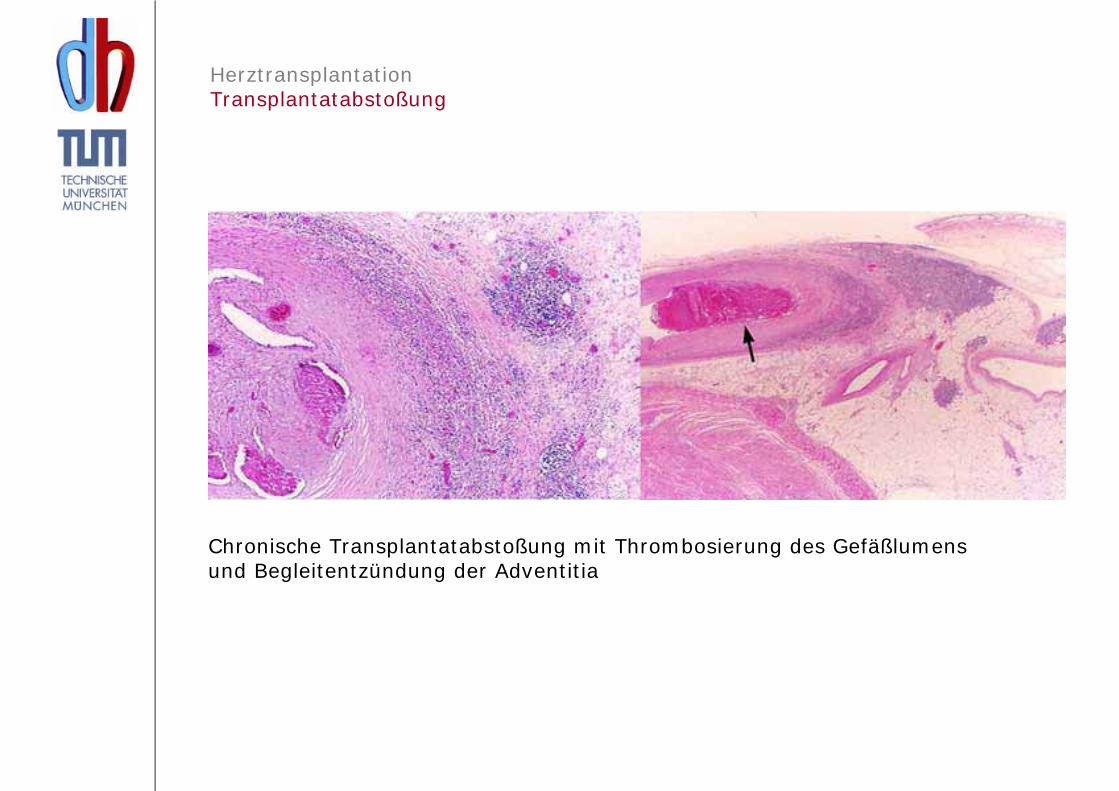
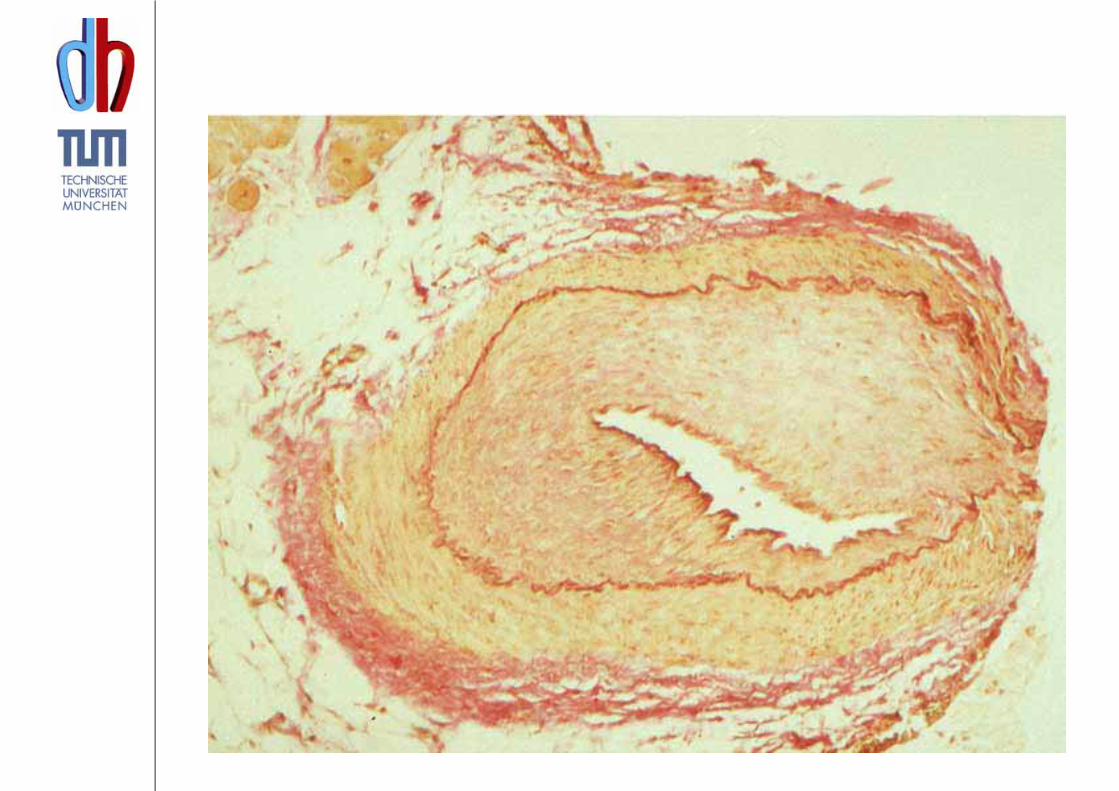
Chronische Transplantatabstoßung mit Thrombosierung des Gefäßlumensund Begleitentzündung der Adventitia
HerztransplantationTransplantatabstoßung
Durchschnittliche 1-Jahresüberlebensrate 85%
• primäres Tx-Versagen führend innerhalb der ersten 30 Tage,
die akute Abstoßung folgt auf Rang zwei.
Jährliche Mortalität anschließend bei 4%
• 2 + 3 Jahre nach Tx: Infektion, Abstoßung, Tumore und
Transplantatvaskulopathie etwa gleich häufig
• ≥4 Jahre stellen Tumore und Infektionen häufigste Todesursache dar,
Tx-Vaskulopathie bei 17%.
• 5 Jahre nach Tx: 10,4% der Patienten zeigen S-Krea-Anstieg
über 2,5mg/dl, 2,5% bereits unter Nierenersatztherapie
Hummel M, Hetzer R. Herztransplantation in Deutschland 2002
Zentralbibl Chir 2003;128:788-795
HerztransplantationGesamtdeutsche HTX-Daten

Continuous Factors
Recipient age
Recipient weight
Donor age
Ischemia time
Transplant center volume
PA systolic pressure
PVR
Bilirubin
Serum creatinine
2007ISHLTJ Heart Lung Transplant 2007;26: 769-781
ADULT HEART TRANSPLANTATION(1/2002 - 6/2005) Risk Factors for 1 Year Mortality

ADULT HEART TRANSPLANTATION Kaplan-Meier Survival Stratified by Rejection Within 1st YearConditional on survival to 1 year for transplants: 1/1999 - 6/2004
Years
Surv
ival
(%)
50
60
70
80
90
100
0 1 2 3 4 5 6 7
No rejection (N=4,832) Rejection (N=3,694)
p < 0.0001
2007ISHLTJ Heart Lung Transplant 2007;26: 769-781
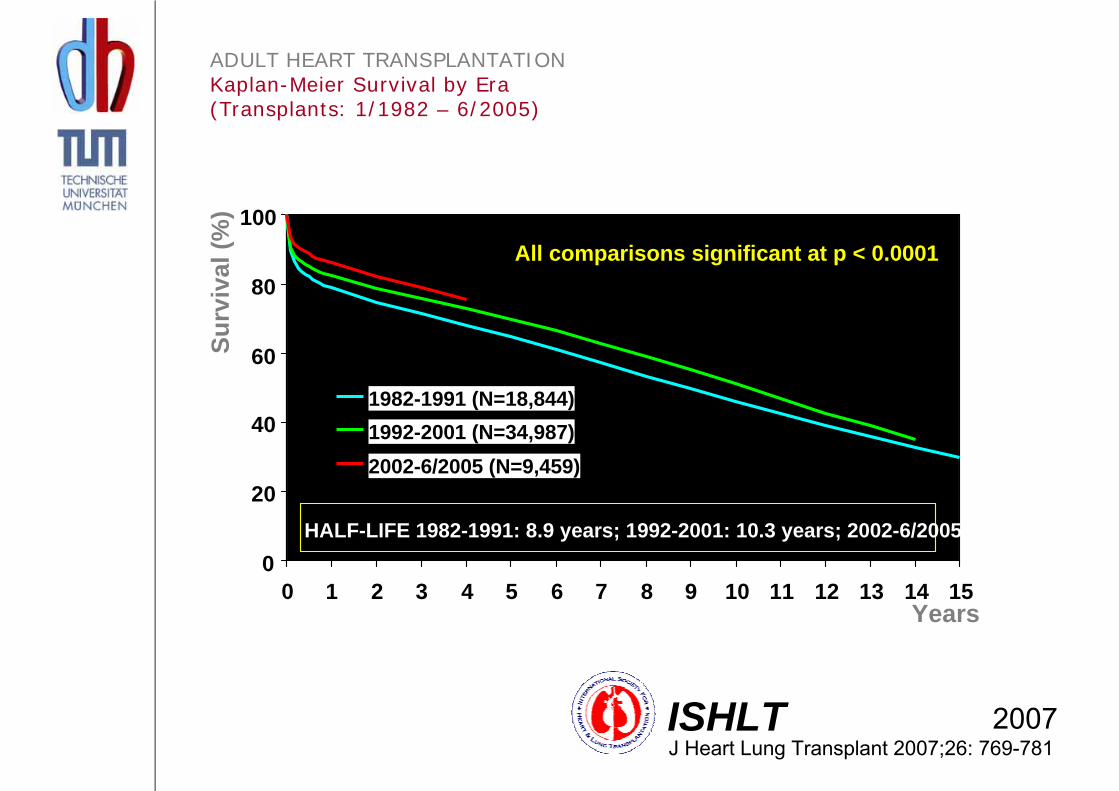
0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
1982-1991 (N=18,844)1992-2001 (N=34,987)2002-6/2005 (N=9,459)
All comparisons significant at p < 0.0001
HALF-LIFE 1982-1991: 8.9 years; 1992-2001: 10.3 years; 2002-6/2005: NA
2007ISHLTJ Heart Lung Transplant 2007;26: 769-781
ADULT HEART TRANSPLANTATION Kaplan-Meier Survival by Era (Transplants: 1/1982 – 6/2005)
Years
Surv
ival
(%)

0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Cardiomyopathy (N = 21,707)Coronary artery disease (N = 21,661)Congenital diagnosis (N = 773)Retransplant (766)Valvular (N= 1,506)Other (N= 929)
All pair-wise comparisons are significant at p <.05 except Cardiomyopathy vs. valvular (p = 34), valvular vs. other (p= .14), andCongenital vs. other (p = .12).
HALF-LIFE Cardiomyopathy: 13.3 years; CAD: 11.3 years; Congenital: 17.1 years; Retransplant: 9.3 years; Valvular: 13.4 years; Other: 14.4 years
2007ISHLTJ Heart Lung Transplant 2007;26: 769-781
Years
Surv
ival
(%)
ADULT HEART TRANSPLANTATION Kaplan-Meier Survival by Diagnosis Conditional on Survival to 1 Year (Transplants: 1/1982 - 6/2005)

0%
20%
40%
60%
80%
100%
1 Year (N = 15,388) 3 Years (N = 13,600) 5 Years (N = 11,698) 7 Years (N = 9,306)
No Activity Limitations Performs with Some Assistance Requires Total Assistance
2007ISHLTJ Heart Lung Transplant 2007;26: 769-781
ADULT HEART TRANSPLANTATION Functional Status of Surviving Recipients (Follow-ups: 1995 - June 2006)
Years
Surv
ival
(%)

• Medikamentöse Therapie (ACE-Hemmer, Betablocker…)
• Ursachenadaptierte Therapie (AK-Apherese, Interferon…)
• Herzschrittmachersysteme: biventrikuläres Pacing, AICD
• Assist-Device: Tandem-Heart, Novacor etc.
• Herzkatheterinterventionen (PTCA, Stentimplantation,Laserrekanalisation)
• Score + Untersuchungsmethoden wie 6-Minute-Walktest etc.
• Monitoring von Biomarkern wie NT-Pro-BNP
• Spezielle Trainings- und Schulungsprogramme
Verbessertes Herzinsuffizienzmanagement

Spendersituation

Zukunft Xenotransplantation ?„Das Schwein in mir!“
revascularisation
mitral valvereconstruction
hearttransplantation
mechanicalassist
cardiomyoplasty
Acorn® cardiacsupport device
Myosplint ®
ventricularrestoration
Chirurgische Optionen der terminalen HerzinsuffizienzHeart Failure - Surgical Strategies
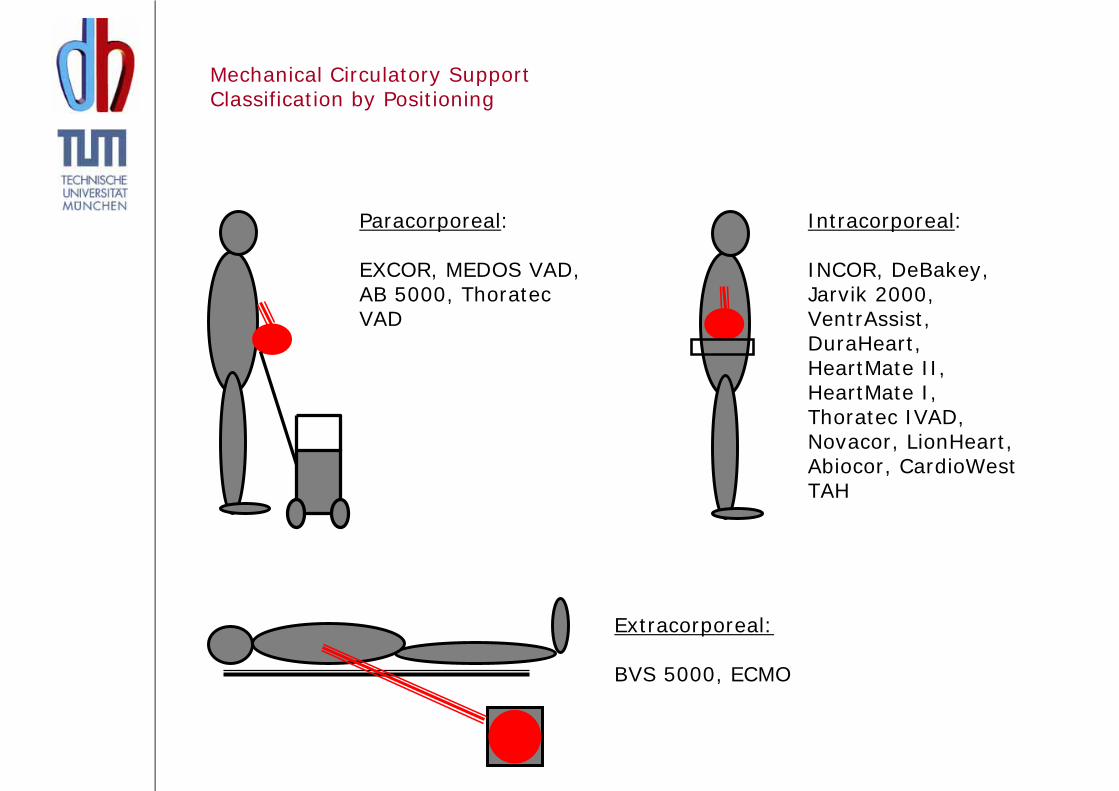
Intracorporeal:
INCOR, DeBakey,Jarvik 2000, VentrAssist, DuraHeart, HeartMate II,HeartMate I,Thoratec IVAD, Novacor, LionHeart,Abiocor, CardioWestTAH
Paracorporeal:
EXCOR, MEDOS VAD, AB 5000, ThoratecVAD
Extracorporeal:
BVS 5000, ECMO
Mechanical Circulatory SupportClassification by Positioning
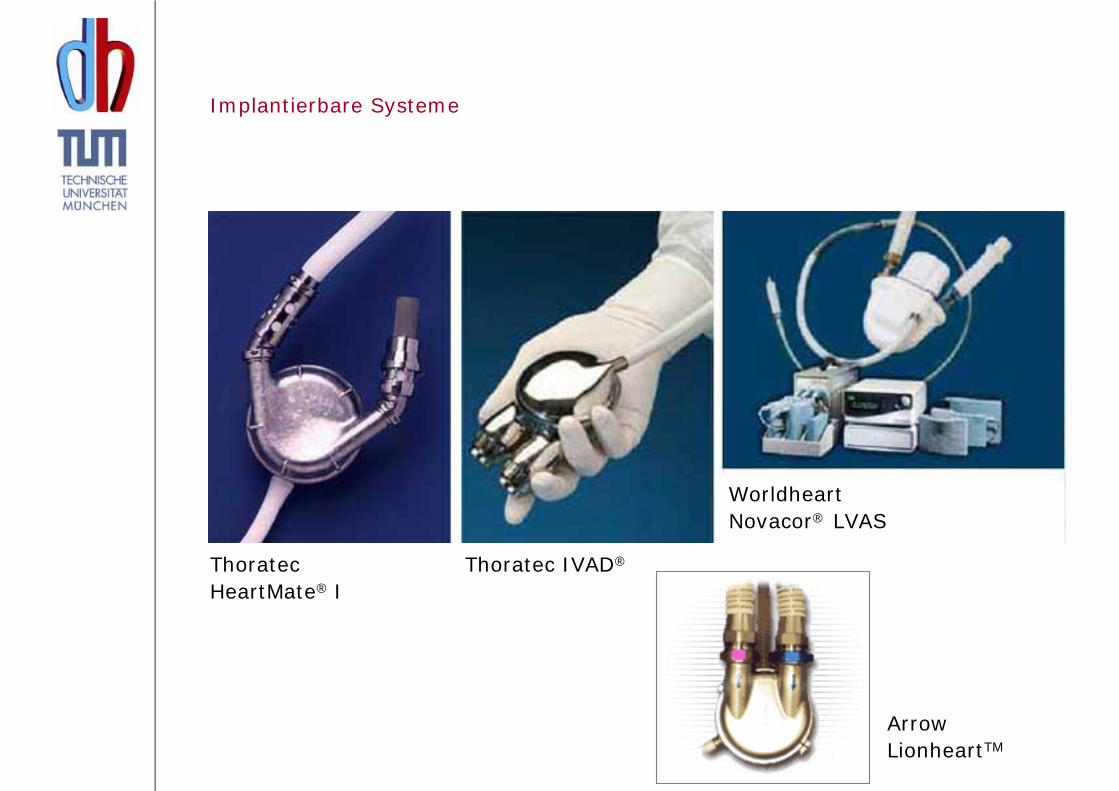
ThoratecHeartMate® I
Thoratec IVAD®
ArrowLionheartTM
Implantierbare Systeme
Worldheart Novacor® LVAS

Abiomed
AbiocorTM TAH
Syncardia
CardiowestTM TAH
Total Artificial Heart

Berlin Heart EXCOR pedriatic
Ventrikuläre Unterstützungssysteme
• Bridge to transplant Überbrückung bis zur Transplantation
• Destination-Therapie Definitive Kreislaufunterstützung (keine TX)
• Bridge to recovery Überbrückung bis zur Erholung der Ventrikelfunktion

Mittelfristige Überbrückung?Mittelfristige Überbrückung?
„bridge to recovery“
• Akute Herzinsuffizienz bei Myocarditis (z.B. Virusmyokarditis)
• Bei ca. 5% der dilatativen/ ischämischen Cardiomyopathien deutliche Verbesserung der Herzfunktion – Explantation möglich

Case Report
A 37-year-old woman was admitted in cardiogenic shock and beginning multiorgan failure.
The patient had suffered from a cold for one week. On echocardiography, the left-ventricular function was reduced to 35%.
Within 24 hours the left-ventricular function decreased dramatically to 7%.
We decided to implant a biventricular assist device.

Diagnosis: Enterovirus myocarditis On 25. post-op day the BVAD was explanted. Global ventricular function had normalized.
Langfristige Unterstützung?Langfristige Unterstützung?

Linksherzunterstützungssystem

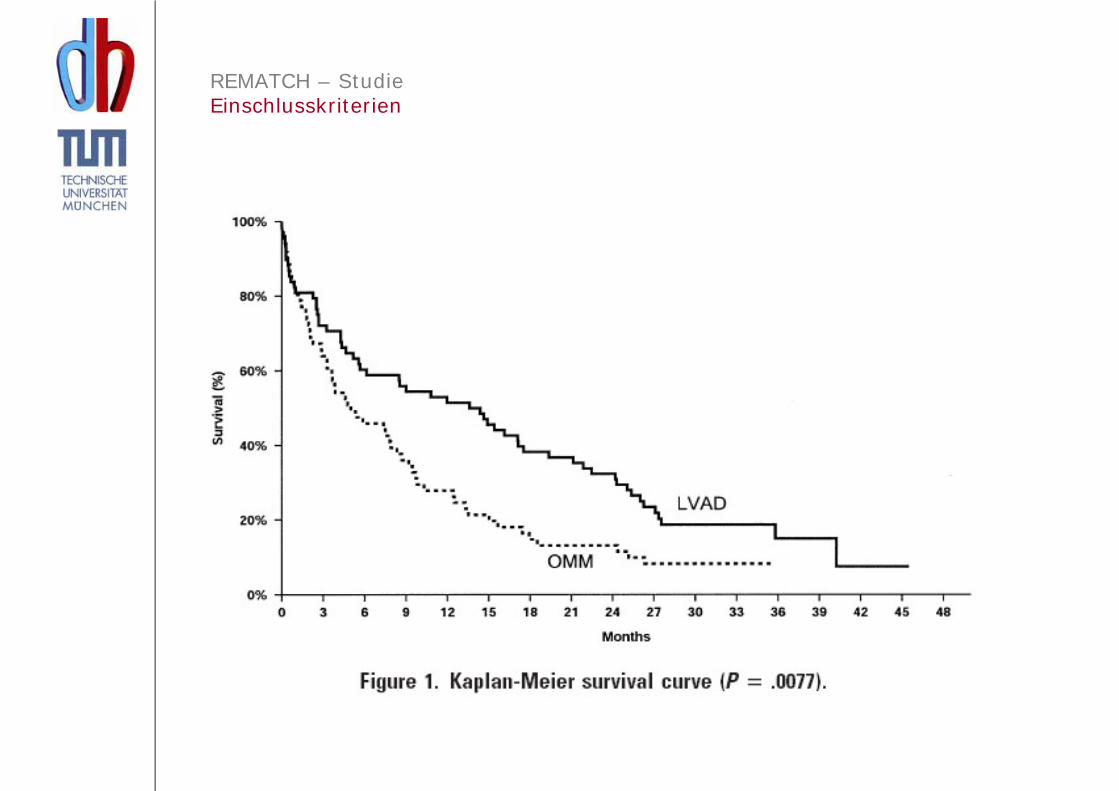
REMATCH – Studie(Randomized Evaluation of Mechanical Assistance for the Treatment ofCongestive Heart Failure)
• Überlebensrate nach ein und zwei Jahren unter medikamentöser Therapie vs. mech. Linksherzunterstützung
• Lebensqualität (NYHA, MLHF)
• Thoratec Heart Mate Unterstützungssystem
Left ventricular assist devices as destination therapy: A new look at survival
Soon J. ParkJ Thorac Cardiovasc Surg.2005 Jan;129(1):9-17

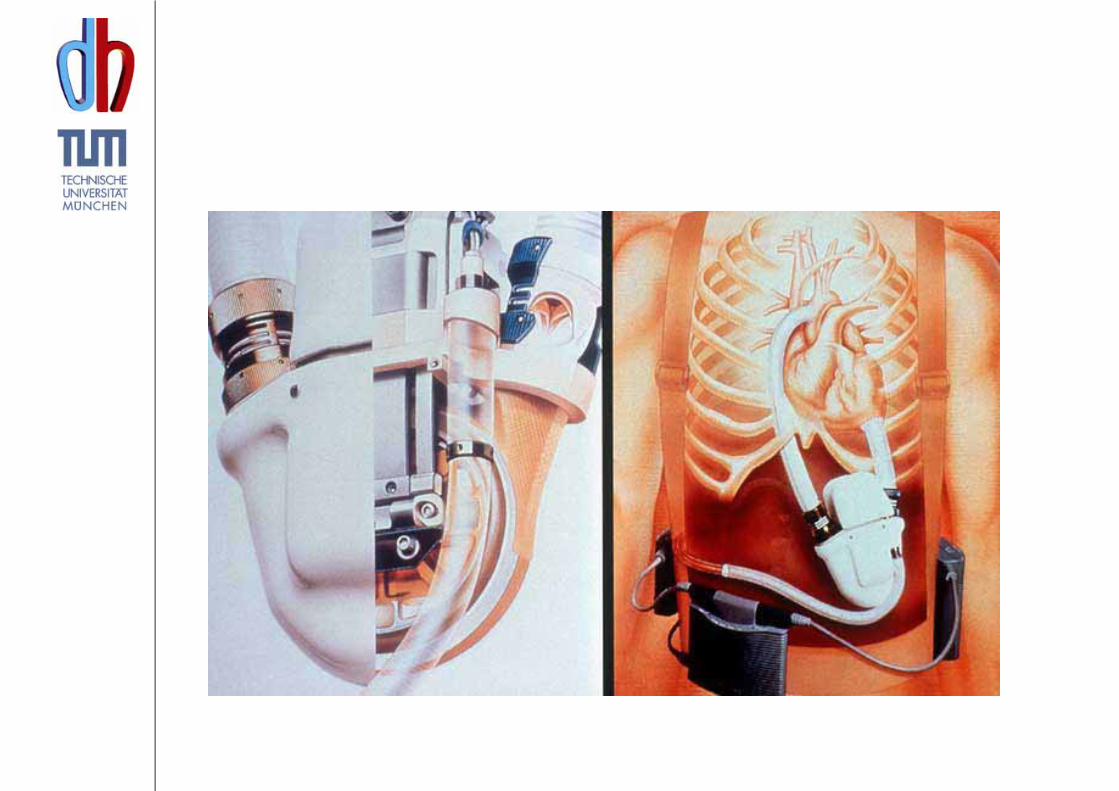
• Pulsatiles, pneumatisch angetriebenes Herzunterstützungssystem
• Komplett implantierbares System
• N = 129 Patienten– 68 LVAD– 61 OMM (optimal medical management)
Thoratec Heart Mate XVE LVAD

REMATCH – StudieEinschlusskriterien
• NYHA IV
• EF < 25%
• Maximale Sauerstoffaufnahme <14ml/kgoder intravenöse inotrope Therapie
• Transplantation kontraindiziert– > 65 Jahre– Insulinpflichtiger Diabetes mellitus mit Endorganschäden– Chronische Niereninsuffizienz
REMATCH – StudieEinschlusskriterien

NYHA-Klassifikation
• OMM: 17% Klasse I/II• LVAD: 71% Klasse I/II
MLHF (Minesota Living with Heart Failure score)
• OMM: 53 Punkte• LVAD: 42 Punkte
REMATCH – StudieLebensqualität

Auf Wiedersehen !