Kostimulationsblockade: Revolution in der Immunsuppression? · •Früher...
35
Kostimulationsblockade: Revolution in der Immunsuppression? Christian Morath Med. Klinik, Nephrologie
Transcript of Kostimulationsblockade: Revolution in der Immunsuppression? · •Früher...

Kostimulationsblockade: Revolution in der
Immunsuppression?
Christian Morath
Med. Klinik, Nephrologie

Disclosure
• Keine Zuwendung von Firmen, deren Produkte hier erwähnt werden

Fa. ABC

Gescheiterte Revolution?
Fa. ABC

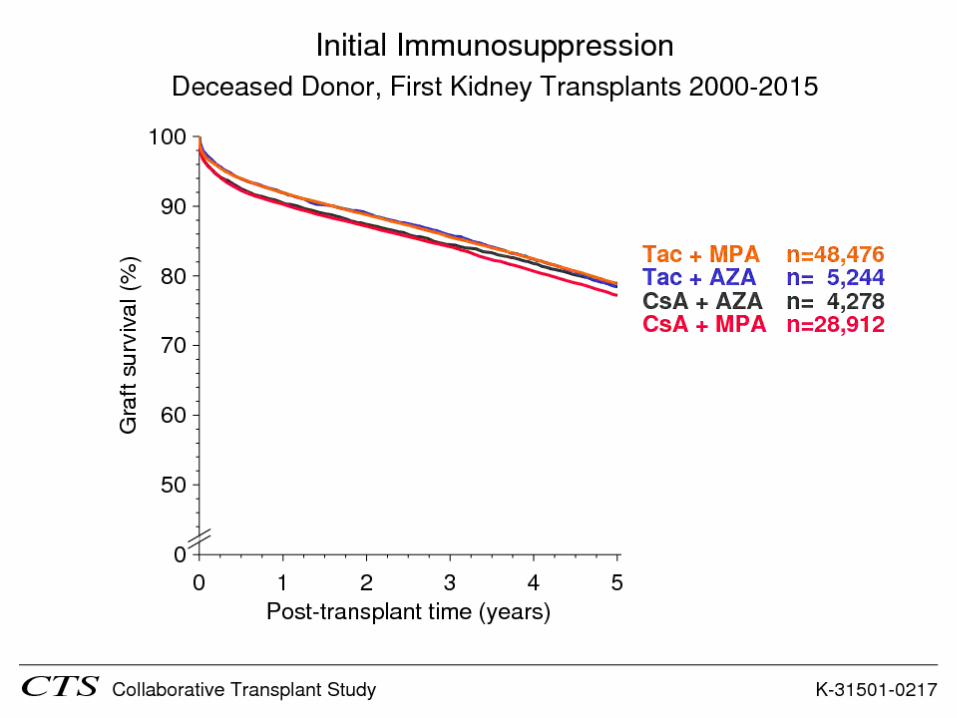
www.ctstransplant.org; *1.-Verstorbenen-Nierentransplantation
2009-2011 (Prognose)* 10-Jahres Transplantatüberleben: 66%
Halbwertszeit: 20,3 Jahre
CNI- Effekt
„Lern“- Effekt

Halloran, N Engl J Med 2004
Calcineurininhibitoren (Cyclosporin, Tacrolimus)

KDIGO Guidelines
(+ IL2- or ATG-Induction)
Kasiske and Zeier (Co-Chairs), Am J Transplant 2009

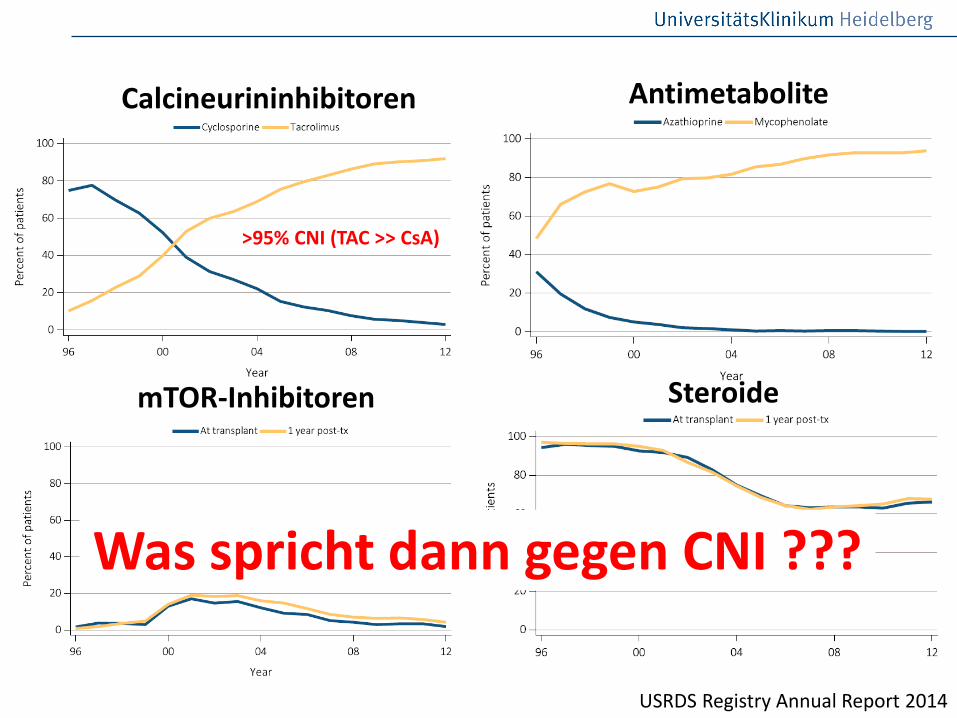
Calcineurininhibitoren Antimetabolite
mTOR-Inhibitoren Steroide
USRDS Registry Annual Report 2014
>95% CNI (TAC >> CsA)
Calcineurininhibitoren Antimetabolite
mTOR-Inhibitoren Steroide
USRDS Registry Annual Report 2014
>95% CNI (TAC >> CsA)
Was spricht dann gegen CNI ???

Calcineurininhibitortoxizität !
Nankivell, N Engl J Med 2003

Calcineurininhibitortoxizität !
Nankivell, N Engl J Med 2003
Überschätzt aber nicht 0!

Calcineurininhibitor-NW !
Wekerle, Transplantation, Klinik 2011
Was sind die Alternativen ?
• Früher Calcineurininhibitor-Entzug und Ersatz mittels mTOR-Inhibitor (Everolimus, Sirolimus)
• De novo Calcineurininhibitor-frei unter Einsatz eines Kostimulationsblockers (z.B. Belatacept)

Kostimulatorische Signalwege
Summers de Luca, Nat Rev Immunol 2012
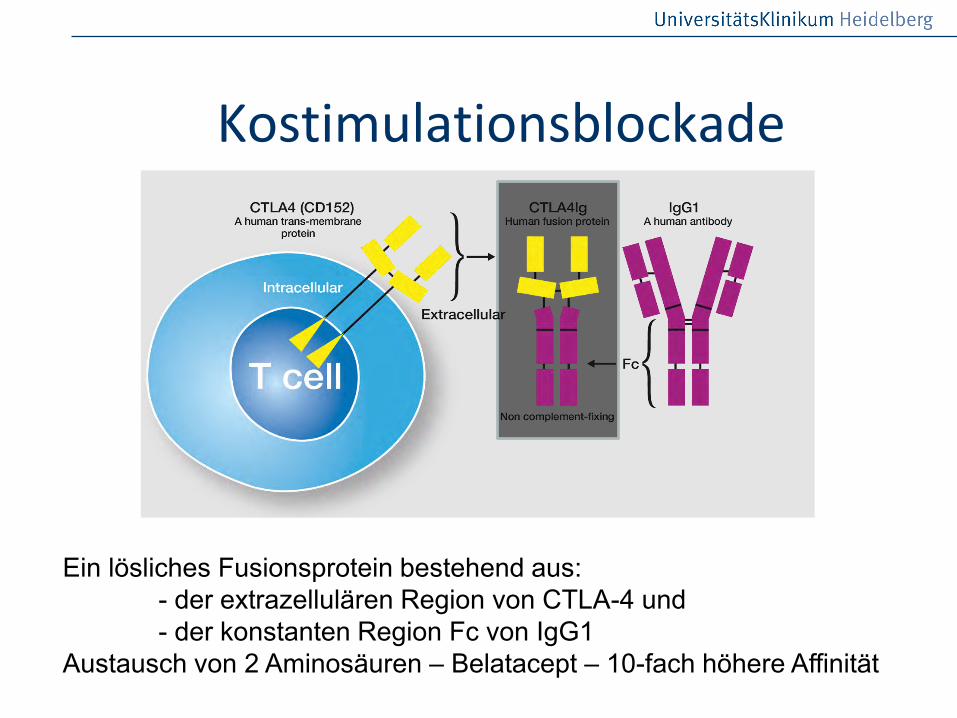
Kostimulationsblockade
Ein lösliches Fusionsprotein bestehend aus: - der extrazellulären Region von CTLA-4 und - der konstanten Region Fc von IgG1 Austausch von 2 Aminosäuren – Belatacept – 10-fach höhere Affinität

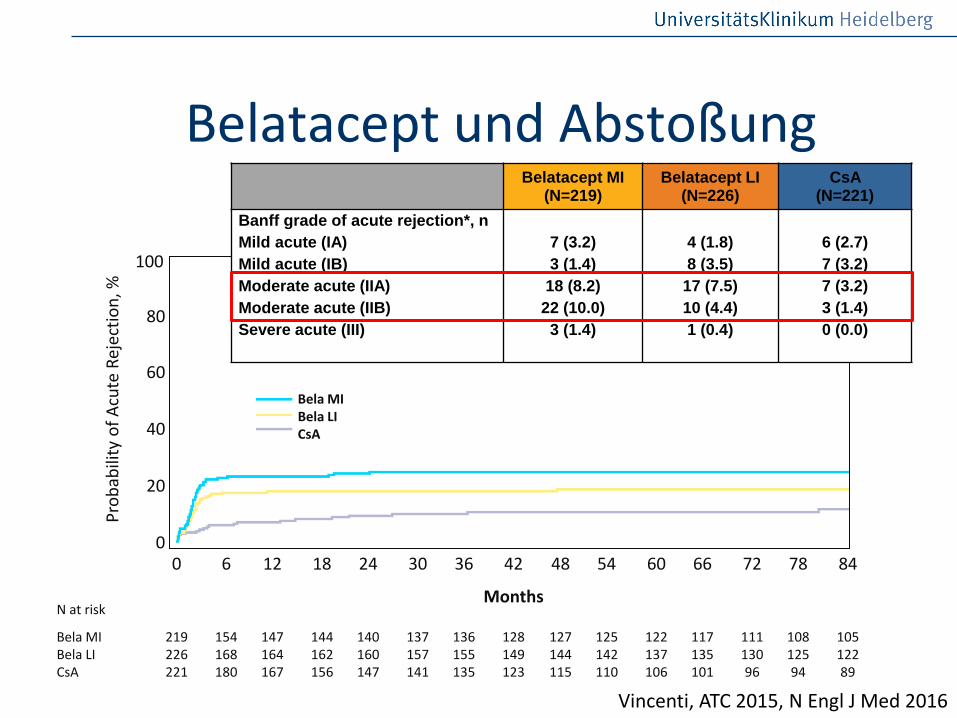
Vincenti, ATC 2015, N Engl J Med 2016
Belatacept statt CNI
Placebo infusions
All patients received basiliximab induction, MMF, and CS .
Transplantation
100–250 ng/mL
10 mg/kg
14 28 56 84 DAY 1 5
10 mg/kg
14 28 42 56 70 84 112 140 168 DAY 1 5
Day 1
CsAb (7 ± 3 mg/kg daily)
Belatacept MI
28 DAY 1
12
150–300 ng/mL
6 months
5 mg/kg every 4 weeks
5 mg/kg every 4 weeks
36 24
Primary
Approved regimen
Belatacept LI
CsA=cyclosporine A; LI=less intensive; MI=more intensive.

Vincenti, ATC 2015, N Engl J Med 2016
Belatacept statt CNI M
ean
cG
FR
, m
L/m
in/1
.73m
2 (
95%
CI)
Patients with measurements
MI: 214 192 179 170 136 132 122 109
LI: 220 192 189 174 142 140 126 115
CsA: 210 186 163 149 107 98 93 74
77.9 ml/min 74.0 ml/min
50.7 ml/min p<0.001
43%-ige Reduktion von Transplantatverlust oder Tod (MI/LI versus CsA)

Belatacept statt CNI
• Niedrigere Inzidenz an NODAT
• Niedrigere Inzidenz an HTN
• Niedrigere Triglyzeride
• Aber …

8,8
5,49
3,3
0,740,49
0,25
1,75
0
1,75
0,250
0,25
0
1
2
3
4
5
6
7
8
9
10
All PTLD CNS PTLD Non-CNS PTLD
Pati
en
ts (
%)
Bela EBV (-) (n = 91)
Bela EBV (+) (n = 810)
CsA EBV (-) (n = 57)
CsA EBV (+) (n = 399)
Belatacept und PTLD
Kumuliert bis März 2011
Vincenti, ATC 2015, N Engl J Med 2016
Belatacept und Abstoßung
100
0
Pro
bab
ility
of
Acu
te R
ejec
tio
n, %
Bela MI Bela LI CsA
P-value HR (95% CI) Bela MI vs CsA 0.0001 2.649 (1.596, 4.397) Bela LI vs CsA 0.0302 1.905 (1.124, 3.232)
0 6 12 18 24 30 36 42 48 54 60 66 72 78 84
Months
219 226 221
154 168 180
147 164 167
144 162 156
140 160 147
137 157 141
136 155 135
128 149 123
127 144 115
125 142 110
122 137 106
117 135 101
111 130 96
108 125 94
105 122 89
Bela MI Bela LI CsA
N at risk
20
40
60
80
Belatacept MI (N=219)
Belatacept LI (N=226)
CsA (N=221)
Banff grade of acute rejection*, n
Mild acute (IA)
Mild acute (IB)
Moderate acute (IIA)
Moderate acute (IIB)
Severe acute (III)
7 (3.2)
3 (1.4)
18 (8.2)
22 (10.0)
3 (1.4)
4 (1.8)
8 (3.5)
17 (7.5)
10 (4.4)
1 (0.4)
6 (2.7)
7 (3.2)
7 (3.2)
3 (1.4)
0 (0.0)

Belatacept und HLA-Antikörper
95% CI MI: 0.28–3.95 LI: 0.84–5.36 CsA: 7.34–15.91
Specificity Bela MI Bela LI CsA
Total, n 3 7 25
Class I DSA, n 1 3 7
Class II DSA, n 2 4 14
Class I and II, n 0 0 4
Bray, ATC 2015

Belatacept und der G-BA
Probleme: IV-Gabe „Nur de novo zugelassen“ Marketing / Verfügbarkeit Jahrestherapiekosten: 13.602,49 €

Belatacept statt CNI

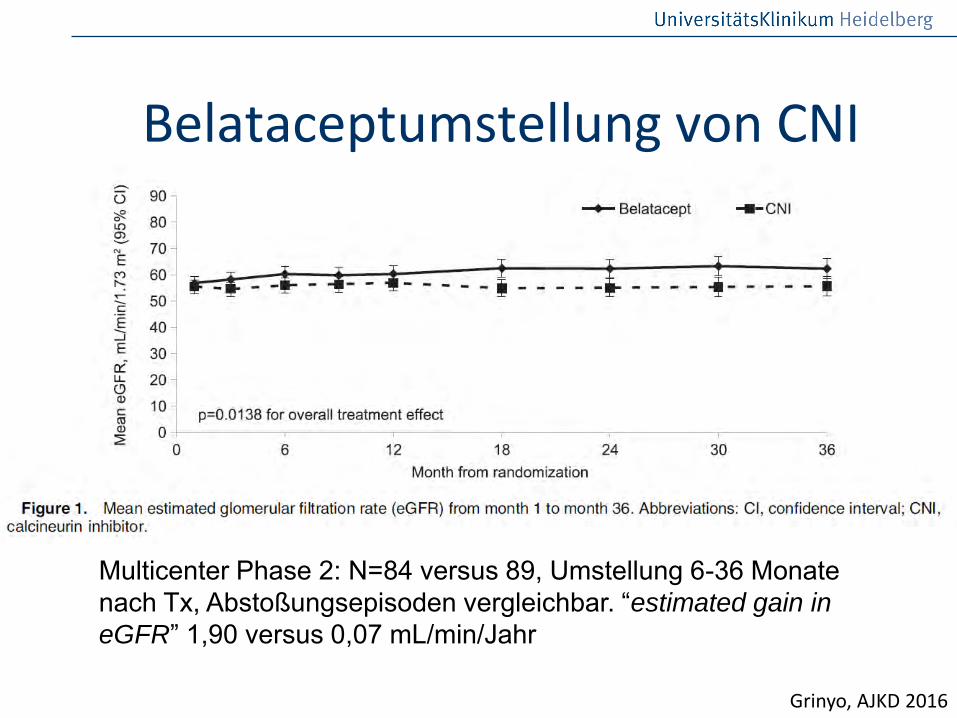
Belataceptumstellung von CNI
Le Meur, Am J Transplant 2016
F: N=25, Umstellung innerhalb der ersten 6 Monate nach Tx, 6 Pat. blieben dialysepflichtig, 3 Pat. mit Therapieversagen, 3 Pat. verstorben, restliche Pat. mit Anstieg der eGFR von 18,3 auf 34,9 mL/min
Belataceptumstellung von CNI
Grinyo, AJKD 2016
Multicenter Phase 2: N=84 versus 89, Umstellung 6-36 Monate nach Tx, Abstoßungsepisoden vergleichbar. “estimated gain in
eGFR” 1,90 versus 0,07 mL/min/Jahr
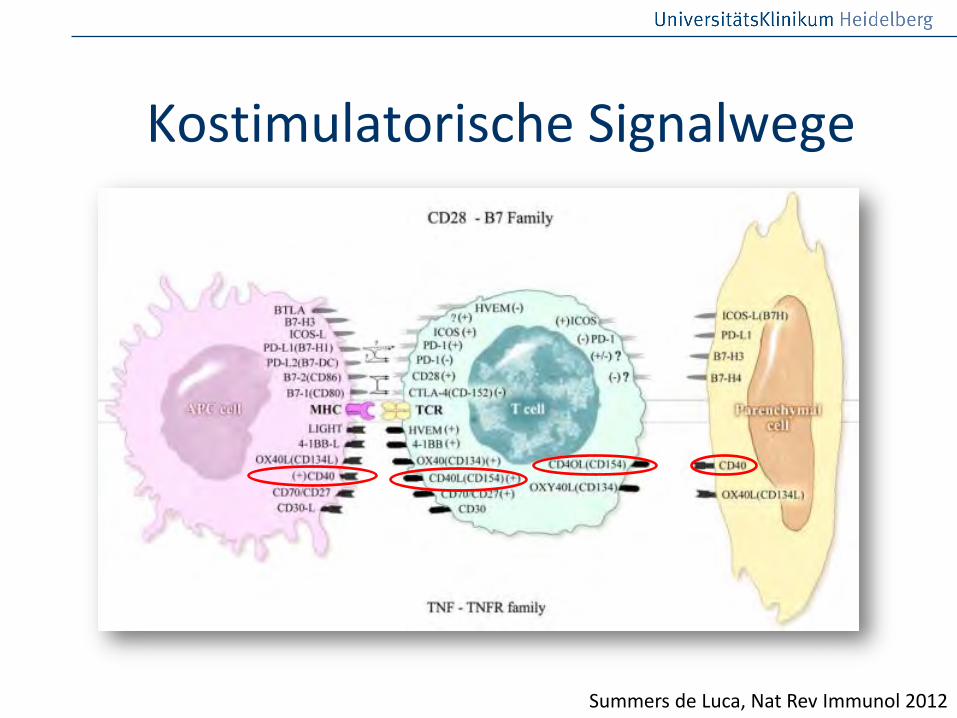
Kostimulatorische Signalwege
Summers de Luca, Nat Rev Immunol 2012

CD40-CD154 Interaktion
Adaptiert nach Mathur, 2006
Germinal center formation Ig isotype switching
anti-
CD40
CD40-CD154 Interaktion:
Zwischen B-Zellen, DCs, Monozyten, Makrophagen, Fibroblasten, Keratinozyten und aktivierten T & B Zellen
CD40-CD154 Defizienz:
Verhindert Abstoßung bei Nagern und Primaten

Cordoba, Am J Transplant 2015
(n=5)
(n=7)
*
CFZ533 Monotherapie verlängert Nierentransplantatüberleben in Primaten im Vergleich zu einem historischen Kontrollkollektiv
CFZ533

Cordoba, Am J Transplant 2015
-2 0 0 2 0 4 0 6 0 8 0 1 0 0 1 2 0
0
1 0 0
2 0 0
3 0 0
T im e (d a y s )
SC
re
a (
ml/l)
5 5 3 5
5 5 4 1
5 5 4 4
5 5 4 5
5 5 3 7
-2 0 0 2 0 4 0 6 0 8 0 1 0 0 1 2 0
0
1 0 0
2 0 0
3 0 0
T im e (d a y s )
SC
re
a (
ml/l)
5 5 3 5
5 5 4 1
5 5 4 4
5 5 4 5
5 5 3 7-2 0 0 2 0 4 0 6 0 8 0 1 0 0 1 2 0
0
1 0 0
2 0 0
3 0 0
T im e (d a y s )
SC
re
a (
ml/l)
5 5 3 5
5 5 4 1
5 5 4 4
5 5 4 5
5 5 3 7
-2 0 0 2 0 4 0 6 0 8 0 1 0 0 1 2 0
0
1 0 0
2 0 0
3 0 0
T im e (d a y s )
SC
re
a (
ml/l)
5 5 3 5
5 5 4 1
5 5 4 4
5 5 4 5
5 5 3 7
-2 0 0 2 0 4 0 6 0 8 0 1 0 0 1 2 0
0
1 0 0
2 0 0
3 0 0
T im e (d a y s p o s t tra n s p la n t )
SC
re
a (
ml/
l)
-2 0 0 2 0 4 0 6 0 8 0 1 0 0 1 2 0
0
1 0
2 0
3 0
4 0
T im e (d a y s p o s t tra n s p la n t )
SU
re
a (
mm
lol/
l)
*
CFZ533

CFZ533 in der klinischen Prüfung
• Phase I Studien sind abgeschlossen
• Aktuell findet eine Phase II Studie in der Nierentransplantation statt

Alternativen zu CNI
• mTOR (sequentiell): mehr Abstoßungen, mehr HLA-Antikörper?, bessere Nierenfunktion
• Kostimulationsblockade (de novo): mehr Abstoßungen, weniger ? HLA-Antikörper, bessere Nierenfunktion, besseres Langzeitüberleben ?
Einfluss auf das Transplantatüberleben ?

Weg zum Transplantatverlust Nonadhärenz und Unterimmunsuppression
Akute zelluläre Nierentransplantatabstoßung
Entwicklung von (de novo) Donor-spezifischen HLA Antikörpern
Akute oder chronische Antikörper-vermittelte Nierentransplantatabstoßung

• mTOR in Kombination mit niedrig-dosiert CNI bei z.B. BKV
• mTOR in Kombination mit MPA bei Tumoren?
• Belatacept (Umstellung) bei z.B. ah2 („CNI-Unverträglichkeit“)
• Belatacept in Zukunft auch vermehrt de novo?
Wie machen wir es ?

Zusammenfassung
• CNI ist und bleibt (noch?) Standard
• CNI auf jeden Fall bei immunologischen Risikokonstellationen (ABOi, HLA-AK)
• Umstellung auf mTOR, cave: HLA-Antikörper
• Umstellung auf Belatacept (logistische Probleme)
• De novo Belatacept bei niedrigem immunologischem Risiko
• Neue Substanzen!